Diphenhydramine as a Sleep Aid: How It Works, Safe Dosage, and Who Should Avoid It
A mechanistically rigorous guide to diphenhydramine — the active ingredient in ZzzQuil, Unisom SleepTabs, and Benadryl — covering how it induces sedation, what the FDA-approved dosage is, how quickly tolerance develops, and which populations face meaningful safety risks that OTC availability tends to obscure.

What Is Diphenhydramine and Which Products Contain It
Diphenhydramine is a first-generation antihistamine that has been used in the United States since the 1940s — originally for allergic reactions, hay fever, and motion sickness. Its tendency to cause drowsiness, a side effect in allergy contexts, became the basis for its second career as an OTC sleep aid.
Today it is the active ingredient in several of the most widely purchased sleep products on US pharmacy shelves:
- ZzzQuil (liquid and LiquiCaps) — Procter & Gamble
- Unisom SleepTabs — Chattem (note: Unisom SleepGels contain doxylamine, a different antihistamine)
- Benadryl (original formulation) — McNeil Consumer Healthcare
- Nytol and Sominex
- Advil PM and Tylenol PM (diphenhydramine combined with ibuprofen or acetaminophen, respectively)
The fact that these products are sold in the same aisle as vitamins and cold remedies creates a widespread impression that they are uniformly safe and appropriate for anyone who has trouble sleeping. That impression is incomplete. Diphenhydramine is a pharmacologically active drug with a specific mechanism, documented limitations on how long it remains useful, and meaningful safety risks for certain populations that OTC availability tends to obscure.
This article focuses specifically on diphenhydramine. Doxylamine (Unisom SleepGels), melatonin, and other OTC options have distinct mechanisms and risk profiles and are not covered here. The goal is to give adults considering or currently using diphenhydramine-containing products a clear, mechanistically grounded account of what the drug does, what it cannot do, and when it should not be used at all.
How Diphenhydramine Works: H1 Inverse Agonism and the Anticholinergic Co-Mechanism
The standard description — "diphenhydramine blocks histamine" — is technically incomplete in a way that matters for understanding both its sedative effect and its side effect profile.
Diphenhydramine acts as an inverse agonist at central histamine H1 receptors — not merely an antagonist. The distinction is meaningful: a simple antagonist blocks the receptor from being activated by histamine; an inverse agonist goes further, reversing the receptor's constitutive baseline activity and actively suppressing the histaminergic arousal system. The result is a more pronounced reduction in cortical wakefulness signals than simple receptor blockade alone would produce.
What allows diphenhydramine to reach central H1 receptors in the first place is its lipophilicity. Fat-soluble molecules cross the blood-brain barrier readily, and diphenhydramine is highly lipid-soluble. This is the defining difference between first-generation antihistamines like diphenhydramine and second-generation antihistamines like cetirizine (Zyrtec) or loratadine (Claritin) — the second-generation drugs were specifically engineered to be less lipophilic so they would not cause CNS sedation. Diphenhydramine was not.
In addition to H1 inverse agonism, diphenhydramine is a potent muscarinic receptor antagonist — it blocks acetylcholine at muscarinic receptors throughout the central and peripheral nervous system. This anticholinergic action contributes to sedation but is also the direct cause of most of the drug's characteristic side effects: dry mouth, urinary retention, constipation, blurred vision, and cognitive effects. The sedation you feel from diphenhydramine is therefore the product of two overlapping mechanisms, not one.
FDA-Approved OTC Dosage
The FDA OTC monograph for nighttime sleep-aid drug products specifies a clear dosage range. According to the StatPearls clinical monograph, the approved dose is 25–50 mg taken approximately 30 minutes before bedtime for adults and children 12 and older. This article does not recommend doses beyond these parameters.
| Population | Approved OTC Dose | Timing | Notes |
|---|---|---|---|
| Adults (18–64) | 25–50 mg | ~30 minutes before bedtime | Use the lowest effective dose; do not exceed 50 mg |
| Adults 65 and older | Not recommended | — | 2023 AGS Beers Criteria: avoid; see population safety section |
| Children 12–17 | 25–50 mg | ~30 minutes before bedtime | Use with caution; consult a clinician first |
| Children under 12 | Not approved for sleep use | — | Do not use diphenhydramine to sedate children under 12 |
| Pregnant individuals | Consult a clinician | — | Non-sedating antihistamines generally preferred |
| Breastfeeding individuals | Avoid high doses | — | High doses may decrease prolactin; consult a clinician |
What the Clinical Evidence Actually Shows
Several randomized controlled trials have examined diphenhydramine's efficacy as a sleep aid. The consistent finding is that it produces real, measurable improvements in sleep latency and subjective sleep quality compared to placebo — but only in the short term, and with a tolerance ceiling that arrives quickly.
