Valerian Root for Sleep: Evidence, Dosage, and Safety
A balanced, evidence-based assessment of valerian root as a sleep aid — covering how it works, what the clinical research actually shows (including why the evidence is mixed), dosage guidance, formulation quality issues, and population-specific safety cautions for adults weighing this dietary supplement against its inconsistent clinical record.

The Popularity–Evidence Gap
Valerian root is among the top-selling herbal supplements in the United States, marketed widely for sleep and relaxation. It appears on pharmacy shelves, in health food stores, and in countless online recommendations. Yet its regulatory status tells a different story: valerian is classified as a dietary supplement by the FDA — not an approved drug. That distinction matters in a specific, practical way: unlike drugs, dietary supplements are not reviewed by the FDA for safety or efficacy before they reach consumers. No pre-market approval is required, and no manufacturer is obligated to demonstrate that the product works.
That gap between popularity and regulatory scrutiny is worth holding in mind as you read through the evidence. Two anchor findings set the tone for this assessment. First, a 2024 umbrella review published in European Neuropsychopharmacology — analyzing eight eligible systematic reviews — found that valerian has a good safety profile but no evidence of efficacy for the treatment of diagnosable insomnia. Second, the American Academy of Sleep Medicine's 2017 clinical practice guideline issued a weak recommendation against valerian for chronic insomnia. Neither of these findings is buried in fine print — they are the operative clinical standards as of mid-2026.
This does not make valerian a dangerous or worthless supplement. It does mean that an honest assessment requires understanding why the evidence is mixed — including formulation instability problems and the gap between how patients report their sleep versus what objective measurements show — rather than simply accepting a dosage recommendation at face value.
What Valerian Root Is
Valerian refers to preparations derived from Valeriana officinalis, a flowering perennial plant native to Europe and Asia and now cultivated widely in North America. The medicinal preparations use the root and underground stem (rhizome), not the flower. Valerian has been used as a calming and sleep-promoting agent since at least the second century CE and became particularly popular in 17th-century Europe as a remedy for nervousness and insomnia.
Today it is available in several forms:
- Dried root or rhizome in capsule or tablet form (whole-root preparations)
- Hydroalcoholic extracts, standardized to valerenic acid content
- Aqueous (water-based) extracts
- Tinctures (alcohol-based liquid extracts)
- Herbal teas, typically made from dried root
The form matters — not just as a consumer preference, but as a scientific variable that directly affects what the clinical research shows. More on that shortly.
How Valerian Is Proposed to Work
Valerian does not work through a single mechanism. Researchers have identified at least three distinct pharmacological pathways, each associated with different constituent compounds. Understanding these pathways also explains why preparation type — whole root versus extract — produces such different outcomes in clinical trials.
The most studied pathway involves valerenic acid and valerenol, which are fat-soluble (lipophilic) compounds found in the root. These compounds act as allosteric modulators of GABA-A receptors, specifically at the beta-3 subunit — the same receptor family targeted by benzodiazepines and barbiturates, though through a different binding site and with far weaker effect. This GABA-A modulation is the most commonly cited mechanism and the one most extract standardization efforts are built around.
A second pathway involves hydrophilic (water-soluble) lignan constituents in the root, which act as partial agonists at adenosine A1 receptors. Adenosine signaling plays a central role in the buildup of sleep pressure across the day — it is the same system that caffeine blocks. This pathway is relevant specifically to water-soluble fractions of the root, which are more concentrated in whole-root preparations than in lipophilic extracts.
A third pathway involves partial agonist activity at serotonin 5-HT5A receptors, demonstrated for both valerian extract and valerenic acid. The functional significance of this pathway for sleep specifically is less well characterized than the GABA-A and adenosine mechanisms.
The practical implication of this multi-pathway, polarity-dependent picture is that different preparations deliver different constituent profiles. A hydroalcoholic extract standardized to valerenic acid will be rich in lipophilic constituents but may be relatively depleted of the hydrophilic lignan fractions that drive adenosine activity. Whole-root preparations preserve a broader constituent range. This is not a minor manufacturing detail — it is a core reason why clinical trials using different formulations produce different results.
