Obstructive Sleep Apnea: Symptoms, Causes, Diagnosis, and Treatment Options
A clinically grounded guide to obstructive sleep apnea covering how airway collapse happens during sleep, why the condition is so often missed — especially in women — and what the current evidence says about diagnosis and treatment, from CPAP and oral appliances to the first FDA-approved OSA medication.
What Is Obstructive Sleep Apnea — and How Common Is It?
Obstructive sleep apnea (OSA) is a sleep-related breathing disorder in which the upper airway repeatedly collapses during sleep, blocking airflow for seconds to over a minute at a time. Each obstruction ends when the brain briefly rouses the sleeper enough to restore muscle tone and reopen the airway — often without the person ever fully waking or remembering it. This cycle can repeat dozens or hundreds of times a night.
OSA is distinct from central sleep apnea, in which breathing pauses occur because the brain temporarily fails to send the signal to breathe — with no obstruction and no respiratory effort. In OSA, the effort to breathe continues throughout the event; the airway is simply blocked. This distinction matters because the two conditions have different causes, different diagnostic patterns, and different treatment pathways.
The scale of OSA is difficult to overstate. Nearly 1 billion people are affected globally, with an estimated 425 million adults aged 30–69 living with moderate-to-severe disease. In the United States, 25–30% of men and 9–17% of women meet the diagnostic criteria. Yet despite this prevalence, the vast majority of people with OSA remain undiagnosed — estimates from multiple sources suggest that somewhere between 80% and 90% of cases go undetected.
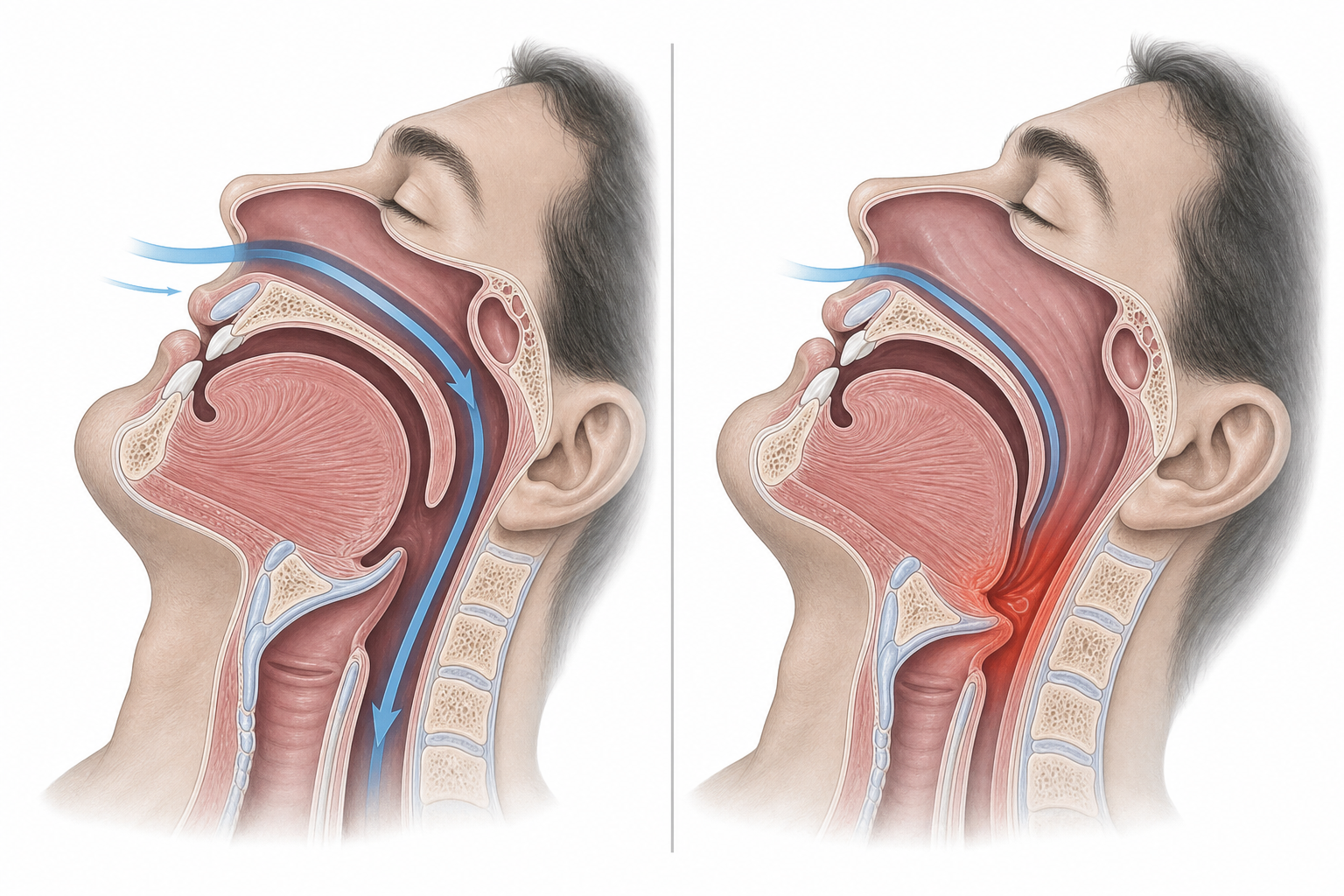
How the Airway Collapses During Sleep
Understanding why OSA happens requires a brief look at what keeps the upper airway open while you are awake — and what changes when you fall asleep.
The upper airway is a soft-walled tube. Unlike the trachea, it has no rigid structural support. During waking hours, a network of pharyngeal muscles — the genioglossus, tensor palatini, and others — actively contract to stiffen the airway walls and counteract the negative pressure created by each breath. This neuromuscular compensation keeps the airway patent even when its anatomy is less than ideal.