| Study | Design | Key Finding | Duration of Benefit |
|---|---|---|---|
| Rickels et al. (1983) | Double-blind crossover, n=111 | Improved sleep latency and subjective restfulness vs. placebo | Short-term; tolerance not the primary focus |
| Morin et al. (2005) | Multicenter RCT, n=184 | Improved subjective sleep parameters and sleep efficiency in first 14 days | First 14 days; efficacy diminished thereafter |
| Schweitzer et al. (1994) | Controlled trial | Tolerance to sedative effects documented by day 3 of consecutive use | Efficacy window: approximately 2–3 days |
| Richardson et al. (2002) | Controlled trial | Tolerance by day 4; performance decline (next-day impairment) reversed by day 4 as tolerance developed | Efficacy window: approximately 3–4 days |
The most current structured expert synthesis is a 2025 Delphi consensus study by Ariza-Salamanca and colleagues, published in the Journal of Clinical Medicine (PMC12112657). A panel of five Latin American sleep specialists reached unanimous agreement (100% consensus) that diphenhydramine is effective for managing acute insomnia and for short-term insomnia of less than three months in adults aged 18–65. For adults 65 and older, no consensus was reached across three rounds of review — reflecting significant expert disagreement about its appropriateness in that population. The panel also unanimously agreed that diphenhydramine is not useful for chronic insomnia lasting more than three months.
Tolerance: Why It Stops Working Within Days
The most consequential limitation of diphenhydramine as a sleep aid is not a side effect — it is the speed at which the drug stops being effective.
When H1 receptors are persistently occupied by an inverse agonist, the brain responds by downregulating the number and sensitivity of those receptors — a compensatory adaptation that reduces the drug's functional impact. This is the mechanism behind tolerance to diphenhydramine's sedative effect, and it happens faster than most OTC consumers expect.
Schweitzer et al. (1994) documented tolerance to sedation by day 3 of consecutive nightly use. Richardson et al. (2002) found tolerance by day 4 — and notably, that the next-day performance impairment (psychomotor slowing, cognitive hangover) was also reversed by day 4 as tolerance developed. This is a useful data point: by the time the drug has stopped helping you sleep, it has also largely stopped impairing your daytime performance. But the implication is that you are left with neither the benefit nor a clear signal that the drug has stopped working.
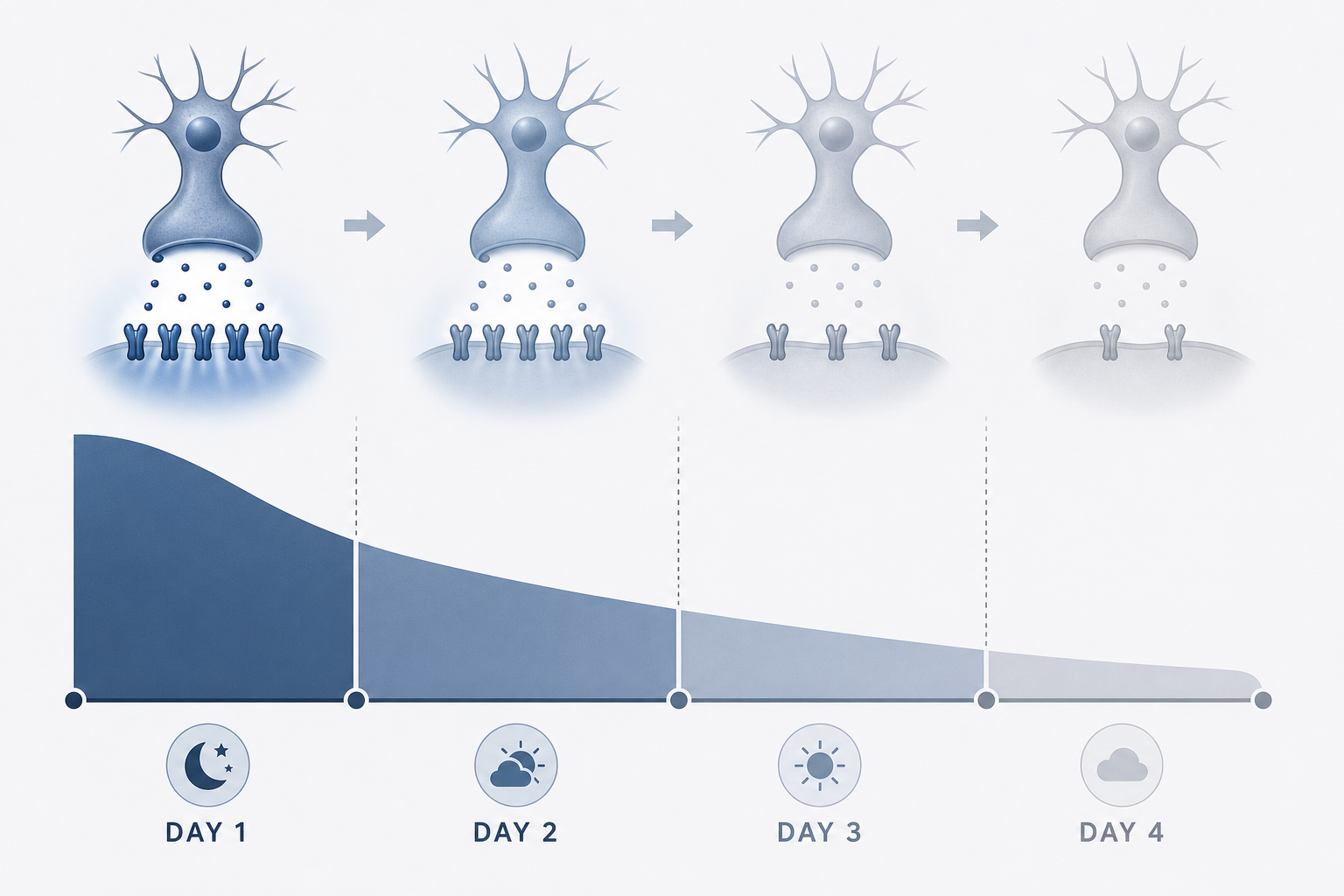