Why the Evidence Is Mixed: Formulation and Measurement Problems
Before presenting the clinical data, it is worth naming the two structural problems that make valerian trials difficult to interpret. These are not excuses for weak evidence — they are explanations for why the same supplement can produce contradictory findings across studies.
Problem 1: Valepotriate Instability
Valepotriates are a class of active compounds found in fresh valerian root that were once considered primary candidates for its sedative effects. They are, however, thermolabile — they break down rapidly with heat and storage. Research cited in the 2020 systematic review and meta-analysis found that valepotriate levels in stored extracts fell to less than 5% of their original content after just two months at room temperature. Valerenic acid levels, by contrast, were unaffected by the same storage conditions.
This means that a product standardized only to valerenic acid content may have lost most of its valepotriate fraction by the time a consumer uses it — and a clinical trial using such a product is not testing the same constituent profile as one using fresh whole root. When extract-based trials fail to show benefit, valepotriate degradation is one plausible explanation.
Problem 2: Subjective vs. Objective Sleep Measurement
Clinical sleep research uses two fundamentally different types of outcome measures. Subjective measures — patient-reported sleep quality ratings, questionnaires, sleep diaries — capture how a person feels about their sleep. Objective measures — polysomnography (PSG), actigraphy — capture physiological sleep parameters such as sleep onset latency, wake after sleep onset (WASO), and sleep stage distribution.
Valerian appears to influence these two types of outcomes differently. The 2024 umbrella review noted that valerian may produce subjective improvement in sleep quality — patients report sleeping better — but this improvement has not been confirmed by objective polysomnographic measurements. That divergence is not a minor statistical footnote. It means valerian may change how sleep feels without measurably changing the underlying sleep architecture, latency, or efficiency that PSG captures.
What the Clinical Research Shows
Two large evidence syntheses form the backbone of what we currently know about valerian's efficacy and safety. They reach different conclusions, but those conclusions are not contradictory — they reflect different scopes of inquiry.
The 2020 Systematic Review and Meta-Analysis
The 2020 review analyzed 60 studies involving 6,894 participants across a wide age range (7–80 years) and a broad spectrum of sleep-related complaints — not limited to diagnosable insomnia. Key findings:
- No serious adverse events were reported across any study or age group.
- In subgroup meta-analysis, whole-root and rhizome preparations showed a combined effect size of Hedges g = 0.83 (95% CI: 0.03–1.62) — a moderate-to-large effect, though with a wide confidence interval.
- Extract-based preparations showed a much smaller effect size of Hedges g = 0.10 (95% CI: −0.02–0.22) — not statistically distinguishable from placebo.
- Single-dose studies produced weak and inconsistent results; the pattern for positive outcomes was repeated use over 4–8 weeks.
- Whole-root preparations at 450–1,410 mg/day for 4–8 weeks consistently showed sleep quality improvements; extracts at 300–600 mg/day for 5 days to 4 weeks produced inconsistent outcomes.
The 2024 Umbrella Review
The 2024 umbrella review in European Neuropsychopharmacology took a narrower focus: it analyzed 8 eligible systematic reviews specifically addressing valerian for diagnosable insomnia as a clinical condition. Its conclusions were clear:
"Data suggested that valerian has a good safety profile, however, the results showed no evidence of efficacy for the treatment of insomnia. Valerian appears to be effective concerning subjective improvement of sleep quality, although its effectiveness has not been demonstrated with quantitative or objective measurements."
The authors concluded that valerian does not have empirical support for insomnia despite its widespread use and prescription by general practitioners and psychiatrists.
Why These Two Reviews Are Not Contradictory
The 2020 review included a broad range of sleep-related problems, formulation types, and populations — some participants had diagnosable insomnia, many did not. The whole-root subgroup advantage it identified is a real signal, but it is drawn from a heterogeneous population. The 2024 umbrella review specifically asked: does valerian work for diagnosable insomnia? Its answer — no — applies to that specific clinical question.