During sleep, that compensatory muscle activity diminishes significantly. The brain reduces its drive to the upper airway muscles as part of normal sleep physiology. For most people, this reduction is manageable. But in people with OSA, the airway is already compromised — by anatomy, by soft tissue volume, or by both — and the loss of neuromuscular tone is enough to allow collapse.
The mechanics work like this: when you inhale, the diaphragm creates negative pressure that pulls air down through the airway. That same negative pressure also exerts a collapsing force on the soft walls of the pharynx. In OSA, the airway walls are pulled inward by this pressure faster than the weakened muscles can resist. During expiration, the retropalatal region — the area just behind the soft palate — narrows progressively, setting up the next inhalation for a more severe obstruction.
Obesity amplifies this process. Excess adipose tissue deposited around the pharynx adds external compressive pressure on the airway walls, reducing the cross-sectional area available for airflow and making the airway more susceptible to collapse even with normal neuromuscular tone. This is why weight is both a major risk factor for OSA and a meaningful treatment target.
Symptoms: Classic Presentations and What Gets Missed
The textbook OSA presentation — a middle-aged man who snores loudly, stops breathing during sleep, and falls asleep at his desk — is real but far from universal. A substantial portion of people with OSA, particularly women, experience a different symptom profile that is both harder to recognize and more likely to be attributed to other causes.
The Classic Symptom Cluster
- Loud, disruptive snoring — caused by turbulent airflow through a partially obstructed airway
- Witnessed apneas — a bed partner observing breathing pauses that end with a gasp, snort, or choking sound
- Gasping or choking arousals — the brief awakening that terminates each apnea event and restores airway patency
- Excessive daytime sleepiness (EDS) — driven by the cumulative arousal burden that fragments sleep architecture across the night
- Unrefreshing sleep — waking feeling as tired as when you went to bed, despite adequate time in bed
Each of these symptoms has a direct mechanical cause. The arousals that terminate apnea events are generated by the brain's response to hypoxemia and rising carbon dioxide — they restore breathing but simultaneously fragment sleep, preventing the consolidation of deep NREM and REM stages. Over hundreds of events per night, this arousal burden produces the daytime sleepiness and cognitive impairment characteristic of OSA.
