Magnesium Glycinate for Sleep: Evidence, Dosage, Timing, and Safety Compared to Other Forms
An evidence-anchored explainer for adults who have encountered magnesium glycinate as a sleep aid recommendation and want an honest assessment — covering what the clinical trials actually show, how glycinate compares to other magnesium forms, how to dose it correctly, who is most likely to benefit, and where it fits relative to first-line insomnia treatments.

What Magnesium Glycinate Is — and Why It Became the Popular Sleep Form
Magnesium glycinate is a chelated compound: one magnesium ion bound to two glycine molecules. Because each magnesium ion carries two glycine carriers, the more precise chemical name is magnesium bisglycinate — and the two terms appear interchangeably throughout the research literature. When you see a study testing "magnesium bisglycinate," it is testing the same compound sold under the "glycinate" label on most supplement shelves.
The chelate structure matters for absorption. Magnesium oxide and magnesium sulfate are inorganic salts that dissolve poorly in liquid and pass through the gut largely unabsorbed. Organic forms — those bound to an amino acid or organic acid — dissolve more completely in the aqueous environment of the small intestine, which gives the body a larger window to absorb the magnesium before it reaches the colon.
The NIH Office of Dietary Supplements confirms that magnesium in the aspartate, citrate, lactate, and chloride forms is absorbed more completely and is more bioavailable than magnesium oxide and magnesium sulfate. Glycinate sits in the same organic-form category.
Beyond absorption, the glycine carrier is not biologically inert. Glycine is an inhibitory amino acid with its own sleep-relevant mechanisms — a point that becomes important when evaluating the clinical trials, because the two components cannot be cleanly separated in a bisglycinate capsule.
How Magnesium and Glycine May Support Sleep: The Biological Pathways
The mechanistic case for magnesium glycinate as a sleep aid rests on two separate sets of pathways — one set driven by magnesium itself, and one set driven by the glycine carrier. Understanding both matters, because they are why bisglycinate is theoretically the most interesting magnesium form for sleep, and also why the clinical trials cannot tell us which component is doing the work.
Magnesium's Four Sleep-Relevant Pathways
- NMDA receptor blockade. Magnesium ions act as voltage-dependent blockers of NMDA (N-methyl-D-aspartate) receptors — the same receptors that drive neuronal excitability and arousal. By reducing NMDA-mediated signaling, magnesium may dampen the kind of cortical hyperarousal that keeps people awake.
- GABA receptor potentiation. Magnesium enhances the activity of GABA (gamma-aminobutyric acid) receptors, the brain's primary inhibitory signaling system. Greater GABAergic tone reduces neuronal firing rates and promotes the transition into sleep.
- Melatonin synthesis support. Magnesium can enhance the activity of serotonin N-acetyltransferase, an enzyme critical for converting serotonin into melatonin. It also appears to reduce serum cortisol concentrations, which otherwise suppress melatonin secretion and maintain a state of physiological alertness.
- Circadian rhythm regulation. Intracellular magnesium concentrations rise and fall within a 24-hour rhythm, playing a role in cellular circadian timekeeping. Disruption of this flux may contribute to circadian misalignment.
Glycine's Independent Contributions
Glycine is not simply a delivery vehicle. It has two sleep-relevant mechanisms of its own:
- Core body temperature reduction. Glycine promotes peripheral vasodilation — widening of blood vessels near the skin — which accelerates heat dissipation and lowers core body temperature. Falling core temperature is one of the body's key physiological signals for initiating sleep onset.
- Inhibitory glycine receptor agonism. Glycine acts on inhibitory glycine receptors in the central nervous system, producing effects that are mechanistically distinct from GABA potentiation but similarly suppressive of neuronal excitability.
What the Clinical Evidence Actually Shows
The mechanistic pathways above explain why researchers have investigated magnesium for sleep. They do not establish that supplementation works in practice. The clinical evidence is considerably more modest than the popular narrative suggests — and reading it carefully requires working through several layers of quality problems.
The NCCIH Position
The National Center for Complementary and Integrative Health states plainly that there is very little research on magnesium supplements for insomnia and other sleep disorders, and there isn't enough rigorous scientific evidence to determine whether they are effective. This is the federal agency responsible for evaluating complementary health approaches — not a skeptical outlier.
