Chronic Insomnia Disorder: Definition, Causes, Diagnosis, and Treatment
A structured clinical reference for adults who suspect their persistent sleep difficulty may meet the diagnostic threshold for chronic insomnia disorder — covering ICSD-3 criteria, the behavioral and neurobiological mechanisms that sustain it, how it is properly diagnosed, and why CBT-I is the guideline-recommended first-line treatment.

What Is Chronic Insomnia Disorder?
Chronic insomnia disorder is a clinically defined condition — not a description of a few rough nights or a stretch of poor sleep. The International Classification of Sleep Disorders, Third Edition (ICSD-3) sets a specific threshold: difficulty initiating sleep, maintaining sleep continuity, or experiencing nonrestorative sleep, occurring three or more nights per week for more than three months, despite having adequate time and opportunity for sleep, and producing clinically meaningful daytime impairment. The DSM-5 uses the same core thresholds.
That daytime impairment criterion is not a footnote — it is a required part of the diagnosis. Difficulty sleeping that leaves a person fully functional during the day does not meet the diagnostic standard for chronic insomnia disorder. This distinction matters because it separates a clinical condition from the broader experience of sleeping less than one would like.
Symptoms: Nighttime and Daytime
Chronic insomnia disorder presents across two distinct dimensions. The nighttime experience is what most people recognize, but the daytime consequences are equally part of the clinical picture — and required for diagnosis.
Nighttime symptoms typically include one or more of the following:
- Difficulty falling asleep at the start of the night (prolonged sleep onset latency)
- Waking in the middle of the night and struggling to return to sleep
- Waking earlier than intended and being unable to fall back asleep
- Lying awake for extended periods during what should be the sleep period
Daytime consequences — which must be present to meet diagnostic criteria — commonly include:
- Fatigue or low energy (distinct from daytime sleepiness, which is more characteristic of sleep apnea or hypersomnia)
- Impaired concentration, attention, or working memory
- Mood disturbance, irritability, or emotional reactivity
- Reduced performance at work, school, or in daily tasks
- Increased accident risk
- Ongoing worry or preoccupation about sleep — which, as discussed below, also functions as a maintaining factor
The relationship between nighttime symptoms and daytime consequences is not simply one of cause and effect. Worry about sleep, anticipatory anxiety before bedtime, and rumination about the previous night's sleep are not just byproducts of insomnia — they are active mechanisms that sustain it.
How Common Is Chronic Insomnia Disorder?
Prevalence figures for insomnia vary widely depending on what is being measured — and that distinction is clinically important. Roughly 30–43% of adults report experiencing at least one insomnia symptom. But meeting the full diagnostic criteria for chronic insomnia disorder is considerably rarer.
Applying strict ICSD-3 or DSM-5-TR criteria, approximately 6–10% of adults meet the threshold for chronic insomnia disorder. A 2024 survey commissioned by the American Academy of Sleep Medicine found that 12% of U.S. adults reported a formal diagnosis. A Spanish general-population study applying the full ICSD-3 criteria stepwise — including all exclusions and diagnostic notes — found a prevalence of 14%, with higher rates among women (14.6%) and adults aged 55 and older (17.9%).
| Measurement | Prevalence | Notes |
|---|---|---|
| At least one insomnia symptom | ~30–43% | Symptom prevalence; does not meet disorder criteria |
| Chronic insomnia disorder (ICSD-3/DSM-5-TR strict criteria) | 6–10% | Requires nighttime symptoms + daytime impairment + ≥3 months duration |
| Self-reported formal diagnosis (U.S. adults) | ~12% | AASM 2024 survey of 2,006 U.S. adults |
| Full ICSD-3 criteria applied stepwise (Spanish population) | ~14% | Higher in women and adults 55+ |
Certain groups carry a disproportionately higher risk: women, adults aged 55 and older, shift workers, and those with comorbid psychiatric or medical conditions. Once insomnia progresses to a disorder, it tends not to resolve on its own. A naturalistic five-year study found that 37.5% of participants with insomnia continued to report it at each annual follow-up — a persistence rate that underscores why understanding the mechanisms of chronicity is not merely academic.