Atypical Presentations: Especially Common in Women
Women with OSA are significantly more likely to present with symptoms that do not fit the classic pattern. Research documented by the American Sleep Apnea Association identifies the following as disproportionately common in women with the condition:
- Persistent fatigue (distinct from sleepiness — more a sense of exhaustion than an urge to fall asleep)
- Insomnia and difficulty maintaining sleep through the night
- Mood disturbances including depression and anxiety
- Morning headaches, caused by overnight hypercapnia and vasodilation
- Nocturia — waking to urinate, driven by negative intrathoracic pressure that triggers atrial natriuretic peptide release
- Vivid or disturbing nightmares, associated with REM-predominant OSA
Women with OSA also tend to have fewer and shorter individual breathing pauses than men, with events concentrated in REM sleep rather than distributed across all sleep stages. This pattern can produce a lower overall AHI while still causing significant daytime impairment — research suggests that mild OSA in women produces daytime impairment comparable to moderate-to-severe OSA in men.
Risk Factors: Who Is Most Likely to Develop OSA
OSA risk is multifactorial. No single factor determines whether someone will develop the condition, but certain combinations substantially raise the probability.
Anatomical Factors
- Large neck circumference (>40 cm in women, >43 cm in men) — correlates with excess pharyngeal soft tissue
- Retrognathia (recessed jaw) — reduces the skeletal space available for the tongue and soft tissues
- Tonsillar or adenoid hypertrophy — reduces oropharyngeal cross-section directly
- Narrow or high-arched hard palate, nasal obstruction, or other craniofacial structural variants
Demographic Factors
- Male sex — men have higher OSA prevalence at most ages, though the gap narrows substantially after age 50
- Advancing age — airway muscle tone and structural support diminish with age; OSA prevalence rises in both sexes across the lifespan
- Race and ethnicity — Hispanic, Black, and Asian populations have elevated OSA risk; Asian individuals tend to have OSA at lower BMI levels due to craniofacial anatomy
Lifestyle Factors
- Obesity — the single strongest modifiable risk factor; excess adipose tissue increases pharyngeal collapsibility
- Alcohol use — selectively reduces upper airway muscle tone and increases both the frequency and duration of respiratory events
- Smoking — causes upper airway inflammation and increased mucus production
- Sedative medications including benzodiazepines and opioids — suppress neuromuscular compensatory activity
Comorbid Conditions
- Hypertension — both a risk factor for and a consequence of OSA; the relationship is bidirectional
- Atrial fibrillation, coronary artery disease, and heart failure — OSA prevalence reaches 40–80% in these populations
- Type 2 diabetes — insulin resistance and OSA share overlapping pathophysiology
- Hypothyroidism — reduces upper airway muscle tone and can cause macroglossia
- Polycystic ovary syndrome (PCOS) — women with PCOS are estimated to be nearly ten times more likely to have OSA than the general female population
- Menopause — postmenopausal women lose the protective effect of progesterone on upper airway muscle tone; some studies report OSA prevalence as high as 67% in postmenopausal women
Screening: The STOP-BANG Questionnaire
Before a formal sleep study, a validated screening tool can help identify who is most likely to have clinically significant OSA. The STOP-BANG questionnaire is the most widely used and best-validated instrument for this purpose. It consists of eight yes/no questions that can be completed in under two minutes.
| Letter | Question | Positive Response |
|---|---|---|
| S — Snoring | Do you snore loudly (louder than talking, or loud enough to be heard through closed doors)? | Yes |
| T — Tired | Do you often feel tired, fatigued, or sleepy during the daytime? | Yes |
| O — Observed | Has anyone observed you stop breathing, or choking/gasping, during your sleep? | Yes |
| P — Pressure | Do you have or are you being treated for high blood pressure? | Yes |
| B — BMI | Is your BMI greater than 35? | Yes |
| A — Age | Are you older than 50? | Yes |
| N — Neck | Is your neck circumference greater than 40 cm (about 15.7 inches)? | Yes |
| G — Gender | Are you male? | Yes |
Interpreting the score:
- 0–2: Low risk for OSA
- 3–4: Intermediate risk — clinical evaluation is reasonable, especially if other risk factors are present
- 5–8: High probability of moderate-to-severe OSA — formal sleep testing is warranted
Diagnosis: Sleep Studies, What They Measure, and Their Limitations
A clinical history and screening questionnaire can raise or lower suspicion for OSA, but diagnosis requires an objective sleep study. Two main options exist: in-laboratory polysomnography and home sleep apnea testing.