The 2025 expert consensus agreed that a maximum recommended treatment duration of approximately four weeks is appropriate — but also unanimously agreed that diphenhydramine is not useful for chronic insomnia. In practice, the clinical utility window for consecutive nightly use is likely measured in days, not weeks. Using it intermittently (not every night) extends the window by allowing receptor sensitivity to partially recover between uses.
Common Side Effects — and Why Each One Occurs
Diphenhydramine's side effects are not random — each one follows directly from either its anticholinergic mechanism or its pharmacokinetic profile. Understanding the mechanism makes the side effects more predictable and helps explain why they are more severe in certain populations.
- Next-day drowsiness and cognitive hangover: Diphenhydramine has a half-life of approximately 9 hours in healthy young adults. This means that if you take it at 11 PM, roughly half the drug is still active at 8 AM. The result is residual sedation, slowed reaction time, and impaired working memory that persists well into the following day. In elderly adults, the half-life extends to approximately 13.5 hours — compounding this risk substantially.
- Impaired psychomotor performance: Multiple controlled studies have documented impaired simulated driving performance the morning after a standard diphenhydramine dose. This is not a theoretical risk — it is a measured, dose-dependent effect that persists beyond the point at which most users feel subjectively alert.
- Dry mouth: Muscarinic blockade reduces salivary gland secretion. Saliva production is controlled by parasympathetic stimulation via M3 muscarinic receptors; diphenhydramine's anticholinergic action suppresses this pathway.
- Urinary retention: The bladder detrusor muscle contracts under parasympathetic (cholinergic) control to initiate urination. Muscarinic blockade impairs detrusor contraction, reducing the ability to fully empty the bladder. This side effect is particularly significant for men with benign prostatic hyperplasia (BPH), who already have compromised urinary flow.
- Constipation: Gastrointestinal motility is regulated in part by parasympathetic cholinergic signaling. Anticholinergic blockade slows gut motility, resulting in constipation with regular use.
- Blurred vision: Muscarinic blockade at the ciliary muscle of the eye impairs accommodation (the ability to focus on near objects) and can dilate the pupil by blocking the pupillary sphincter muscle. This is why diphenhydramine is contraindicated in closed-angle glaucoma — pupil dilation can precipitate an acute attack by narrowing the trabecular drainage angle.