Why Insomnia Becomes Chronic: The 3P Model and Hyperarousal
The most important thing to understand about chronic insomnia disorder is that the original stressor — the event that first disrupted sleep — is usually no longer the reason the insomnia continues. What sustains it is something else entirely.
The 3P model, developed by Arthur Spielman, provides the most widely used framework for understanding this progression. It describes three categories of factors that interact over time:
- Predisposing factors — traits and vulnerabilities present before insomnia begins, including neuroticism, a tendency toward heightened physiological arousal, lower stress resilience, and genetic factors concentrated in emotion-regulation circuits rather than core sleep-regulation genes. These set a baseline threshold for how easily sleep can be disrupted.
- Precipitating factors — the stressor or event that launches the episode: a job loss, a relationship breakdown, a medical illness, a major life change. These explain why insomnia started when it did.
- Perpetuating factors — the behaviors, beliefs, and cognitive patterns that sustain insomnia long after the precipitating stressor has passed. These are what transform an acute sleep disruption into a chronic disorder.
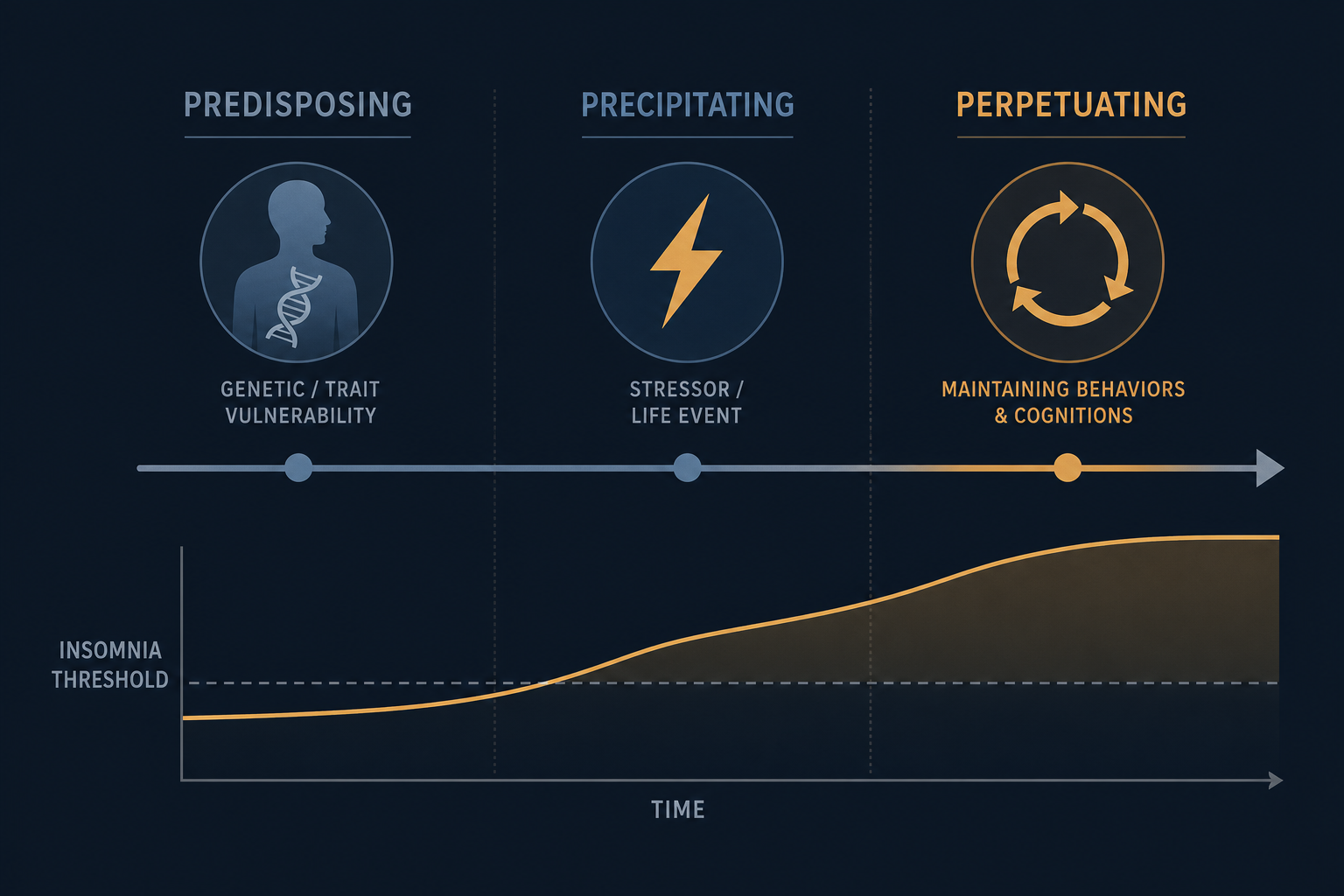
Common perpetuating factors include spending more time in bed to compensate for lost sleep (which paradoxically reduces sleep pressure and fragments sleep further), daytime napping, clock-watching during the night, catastrophizing about the consequences of poor sleep, and what researchers call affective sleep preoccupation — the worry and rumination about sleep that becomes its own arousal stimulus.