The Mah and Pitre 2021 Systematic Review
A 2021 systematic review by Mah and Pitre searched the literature for randomized controlled trials of magnesium supplementation for insomnia in older adults. After applying eligibility criteria, only three trials qualified — involving a combined 151 participants. The reviewers rated the evidence as low to very low quality. The pooled estimate suggested magnesium might reduce sleep-onset latency by approximately 16 minutes, but this finding was statistically non-significant. The reviewers explicitly stated the studies were inadequate for making well-informed clinical decisions.
Three trials with 151 participants is a thin foundation for the level of confidence that magnesium-for-sleep recommendations typically carry.
The Schuster 2025 Bisglycinate RCT — in Full
The most recent and most directly relevant trial tested magnesium bisglycinate specifically in adults with insomnia symptoms. It is the best available evidence for the specific form this article covers — and it deserves to be read carefully rather than summarized as simply "positive."
Participants in the magnesium group saw their Insomnia Severity Index (ISI) score drop by 3.9 points over the course of the trial. That sounds meaningful until you account for the placebo group, whose ISI score dropped by 2.3 points on its own — without any active supplement. The net difference attributable to the magnesium bisglycinate was 1.6 points on a 28-point scale.
The study itself defined a clinically meaningful improvement as a 6-point drop on the ISI. By that threshold — the study's own threshold — 81% of participants taking magnesium bisglycinate did not achieve meaningful benefit. There were no statistically significant changes on any of the eight secondary outcomes measured.
An independent analysis of the trial data concluded that approximately 59% of the improvement observed in the magnesium group was attributable to the placebo effect, not the supplement itself. The effect size for magnesium was d=0.2 — a small effect by conventional standards.
The Oxide Problem in the Broader Literature
Most of the trials that have reported positive findings for magnesium and sleep used magnesium oxide — a form the NIH ODS confirms is poorly absorbed by the digestive tract. This creates a paradox: the most "positive" evidence in the literature was generated using the least bioavailable form. If the body barely absorbs oxide, the mechanism by which it would improve sleep is unclear, and the positive findings may reflect confounding factors rather than genuine magnesium activity.
Extrapolating from oxide trials to glycinate — or assuming glycinate will perform better because it absorbs better — is a logical step, but it is not supported by direct evidence. No magnesium sleep study has been published in Sleep or the Journal of Clinical Sleep Medicine, the field's two highest-tier journals.