Serious and Overdose Risks
At therapeutic doses, diphenhydramine's risks are manageable for most healthy adults in the short term. At higher doses — whether from intentional misuse, accidental combination of multiple products, or individual pharmacokinetic sensitivity — the risks become serious and potentially life-threatening.
Diphenhydramine prolongs the cardiac QT interval through two distinct mechanisms: blockade of sodium channels and inhibition of the hERG potassium channel (the delayed rectifier potassium channel responsible for cardiac repolarization). Prolonged QT can progress to torsades de pointes, a form of ventricular tachycardia that can degenerate into ventricular fibrillation. Brugada-like EKG pattern changes have also been documented in overdose cases.
At high doses, the full anticholinergic toxidrome can develop: delirium, hallucinations, hyperpyrexia (dangerously elevated body temperature), urinary retention, seizures, and cardiovascular collapse. The clinical management of severe anticholinergic toxidrome includes physostigmine (a cholinesterase inhibitor that reverses central anticholinergic effects) and sodium bicarbonate for QRS prolongation.
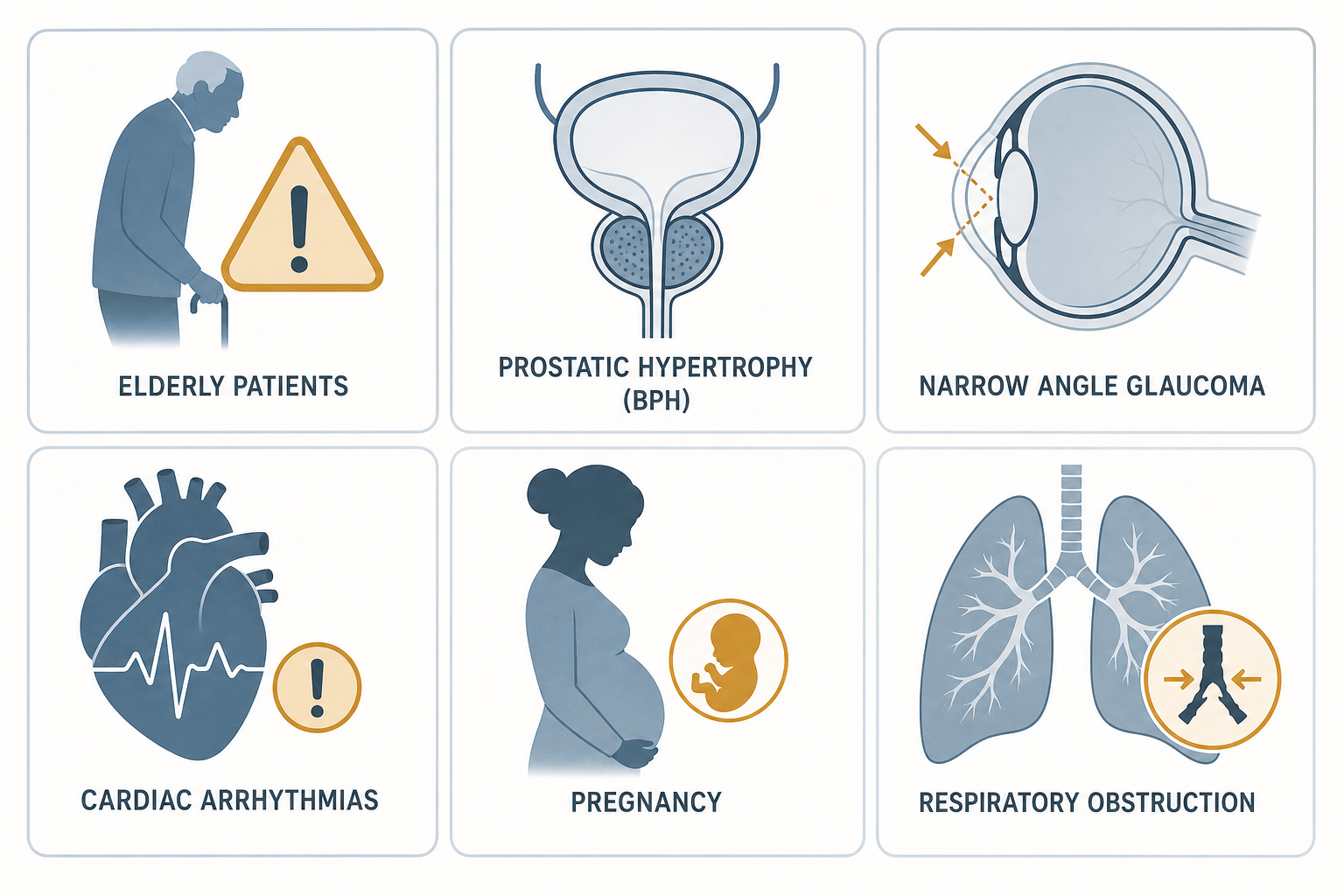
Who Should Not Use Diphenhydramine: Population-Specific Safety Warnings
OTC availability does not mean universal safety. Several populations face meaningful risks from diphenhydramine that are not adequately communicated by standard product labeling.