This is not just theoretical. A prospective study by Ellis and colleagues tested the 3P model empirically during the acute insomnia phase and found that only three baseline factors predicted whether insomnia persisted rather than naturally remitting: prior insomnia episode history, depression scores, and — most notably — higher affective sleep preoccupation. The original stressor was not the predictor. The worry about sleep was.
The Neurobiological Core: Hyperarousal and Conditioned Arousal
Beneath the behavioral patterns of perpetuating factors lies a neurobiological mechanism: hyperarousal. This refers to a state of elevated physiological, cognitive, and cortical activation that persists into the sleep period — the opposite of the quiet disengagement from the environment that sleep requires.
The brain's sleep-wake system operates something like a flip-flop switch: circuits promoting wakefulness and circuits promoting sleep suppress each other, creating a stable transition between states. In chronic insomnia, this switch is disrupted by simultaneous co-activation of both systems during the intended sleep period — neither fully wins, and the result is the frustrating middle state of lying awake, exhausted but unable to sleep.
A second mechanism compounds this: conditioned arousal. Through repeated association of the bed and bedroom with wakefulness, frustration, and anxiety — rather than with sleep — these environmental cues become learned triggers for arousal. The bedroom itself begins to activate the arousal system. This is not a metaphor; it is a well-documented learned response, and it is the mechanism that stimulus control therapy — one of CBT-I's core components — is specifically designed to break.
Risk Factors and Causes
Chronic insomnia disorder does not arise from a single cause. The 3P model's three categories map onto distinct types of contributing factors.
Predisposing traits — present before insomnia begins — include neuroticism, a tendency toward heightened physiological arousal, and polygenic risk concentrated in emotion-regulation circuits. Notably, the genetic architecture of insomnia vulnerability does not appear to involve the core sleep-regulation genes. This helps explain why people with insomnia often do not feel sleepy during the day the way someone with sleep deprivation would — the underlying biology is different.
Precipitating events that commonly trigger an initial episode include:
- Major psychosocial stressors — job loss, relationship breakdown, bereavement, significant life transitions
- Acute medical illness or hospitalization
- Changes in sleep environment or schedule
Conditions that elevate risk or complicate the clinical picture include:
- Depression and anxiety disorders — which have a bidirectional relationship with insomnia, not a simple cause-and-effect relationship
- Chronic pain conditions, which disrupt sleep continuity
- COPD, GERD, and other medical conditions that produce nighttime symptoms
- Obstructive sleep apnea — which can coexist with insomnia and requires separate evaluation
- Medications that disrupt sleep architecture (certain antidepressants, corticosteroids, stimulants, beta-blockers)
- Shift work and irregular schedules, which create chronic circadian misalignment
Health Consequences and Comorbidities
Untreated chronic insomnia disorder carries meaningful downstream health risks — not just the immediate functional impairments of fatigue and cognitive difficulty, but longer-term associations with serious medical and psychiatric conditions.