Taken together, the evidence suggests: valerian may improve how some people with mild, situational sleep difficulties feel about their sleep, particularly with whole-root preparations used over several weeks. It does not appear to produce clinically meaningful, objectively confirmed improvements in insomnia as a diagnosable sleep disorder.
| Review | Scope | Key Finding | Safety Finding |
|---|---|---|---|
| 2020 Systematic Review & Meta-Analysis (60 studies, n=6,894) | Broad sleep problems; multiple formulations; ages 7–80 | Whole-root: Hedges g=0.83; extract: g=0.10; single doses ineffective; 4–8 weeks of repeated use for positive outcomes | No serious adverse events across any study or age group |
| 2024 Umbrella Review (8 systematic reviews) | Diagnosable insomnia specifically | No evidence of efficacy for insomnia; subjective improvement possible but not confirmed by objective measures | Good safety profile confirmed |
What Clinical Guidelines Recommend
The American Academy of Sleep Medicine's 2017 clinical practice guideline — the first to provide comprehensive, evidence-based analyses of individual sleep agents — reviewed valerian alongside 13 other agents. It issued a weak recommendation against valerian for both sleep-onset and sleep-maintenance insomnia in adults. "Weak" in AASM guideline terminology reflects lower certainty in the evidence, not a minor or dismissible finding — it means the available data did not support recommending the supplement for clinical use.
The same guideline reiterates CBT-I as the initial evidence-based intervention for chronic insomnia and states that sleep medications — including supplements — should be considered mainly for patients who cannot participate in CBT-I, who still have symptoms after completing it, or who need a temporary adjunct. Supplements are not positioned as a first-line or equivalent alternative.
The National Center for Complementary and Integrative Health (NCCIH) aligns with this position: it describes the evidence on valerian for sleep as inconsistent and states there is not enough to recommend it. The NCCIH also notes that the safety of long-term valerian use remains unknown.
| Authority | Position on Valerian | First-Line Recommendation |
|---|---|---|
| AASM (2017 Clinical Practice Guideline) | Weak recommendation against for sleep-onset and sleep-maintenance insomnia | CBT-I |
| NCCIH (Updated 2025) | Evidence inconsistent; not enough to recommend | Clinical evaluation; CBT-I for chronic insomnia |
| 2024 European Neuropsychopharmacology Umbrella Review | No evidence of efficacy for diagnosable insomnia | Not applicable (research review, not clinical guideline) |
Dosage and Timing
The dosage ranges cited across clinical literature depend on the preparation type. For hydroalcoholic extracts, the commonly referenced range is 300–600 mg daily. For whole-root or rhizome preparations, positive-outcome studies used 450–1,060 mg daily (some studies extended to 1,410 mg). Timing is consistently 30–120 minutes before bedtime.
A critical practical point: single doses are unlikely to produce meaningful effects. The consistent pattern in studies showing positive outcomes is repeated use over 4–8 weeks. If you try valerian once and notice little effect, that is consistent with the evidence — not a reason to double the dose.
Why Product Standardization Is Not Straightforward
Many commercial valerian products are labeled as "standardized to 0.8% valerenic acid" — a common quality benchmark. The problem is that valerenic acid is only one of valerian's active constituents. Standardizing to valerenic acid alone does not guarantee the presence of the hydrophilic lignan fractions (adenosine A1 activity) or adequate valepotriate content — and as noted above, valepotriates degrade rapidly in stored extracts regardless of valerenic acid levels.
The subgroup data from the 2020 meta-analysis suggests that whole-root preparations — which preserve a broader constituent range — are more consistent with the positive-outcome studies than extract-only products. This does not mean every whole-root product is superior, but it does mean that valerenic acid standardization alone is not a reliable quality proxy.