| Population | Risk Level | Rationale | Guideline Source |
|---|---|---|---|
| Adults 65 and older | AVOID — Strong recommendation | Reduced drug clearance (half-life ~13.5 h vs. ~9.2 h in younger adults); highly anticholinergic; tolerance develops as hypnotic; elevated risk of confusion, delirium, falls, and fractures; dementia association with cumulative anticholinergic burden | 2023 AGS Beers Criteria (Strong recommendation, Moderate evidence quality) |
| Men with BPH or urinary retention | AVOID | Muscarinic blockade impairs detrusor muscle contraction, worsening urinary flow obstruction and increasing urinary retention risk | 2023 Beers Criteria (Table 3: Lower urinary tract symptoms/BPH) |
| Closed-angle glaucoma | AVOID | Anticholinergic-induced pupil dilation can precipitate acute angle-closure attack by narrowing the trabecular drainage angle | Contraindicated per FDA labeling and clinical guidelines |
| Asthma or COPD | Use with caution / Avoid | Anticholinergic effects increase bronchial secretion viscosity, potentially worsening airway obstruction | Clinical contraindication; consult clinician |
| Pre-existing cardiac conditions | Use with caution / Avoid | QT prolongation via hERG channel blockade and sodium channel blockade; risk of torsades de pointes | StatPearls; 2025 expert consensus |
| Concurrent anticholinergic medications | AVOID combining | Additive anticholinergic burden increases risk of cognitive decline, delirium, and falls; Beers Criteria explicitly warns against combining multiple anticholinergic agents | 2023 Beers Criteria (Table 5) |
| Pregnancy | Consult a clinician | Safety data are limited; non-sedating antihistamines are generally preferred; consult a healthcare provider before use | MedlinePlus; clinical guidance |
| Breastfeeding | Avoid high doses | High doses may decrease prolactin levels and potentially impact lactation; non-sedating antihistamines are preferred | StatPearls (NBK526010) |
The concern about dementia risk in older adults warrants careful framing. A 10-year prospective cohort study (Gray et al., JAMA Internal Medicine, 2015) found that cumulative anticholinergic drug use equivalent to three or more years of continuous exposure was associated with a 54% higher incidence of dementia compared to minimal or no anticholinergic use. This finding is referenced in both the 2023 AGS Beers Criteria and the 2025 expert consensus.
Drug Interactions
Diphenhydramine interacts with several drug classes in ways that range from additive sedation to life-threatening toxicity. The interactions below reflect the categories with the strongest clinical evidence and the most practical relevance for OTC users.