The relationship with depression and anxiety is among the most clinically significant. Approximately 66% of people with depression also have insomnia. Compared to those without insomnia, people with the disorder are roughly five times more likely to develop anxiety or depression. Individuals with chronic insomnia are estimated to be 40 times more likely to develop severe depressive disorder than those without insomnia. And people with persistent insomnia carry a roughly twofold increased risk of developing depression compared to those whose insomnia has remitted or been treated — a finding that underscores the importance of treating insomnia directly, not waiting for the mood disorder to resolve first.
Cardiovascular and metabolic consequences are supported by meta-analytic epidemiological evidence. Chronic insomnia — particularly when accompanied by objectively short sleep duration, which researchers use as a marker of physiological hyperarousal — is associated with incident hypertension, type 2 diabetes, heart failure, stroke, and all-cause mortality. The mechanism is thought to involve dysregulation of the HPA axis, increased sympathetic nervous system activation, and elevated inflammatory markers — all consequences of chronic hyperarousal. A 2025 review in Circulation Research summarized this meta-analytic evidence and noted that randomized trials have not yet demonstrated whether treating insomnia with CBT-I or pharmacotherapy directly improves cardiovascular outcomes — an important distinction between association and causation.
How Chronic Insomnia Is Diagnosed
Diagnosis rests on self-reported symptoms and clinical history — not on laboratory testing. There is no blood test or brain scan that diagnoses chronic insomnia disorder. A clinician will typically conduct a structured interview covering sleep patterns, daytime functioning, symptom duration, and potential contributing factors.
The sleep diary is the standard clinical tool. Kept for 7–14 days, it captures nightly sleep onset time, wake times, time out of bed, and subjective sleep quality — providing the pattern data needed to characterize the insomnia and establish a baseline before treatment begins.
Several validated self-report scales are commonly used:
| Scale | Items | Score Range | Clinical Thresholds |
|---|---|---|---|
| Insomnia Severity Index (ISI) | 7 items | 0–28 | ≥8: subthreshold; ≥15: moderate-to-severe; ≥22: severe. A change of ≥8 points indicates clinically meaningful improvement. |
| Pittsburgh Sleep Quality Index (PSQI) | 19 items | 0–21 | Score >5 indicates poor sleep quality |