For quality assurance, look for products that have been independently verified by third-party certification programs such as USP, NSF International, or ConsumerLab. These programs test for label accuracy, contamination, and disintegration — they do not certify efficacy, but they provide meaningful quality assurance that the product contains what the label claims.
| Preparation Type | Typical Dosage Range | Timing | Evidence Pattern |
|---|---|---|---|
| Whole root / rhizome | 450–1,060 mg/day (some trials to 1,410 mg) | 30–120 min before bed | More consistent positive outcomes in 4–8 week trials |
| Hydroalcoholic extract | 300–600 mg/day | 30–120 min before bed | Inconsistent outcomes; extract subgroup effect size near zero in meta-analysis |
| Single dose (either form) | Any | Before bed | Weak evidence; repeated use over weeks is the consistent pattern |
Safety Profile and Known Side Effects
Across the 60 studies included in the 2020 systematic review — spanning participants aged 7 to 80 — no serious adverse events were reported. The 2024 umbrella review confirmed this finding: valerian has a good safety profile for short-term use. The NCCIH notes that valerian has been used with apparent safety at doses of 300–600 mg daily for up to 6 weeks.
Known mild side effects include:
- Headache
- Gastrointestinal upset (stomach discomfort, nausea)
- Vivid dreams
- Drowsiness or mental dullness the following morning
- Excitability or uneasiness (paradoxical stimulant effect in some individuals)
In very rare cases, liver injury has been reported in association with valerian use — but most documented cases involved combination herbal products rather than valerian alone. Causality in these cases is difficult to establish, and isolated valerian at standard doses has not been consistently linked to hepatotoxicity in controlled studies.
One additional caution applies to prolonged use: there are anecdotal reports of withdrawal-like symptoms (increased anxiety, agitation) after stopping valerian following extended regular use. The clinical evidence base for this is limited, but it is a reasonable precaution to taper rather than stop abruptly after several months of consistent use.
Drug Interactions
Valerian's interaction profile involves two distinct categories that must not be collapsed into a single risk assessment.
Pharmacokinetic (CYP Enzyme) Interactions: Low Risk
Multiple human trials have shown that valerian has no significant inhibitory or inductive effects on CYP1A2, CYP2D6, CYP2E1, or CYP3A4 — the major cytochrome P450 enzymes responsible for metabolizing most prescription medications. This finding, documented in a 2017 review in American Family Physician, means that valerian is unlikely to meaningfully alter the blood levels of drugs metabolized by these enzymes. This is a genuinely reassuring finding for pharmacokinetic interaction risk.
Pharmacodynamic (CNS Depressant) Interactions: Clinically Meaningful
Low CYP interaction risk does not mean valerian is interaction-free. The pharmacodynamic category — additive effects from combining valerian with other substances that depress the central nervous system — is a separate and clinically important concern.
Combining valerian with any of the following can produce additive sedation, impaired coordination, and increased risk of respiratory depression:
- Alcohol
- Benzodiazepines (e.g., lorazepam, diazepam, clonazepam)
- Opioid pain medications
- Antihistamines with sedative properties (e.g., diphenhydramine, doxylamine)
- Barbiturates
- Other herbal sedatives (e.g., kava, passionflower)
| Interaction Type | Risk Level | Mechanism | Clinical Implication |
|---|---|---|---|
| CYP enzyme (pharmacokinetic) | Low | No significant inhibition or induction of CYP1A2, 2D6, 2E1, or 3A4 in human trials | Unlikely to alter blood levels of most prescription drugs |
| CNS depressants (pharmacodynamic) | Clinically meaningful | Additive sedation via overlapping CNS depression pathways | Consult clinician before combining with alcohol, benzodiazepines, opioids, antihistamines, or barbiturates |
Population-Specific Cautions
Valerian's safety record in healthy adults does not extend uniformly across all populations. The following groups require specific consideration.