| Drug / Drug Class | Interaction Type | Clinical Consequence | Guidance |
|---|---|---|---|
| Alcohol | Additive CNS depression | Significantly increased sedation, respiratory depression risk, severely impaired psychomotor performance | Explicitly contraindicated — never combine |
| Benzodiazepines (e.g., diazepam, lorazepam) | Additive CNS depression | Compounded sedation and respiratory depression; increased fall and overdose risk | Avoid concurrent use |
| Z-drugs (zolpidem, eszopiclone) | Additive CNS depression | Compounded sedation; increased next-day impairment | Avoid concurrent use |
| Opioids | Additive CNS and respiratory depression | Substantially elevated risk of respiratory depression and overdose | Avoid concurrent use |
| MAO inhibitors (MAOIs) | Prolongs and intensifies anticholinergic effects | Increased risk of anticholinergic toxidrome; enhanced sedation | Contraindicated; do not use within 14 days of MAOI |
| Other anticholinergic drugs (TCAs, bladder antimuscarinics, benztropine, trihexyphenidyl, hydroxyzine, chlorpromazine, olanzapine) | Additive anticholinergic burden | Increased risk of cognitive decline, delirium, urinary retention, falls, and fractures | Avoid combining; review total anticholinergic burden |
| Antipsychotics (chlorpromazine, olanzapine) | Additive anticholinergic and CNS depressant effects | Increased sedation and anticholinergic toxicity risk | Avoid concurrent use without clinician guidance |
| Multiple diphenhydramine-containing products simultaneously | Direct dose stacking | Risk of overdose; cardiac and neurological toxicity | FDA-required labeling warning since 2002 — never combine |
What Clinical Guidelines Say — and When to Seek Professional Help
The American Academy of Sleep Medicine (AASM) Clinical Practice Guideline is unambiguous on this point: clinicians should not use diphenhydramine for sleep onset or sleep maintenance insomnia. This recommendation is cited directly in the StatPearls clinical monograph on diphenhydramine and reflects the AASM's 2017 guideline position, which cited poor effectiveness and low quality of evidence as the basis for the recommendation against use.
The first-line evidence-based treatment for chronic insomnia — defined as difficulty sleeping three or more nights per week for three or more months — is Cognitive Behavioral Therapy for Insomnia (CBT-I). CBT-I addresses the behavioral, cognitive, and physiological drivers of chronic insomnia through structured components including sleep restriction, stimulus control, and cognitive restructuring. It produces durable improvements that persist after treatment ends — something no OTC sleep aid can offer.
Short-term OTC diphenhydramine use may be reasonable in a narrow set of circumstances: a healthy adult aged 18–64 with no contraindicated conditions, experiencing brief acute insomnia driven by a clear situational stressor (travel, a stressful life event, temporary schedule disruption), who needs one to three nights of assistance falling asleep while the stressor resolves. Even in this context, a clinician at Baylor College of Medicine has noted that consulting a physician before using any pharmacological sleep aid is advisable rather than defaulting to OTC options.
All content on this site is educational and does not substitute for professional clinical evaluation. If you have questions about whether diphenhydramine is appropriate for your specific situation, consult a healthcare provider.
Key Takeaways
- What diphenhydramine is: An FDA-approved OTC sleep aid — the active ingredient in ZzzQuil, Unisom SleepTabs, Benadryl, Nytol, Sominex, Advil PM, and Tylenol PM — that works through H1 inverse agonism and muscarinic receptor blockade.
- What it can do: Reduce sleep latency and improve subjective sleep quality in healthy adults aged 18–65 for brief, acute insomnia. RCT evidence supports short-term efficacy.
- What it cannot do: Provide restorative sleep (it reduces REM), treat chronic insomnia, or maintain its sedative effect beyond a few nights of consecutive use.
- Tolerance timeline: Tolerance to the sedative effect develops within 3–4 days of consecutive nightly use due to H1 receptor downregulation. Intermittent use extends the window; nightly consecutive use does not.
- The half-life problem: A ~9-hour half-life in adults means the drug is still substantially active the next morning. Documented next-day psychomotor impairment — including impaired simulated driving — is a real risk, not a theoretical one.
- Who should not use it: Adults 65 and older (2023 AGS Beers Criteria: Strong recommendation to avoid), men with BPH, individuals with closed-angle glaucoma, asthma/COPD, pre-existing cardiac conditions, concurrent anticholinergic medication burden, and those who are pregnant or breastfeeding.
- The AASM guideline position: The American Academy of Sleep Medicine recommends against using diphenhydramine for chronic insomnia. CBT-I is the evidence-based first-line treatment for chronic insomnia.
- Never combine with alcohol: The combination of diphenhydramine and alcohol produces additive CNS depression and is explicitly contraindicated.
- Never combine multiple products: Advil PM, Tylenol PM, ZzzQuil, and Benadryl all contain diphenhydramine. Taking more than one simultaneously risks overdose.
Explore the mechanism
Next step
Spot an error or have clinical feedback?
Because this article covers clinical, medication, or safety information, we use a moderated correction channel instead of open public comments. Let us know if something about “Diphenhydramine as a Sleep Aid: How It Works, Safe Dosage, and Who Should Avoid It” needs a closer look.
Send feedback on this article