| Epworth Sleepiness Scale (ESS) | 8 items | 0–24 | Used to assess daytime sleepiness; high scores may suggest a comorbid condition such as sleep apnea |
Clinically, the diagnostic thresholds that guide assessment align with the ICSD-3 criteria: sleep latency greater than 30 minutes, wake after sleep onset greater than 30 minutes, sleep efficiency below 85%, or total sleep time below 6–6.5 hours — occurring three or more nights per week for three or more months, with daytime impairment.
Treatment: CBT-I First, Pharmacotherapy Second
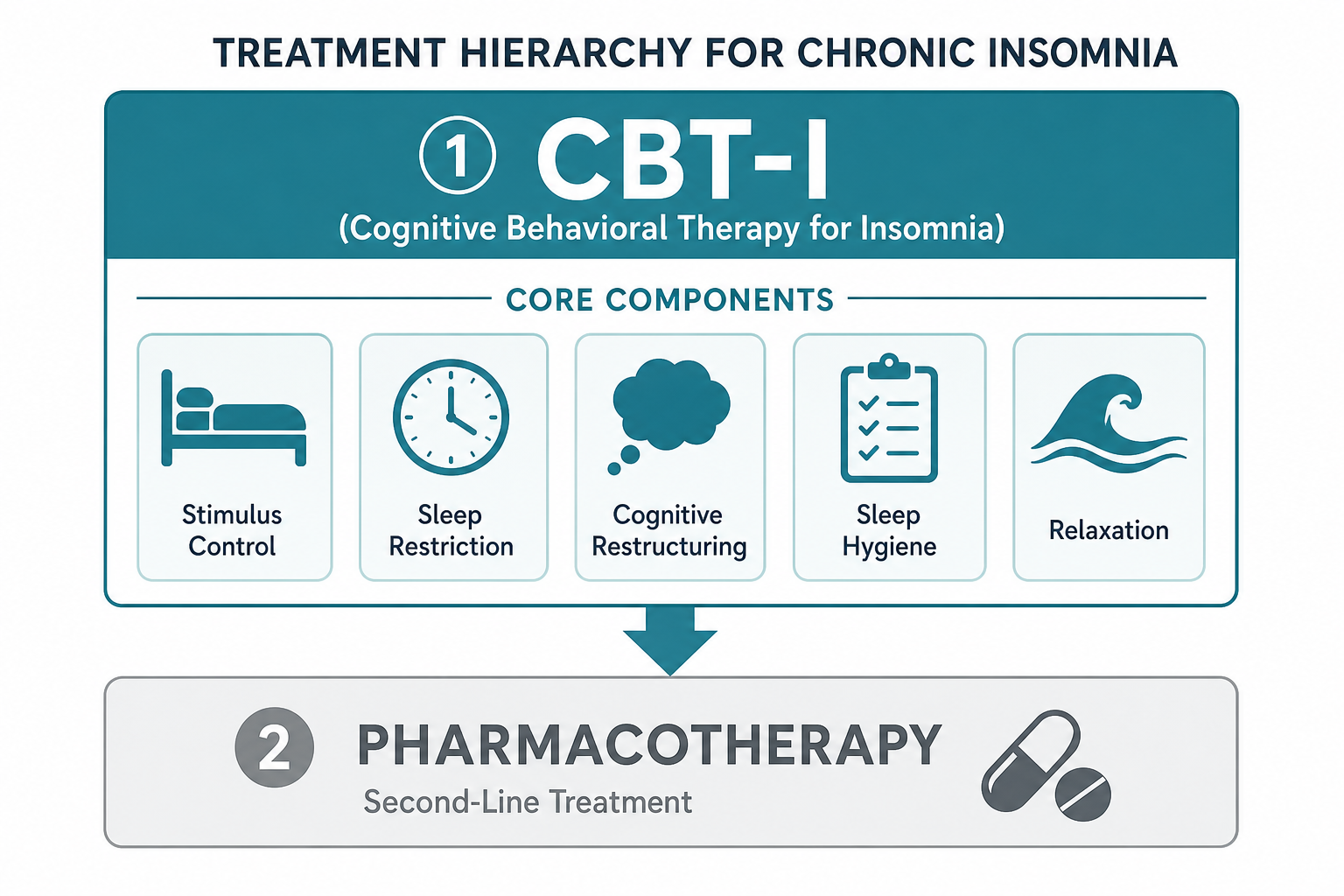
Every major clinical guideline — the American Academy of Sleep Medicine (AASM), the American College of Physicians (ACP), the 2023 European Insomnia Guideline, and the 2025 Chinese insomnia guidelines — places the same treatment at the top of the hierarchy: Cognitive Behavioral Therapy for Insomnia (CBT-I). Not sleep medication. Not supplements. CBT-I.
CBT-I: Components and How They Work
CBT-I is a multicomponent treatment — and the evidence consistently shows that the multicomponent approach outperforms any single component alone. Each component targets a specific perpetuating mechanism from the 3P model:
- Stimulus control — breaks conditioned arousal by restricting bed use to sleep and sex only, and instructing the person to leave the bed when unable to sleep. This progressively reassociates the bed and bedroom with sleep rather than wakefulness.
- Sleep restriction therapy — temporarily limits time in bed to the person's actual average sleep time, which initially increases homeostatic sleep pressure and consolidates fragmented sleep. Time in bed is then gradually extended as sleep efficiency improves.
- Cognitive restructuring — identifies and challenges dysfunctional beliefs about sleep ("I must get eight hours or I cannot function"; "I have lost control of my sleep") and replaces them with more accurate, less catastrophizing expectations.
- Sleep hygiene education — addresses behaviors that interfere with sleep: caffeine timing, alcohol use, irregular sleep schedules, and bedroom environment. This component alone is insufficient for chronic insomnia but supports the other components.
- Relaxation training — techniques such as progressive muscle relaxation, diaphragmatic breathing, or imagery rehearsal that reduce physiological and cognitive arousal at bedtime.
CBT-I produces response rates of 70–80% and — critically — its benefits persist long after treatment ends. This durability advantage over pharmacotherapy is one of the primary reasons guidelines place it first. A minimum effective course is four sessions; five or more sessions produce better outcomes. Six to eight sessions is a typical full course.