| Population | Recommendation | Rationale |
|---|---|---|
| Pregnant women | Not recommended | Insufficient safety data; potential uterotonic effects have been raised in animal studies; the risk-benefit calculation does not support use without clinical guidance |
| Breastfeeding women | Not recommended | Insufficient data on transfer to breast milk and infant effects |
| Elderly adults (65+) | Use with caution; consult clinician | Limited data in this age group; additive sedation potential raises fall risk, particularly if taking other CNS-active medications |
| Children under age 3 | Avoid | No safety data; not appropriate for this age group |
| Children ages 3 and older | Limited data; clinical guidance recommended | The 2020 review included subjects as young as age 7 with no serious adverse events, but this does not constitute a general pediatric endorsement; clinical guidance is appropriate before use in children |
| Adults with anxiety or depression | Consult clinician | Limited data on interactions with anxiolytic or antidepressant medications; potential for pharmacodynamic interactions with serotonergic agents |
A Practical Decision Framework
Given everything above, here is a structured way to think through whether valerian root is appropriate for your situation — without prescribing an outcome.
When It Is Reasonable to Consider
- Your sleep difficulty is mild and situational — related to a stressful period, travel, or a temporary disruption — rather than a chronic, persistent pattern.
- You are a healthy adult without contraindicated medications (CNS depressants, benzodiazepines, opioids, antihistamines) or conditions.
- You are willing to use it consistently over 4–8 weeks rather than expecting single-dose results.
- You are not pregnant, breastfeeding, elderly with fall risk, or under age 3.
- You understand this is a low-risk, low-certainty option — not a proven treatment.
How to Choose a Quality Product
- Look for third-party tested products verified by USP, NSF International, or ConsumerLab — these programs confirm label accuracy and test for contaminants.
- Whole-root or rhizome preparations are more consistent with the positive-outcome clinical evidence than extract-only products standardized solely to valerenic acid.
- Do not rely on valerenic acid standardization alone as a quality proxy — it does not account for valepotriate content or the hydrophilic lignan fractions.