Magnesium Forms Compared: Glycinate, Citrate, Oxide, L-Threonate, and Malate
Choosing a magnesium form involves trade-offs across bioavailability, gastrointestinal tolerance, and the availability of sleep-specific evidence. The table below summarizes the key dimensions for the five forms most commonly marketed for sleep.
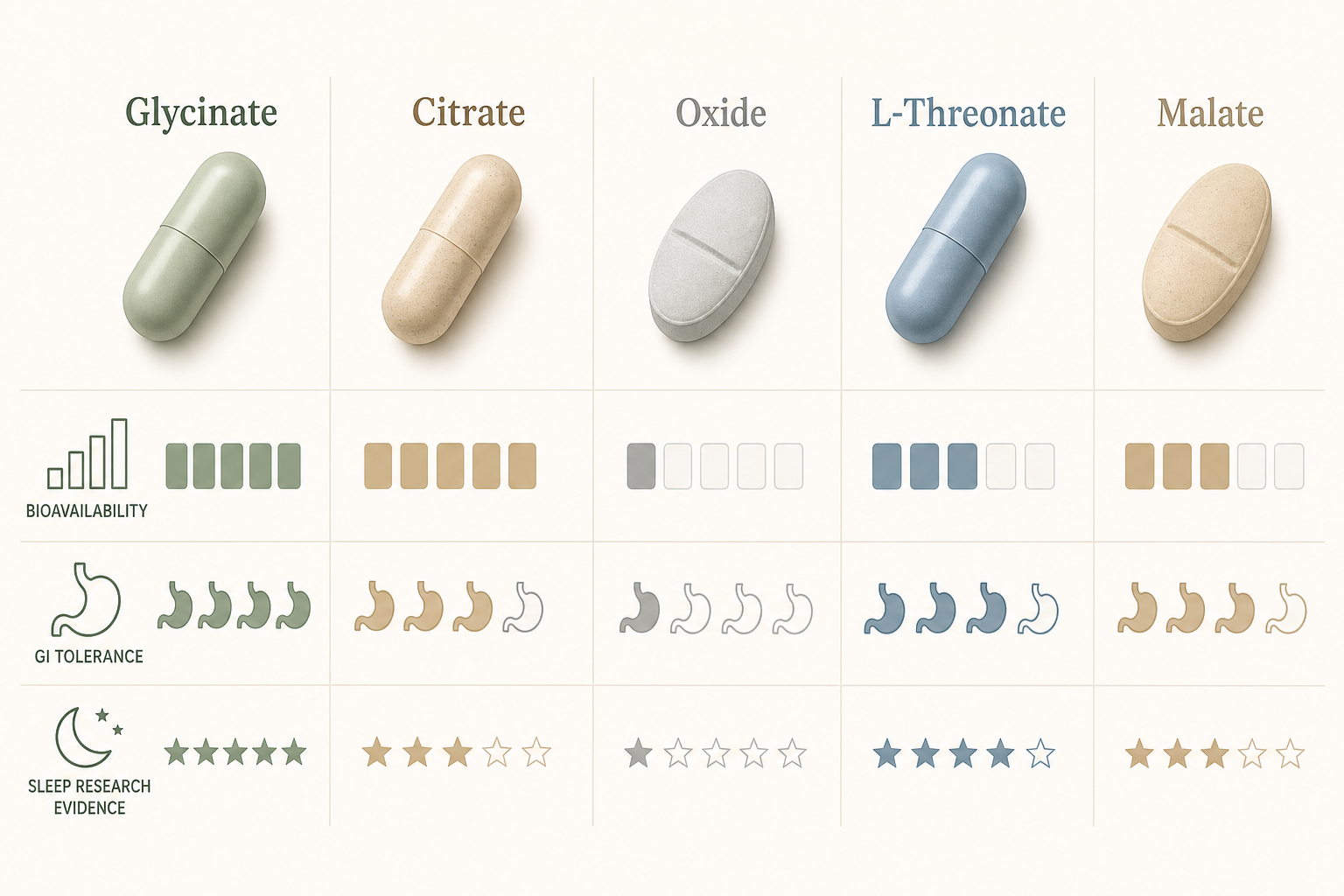
| Form | Bioavailability | GI Tolerance / Laxative Risk | Sleep-Specific Trial Evidence | Best-Fit Use Case |
|---|---|---|---|---|
| Glycinate (bisglycinate) | High — organic chelate, dissolves well in liquid | Very good — lowest GI side-effect rate of common forms | One RCT (Schuster 2025): 1.6-point net ISI improvement; glycine confound limits attribution | Sleep support, GI-sensitive users, those who have experienced diarrhea on other forms |
| Citrate | High — among the most bioavailable forms per NIH ODS | Moderate — natural laxative effect at higher doses | Some positive trials; not bisglycinate-specific; laxative effects complicate high-dose use | General supplementation; users without GI sensitivity; constipation as a secondary concern |
| Oxide | Low — poorly absorbed by the digestive tract | Generally tolerable at lower doses; high doses cause diarrhea | Dominates the positive sleep literature — but low bioavailability undermines interpretation | Not recommended for sleep or deficiency correction; used mainly for digestive symptom relief |
| L-Threonate | Moderate systemically; theoretically higher CNS penetration in animal research | Generally well tolerated | Hausenblas 2024: between-group difference driven by placebo group declining, not treatment group improving — methodological concern | Theoretical CNS advantage unproven in sleep RCTs; insufficient evidence to recommend over glycinate for sleep |
| Malate | High — well absorbed | Good — low laxative risk | No sleep-specific RCTs identified | General supplementation; energy metabolism support; reasonable choice if glycinate unavailable |
Dosage: Elemental Magnesium vs. Compound Weight
One of the most common errors people make when dosing magnesium is confusing the weight of the entire compound with the amount of elemental magnesium it contains.
The NIH ODS is explicit on this point: the Supplement Facts panel on a dietary supplement label declares the amount of elemental magnesium in the product, not the weight of the entire magnesium-containing compound. So if a label reads "400 mg magnesium (as magnesium glycinate)," the 400 mg refers to elemental magnesium — not to the total weight of the glycinate compound, which would be substantially higher.