In-Laboratory Polysomnography: The Gold Standard
Polysomnography (PSG) is the most comprehensive sleep diagnostic tool available. Conducted overnight in a monitored sleep center, it simultaneously records multiple physiological signals:
- Electroencephalography (EEG) — tracks brain wave activity to stage sleep (N1, N2, N3, and REM) and identify arousals
- Electrooculography (EOG) — records eye movements to confirm REM sleep
- Electrocardiography (ECG) — detects cardiac arrhythmias associated with apneic events
- Pulse oximetry — measures oxygen saturation; desaturation events are a key marker of apnea severity
- Airflow channels (nasal pressure and thermistor) — directly detect cessation and reduction of airflow
- Respiratory effort belts (thoracic and abdominal) — distinguish obstructive events (effort continues) from central events (effort absent)
- Electromyography (EMG) of chin and leg muscles — detects muscle activity relevant to REM sleep behavior disorder and periodic limb movements
Because PSG measures actual sleep time using EEG, it calculates the apnea-hypopnea index (AHI) as events per hour of true sleep — the most accurate available measure of OSA severity.
Home Sleep Apnea Testing: Appropriate Use and a Critical Limitation
Home sleep apnea testing (HSAT) uses a portable device worn overnight at home. Most HSAT devices measure airflow, respiratory effort, oxygen saturation, and heart rate, but they do not include EEG — meaning they cannot distinguish sleep from wakefulness.
This creates a structural limitation. Because HSAT cannot confirm when the patient is actually asleep, it uses total recording time as the denominator when calculating the respiratory event index (REI) rather than total sleep time. If a patient spends 8 hours in the device but only sleeps 6 of them, all respiratory events are divided across 8 hours rather than 6 — systematically underestimating the true event rate.
HSAT is appropriate for adults with a high pretest probability of moderate-to-severe OSA who do not have significant cardiopulmonary disease, neuromuscular disease, chronic opioid use, a history of stroke, or severe insomnia. In these uncomplicated cases, HSAT offers a faster and less costly path to diagnosis without meaningful loss of accuracy for moderate-to-severe disease.
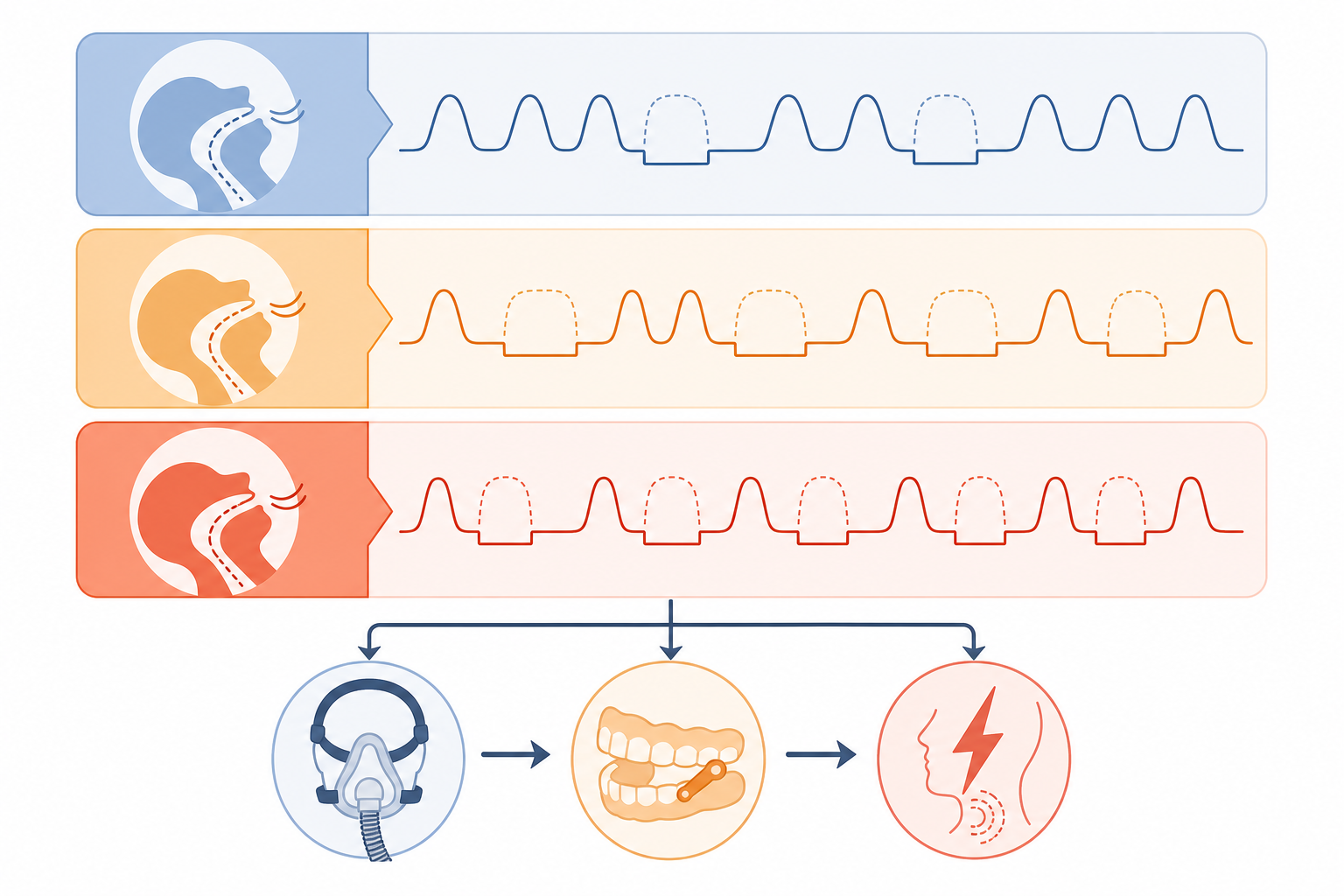
AHI Severity Grading
| Severity | AHI / REI (events per hour) | Clinical Significance |