- Check storage conditions — valepotriates degrade rapidly at room temperature. Products stored or shipped in warm conditions may have reduced constituent activity.
When to Stop and Seek Care
- Your sleep problems persist beyond 2–4 weeks of consistent valerian use without improvement.
- Your sleep difficulties are worsening, chronic (lasting more than three months), or accompanied by significant daytime impairment.
- You experience any new side effects — particularly unusual liver-related symptoms (jaundice, right-side abdominal pain, dark urine), which should prompt immediate medical evaluation.
- You have been using valerian for more than 6–12 weeks continuously and want to stop — consider tapering gradually rather than stopping abruptly.
Valerian Within the Insomnia Treatment Hierarchy
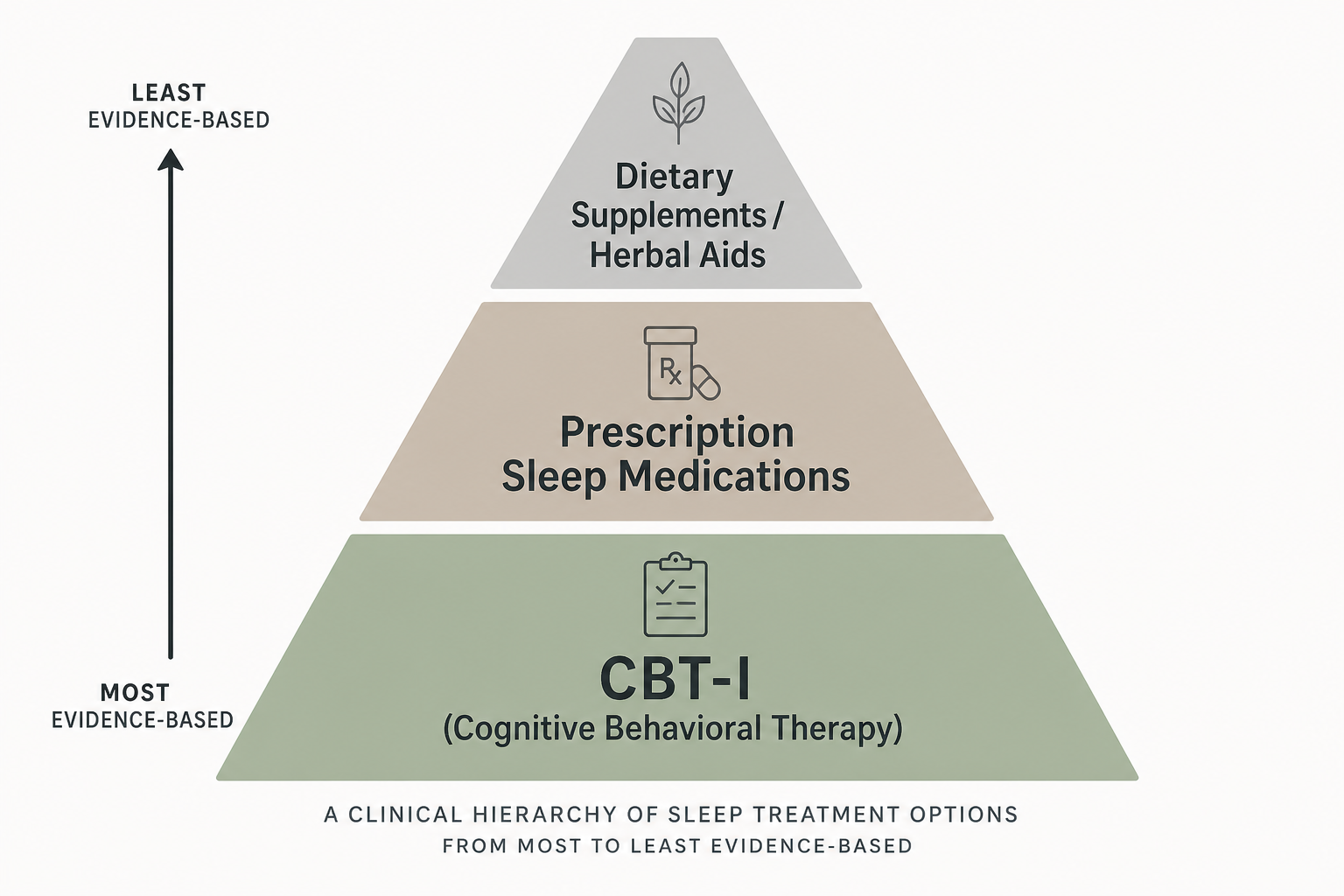
Valerian's appropriate place in the insomnia treatment hierarchy is at the top of the pyramid — the smallest tier, representing the lowest certainty and the most limited evidence. The AASM guideline is explicit: cognitive behavioral therapy for insomnia (CBT-I) is the initial evidence-based intervention for chronic insomnia. Supplements should be considered only when CBT-I is unavailable, insufficient after a full course, or used as a short-term adjunct — not as an equivalent or first-choice alternative.
CBT-I addresses the behavioral, cognitive, and physiological drivers of insomnia — stimulus control, sleep restriction, sleep hygiene, and cognitive restructuring — through a structured, evidence-based protocol. It produces durable improvements in sleep that persist after treatment ends, which is not a characteristic of any supplement currently on the market, including valerian.
For mild, situational sleep difficulty in a healthy adult — the scenario where valerian has the most reasonable risk-benefit profile — the evidence suggests it is a low-risk option with modest and inconsistent efficacy. It may improve how you feel about your sleep without necessarily changing the underlying sleep architecture. That is a meaningful distinction, and it is the most accurate summary of what the current evidence actually shows.
Explore the mechanism
Next step
Spot an error or have clinical feedback?
Because this article covers clinical, medication, or safety information, we use a moderated correction channel instead of open public comments. Let us know if something about “Valerian Root for Sleep: Evidence, Dosage, and Safety” needs a closer look.
Send feedback on this article