This matters because some products list compound weight rather than elemental content in their marketing copy, even if the Supplement Facts panel is accurate. A capsule containing 2,000 mg of magnesium glycinate compound might deliver only 200 mg of elemental magnesium.
| Reference Value | Amount | Applies To |
|---|---|---|
| Adult RDA (men 19–30) | 400 mg elemental Mg/day | All sources combined (food + supplements) |
| Adult RDA (men 31+) | 420 mg elemental Mg/day | All sources combined |
| Adult RDA (women 19–30) | 310 mg elemental Mg/day | All sources combined |
| Adult RDA (women 31+) | 320 mg elemental Mg/day | All sources combined |
| Tolerable Upper Intake Level (adults 19+) | 350 mg elemental Mg/day | Supplements and medications only — does not apply to food |
| Commonly cited sleep-support range | 200–400 mg elemental Mg | Supplements only; start at the lower end |
The adult RDA covers total intake from all sources. If your diet already provides 300 mg of magnesium daily from food — which is plausible with a reasonably varied diet — a 200 mg supplement brings your total to 500 mg, which exceeds the RDA but remains below the UL ceiling for supplemental magnesium. The UL of 350 mg applies only to supplements and medications, not to dietary magnesium, because the kidneys efficiently excrete excess magnesium from food in healthy individuals.
Timing: When to Take It Before Bed
The most commonly recommended window is 30 to 60 minutes before your intended sleep time. This timing is consistent with the Schuster 2025 trial protocol and with clinical guidance from practitioners who recommend magnesium for sleep support.
The rationale connects to the mechanisms described earlier. The NMDA receptor blockade and GABA potentiation effects require the magnesium to be absorbed and circulating — which takes time after an oral dose. Glycine's core body temperature-lowering effect via cutaneous vasodilation also needs time to develop before the body enters the sleep-onset window.
Taking magnesium with a small amount of food can reduce the likelihood of GI discomfort, though glycinate is generally well tolerated even on an empty stomach. Avoid taking it at the same time as certain medications — the interaction timing requirements are covered in the next section.
Safety, Contraindications, and Drug Interactions
Magnesium glycinate has a favorable safety profile in healthy adults at recommended doses — but "generally safe" does not mean universally safe. Several specific populations and medication combinations require attention.
The Kidney Disease Contraindication
Drug Interactions
Magnesium interacts with several common medication classes in ways that affect either the medication's absorption or the body's magnesium balance:
| Medication Class | Interaction Mechanism | Practical Guidance |
|---|---|---|
| Bisphosphonates (e.g., alendronate, risedronate) | Magnesium-rich supplements decrease absorption of oral bisphosphonates | Take bisphosphonate at least 2 hours before or after magnesium supplement |
| Tetracycline antibiotics (e.g., doxycycline, minocycline) | Magnesium forms insoluble complexes with tetracyclines, reducing antibiotic absorption | Take antibiotic 2–6 hours before or after magnesium supplement |
| Quinolone antibiotics (e.g., ciprofloxacin, levofloxacin) | Same mechanism as tetracyclines — complex formation reduces antibiotic bioavailability | Take antibiotic 2–6 hours before or after magnesium supplement |
| Loop diuretics (e.g., furosemide) and thiazide diuretics (e.g., hydrochlorothiazide) | Increase urinary magnesium excretion, contributing to deficiency | Supplementation may be warranted but should be guided by a clinician monitoring serum levels |
| Proton pump inhibitors / PPIs (e.g., omeprazole, pantoprazole) | Long-term use causes hypomagnesemia; supplements sometimes fail to correct levels adequately | Long-term PPI users should have magnesium levels monitored; supplementation alone may not be sufficient |
Population-Specific Safety Notes
- Older adults. Magnesium intake tends to be lower in older populations, and the gut absorbs it less efficiently with age. Renal excretion also increases. Combined with the higher likelihood of polypharmacy — particularly diuretics and PPIs — older adults face elevated risk of both deficiency and of interactions. Supplementation should be discussed with a clinician, and the dose should be conservative.
- Pregnant individuals. The RDA for magnesium during pregnancy is higher than for non-pregnant adults of the same age group (350 mg for ages 19–30; 360 mg for ages 31–50). The supplemental UL of 350 mg/day applies equally during pregnancy. Because pregnancy involves significant physiological changes that affect nutrient metabolism, any supplementation during pregnancy should be discussed with an OB/GYN rather than self-managed.