Digital CBT-I When In-Person Access Is Limited
Access to a CBT-I-trained therapist remains a significant practical barrier. The AASM recommends that when in-person CBT-I is unavailable or wait lists are extended, digital CBT-I (dCBT-I) is a reasonable alternative — followed by therapist-delivered CBT-I when it becomes accessible. Digital formats show comparable post-treatment efficacy to in-person delivery at lower cost.
Among available platforms, two stand out on evidence grounds. Somryst (formerly SHUTi) is the only FDA-cleared prescription digital therapeutic for chronic insomnia — it requires a clinician prescription. Sleepio has 12 published randomized controlled trials supporting its efficacy. Most other sleep apps have few or no published studies and should be evaluated cautiously.
Pharmacotherapy: Second-Line, Short-Term, With Caveats
Sleep medications are a second-line option — used when CBT-I has not produced sufficient improvement, when access to CBT-I is genuinely unavailable, or as a short-term bridge while behavioral treatment begins. They are not the default starting point.
| Drug Class | Examples | Mechanism | Key Considerations |
|---|---|---|---|
| Dual orexin receptor antagonists (DORAs) | Suvorexant, lemborexant, daridorexant | Block orexin A and B binding to OX1/OX2 receptors, reducing wake-promoting orexin signaling | Most mechanistically targeted option; more favorable profile for sleep maintenance insomnia; lower dependency risk than Z-drugs |
| Z-drugs | Zolpidem, eszopiclone | GABA-A receptor positive allosteric modulators | Second-line; short-term use only; risks of tolerance, dependency, next-day impairment, and parasomnias |
| Benzodiazepines | Temazepam, triazolam | GABA-A receptor agonists | Second-line; short-term only; significant dependency, tolerance, and cognitive impairment risk; Beers Criteria advises against use in adults ≥65 |
| Low-dose doxepin | Silenor | Histamine H1 receptor antagonism at low doses | FDA-approved specifically for sleep maintenance insomnia; minimal next-day sedation at approved doses |
| Melatonin | Various OTC formulations | Circadian signal; does not directly induce sleep | No convincing evidence for chronic insomnia disorder; AASM guidelines advise against prescribing it for this indication |
| OTC antihistamines | Diphenhydramine, doxylamine | Histamine H1 receptor antagonism | Very limited evidence for insomnia; rapid tolerance development; Beers Criteria advises against in adults ≥65 |
Prognosis and When to Seek Clinical Care
The natural course of untreated chronic insomnia disorder is not one of gradual self-resolution. The five-year naturalistic data are clear: 37.5% of people with the disorder still report it at every annual follow-up. Without addressing the perpetuating mechanisms, the condition persists.
With CBT-I, the picture is meaningfully different. Most people experience clinically significant improvement within 4–8 sessions, and the gains tend to be durable — the behavioral and cognitive changes that CBT-I produces continue to work after treatment ends, unlike pharmacotherapy, which requires ongoing use to maintain effect.
Professional evaluation is warranted in the following circumstances:
- Sleep difficulty meeting the ICSD-3 threshold: occurring three or more nights per week for three or more months, with meaningful daytime impairment
- Symptoms suggesting a comorbid sleep disorder — witnessed breathing pauses or gasping during sleep (possible obstructive sleep apnea), uncomfortable leg sensations at night with urge to move (possible restless legs syndrome), or excessive daytime sleepiness disproportionate to the nighttime sleep difficulty
- Insomnia accompanied by significant depression, anxiety, or — urgently — any suicidal ideation
- Self-managed behavioral approaches — consistent sleep schedule, reduced time in bed, stimulus control practices — that have not produced improvement after several weeks of consistent effort
- Insomnia in adults aged 65 or older, where medication selection carries higher risk and where the clinical picture may be more complex
Explore the mechanism
Next step
Spot an error or have clinical feedback?
Because this article covers clinical, medication, or safety information, we use a moderated correction channel instead of open public comments. Let us know if something about “Chronic Insomnia Disorder: Definition, Causes, Diagnosis, and Treatment” needs a closer look.
Send feedback on this article