- Children. Pediatric dosing requirements differ substantially from adult requirements. There is no established evidence for magnesium glycinate as a pediatric sleep aid. Consult a pediatrician before giving any magnesium supplement to a child.
Who Is Most Likely to Benefit
The honest answer to "will magnesium glycinate help my sleep?" depends significantly on your baseline magnesium status. The supplement is most plausibly useful for people who are not getting enough magnesium from their diet — a larger group than most people assume.
An analysis of NHANES 2013–2016 data found that 48% of Americans of all ages consume less magnesium than their Estimated Average Requirement. Subclinical deficiency — insufficient intake without overt clinical symptoms — is the plausible context in which correcting magnesium status might produce sleep improvements.
Risk Factors for Low Magnesium Status
- Diet high in processed foods and low in whole grains, legumes, nuts, and leafy greens — the primary dietary sources of magnesium
- Chronic psychological stress, which increases urinary magnesium excretion
- Regular alcohol consumption, which impairs magnesium absorption and increases renal excretion
- Type 2 diabetes, which is associated with increased renal magnesium losses
- Gastrointestinal disorders affecting absorption (Crohn's disease, celiac disease, chronic diarrhea)
- Long-term use of PPIs or loop/thiazide diuretics, as described in the interactions section
- Older age, due to reduced gut absorption and increased renal excretion
Observational data from the CARDIA cohort — a longitudinal study of nearly 4,000 young American adults — found that higher magnesium intake was associated with a 36% lower likelihood of short sleep duration. Critically, this association was observed only among participants without depressive disorders — it was not found in those with depression. This suggests the relationship between magnesium and sleep is not universal and may be moderated by underlying mental health status.
For someone with genuinely adequate magnesium intake from a varied whole-food diet and no risk factors for depletion, the case for supplementation is weaker. The supplement is unlikely to produce meaningful sleep improvements in a person who is already replete.
Where Magnesium Fits in the Treatment Hierarchy
If you have chronic insomnia — difficulty sleeping three or more nights per week for three or more months — the evidence hierarchy is unambiguous. Cognitive Behavioral Therapy for Insomnia (CBT-I) is the first-line treatment endorsed by the American Academy of Sleep Medicine (AASM) and the American College of Physicians. It is not one option among several; it is the treatment with the strongest evidence base for chronic insomnia.
The numbers make the gap concrete. CBT-I produces effect sizes of d=1.0 to 1.5 on the Insomnia Severity Index. The best available estimate for magnesium supplementation is d=0.2. Behavioral therapy is five to seven times more effective for chronic insomnia than magnesium supplementation — and unlike supplements, CBT-I produces durable improvements that persist after treatment ends.
This does not mean magnesium glycinate has no place. For people with subclinical magnesium deficiency, stress-driven sleep disruption, or risk factors that deplete magnesium status, it is a low-risk adjunct worth considering — particularly given its favorable safety profile, minimal GI side effects, and the dual mechanism from both magnesium and glycine. The framing that fits the evidence is: a reasonable supplement to add to a broader sleep strategy, not a standalone insomnia treatment.
When to Consult a Clinician
- Your sleep difficulties have persisted for three or more months, occurring most nights — this meets the threshold for chronic insomnia, which warrants clinical evaluation and CBT-I referral.
- You have chronic kidney disease or any condition affecting renal function — magnesium supplementation requires physician oversight.
- You take bisphosphonates, tetracycline or quinolone antibiotics, loop or thiazide diuretics, or long-term PPIs — interaction management may be needed.
- You are pregnant — supplementation during pregnancy should be discussed with your OB/GYN, not self-managed.
- You are an older adult taking multiple medications — the combination of polypharmacy risk and reduced renal clearance warrants a clinician's input before starting any new supplement.
- Your sleep disruption is accompanied by mood changes, excessive daytime sleepiness, witnessed apneas, or significant anxiety — these may indicate a condition requiring a different diagnosis and treatment approach.
Explore the mechanism
Next step
Spot an error or have clinical feedback?
Because this article covers clinical, medication, or safety information, we use a moderated correction channel instead of open public comments. Let us know if something about “Magnesium Glycinate for Sleep: Evidence, Dosage, Timing, and Safety Compared to Other Forms” needs a closer look.
Send feedback on this article