|---|---|---|
| Normal | Fewer than 5 | No OSA diagnosis; some symptoms may warrant evaluation for other causes |
| Mild OSA | 5 to fewer than 15 | Symptoms may be present; treatment is recommended when symptoms are significant |
| Moderate OSA | 15 to fewer than 30 | Significant cardiovascular and neurobehavioral risk; treatment is recommended |
| Severe OSA | 30 or more | High cardiovascular risk; associated with increased mortality; treatment is strongly recommended |
Treatment Options: Evidence, Trade-offs, and How to Choose
OSA treatment has expanded considerably over the past decade. No single option is right for every patient, and the honest picture involves acknowledging both the strengths and the real-world limitations of each approach.
Positive Airway Pressure: CPAP, APAP, and BiPAP
Continuous positive airway pressure (CPAP) remains the most efficacious treatment for OSA across all severity levels. It works by delivering a constant stream of pressurized air through a mask, acting as a pneumatic splint that holds the pharyngeal walls open throughout the respiratory cycle. When used consistently, CPAP virtually eliminates apnea events and normalizes the AHI.
Auto-titrating PAP (APAP) adjusts pressure breath-by-breath based on detected airway resistance — useful for patients whose pressure needs vary by sleep position or sleep stage. BiPAP delivers different pressures on inhalation and exhalation and is typically reserved for patients who require higher pressures or who have difficulty exhaling against a fixed pressure.
The central challenge with PAP therapy is adherence. Approximately 50% of patients discontinue CPAP within the first month. Mask discomfort, pressure intolerance, claustrophobia, and nasal congestion are the most commonly cited reasons. This is a real and well-documented problem — but it is also a solvable one. Strategies with evidence behind them include:
- Telemedicine-based remote monitoring — allows clinicians to identify and address adherence problems within days of initiation rather than weeks
- Mask fitting support — proper mask interface selection (nasal pillow, nasal mask, or full-face mask) substantially affects comfort and leak rates
- APAP rather than fixed-pressure CPAP — reduces the experience of pressure intolerance during exhalation
- Heated humidification — reduces nasal congestion and dryness, a common adherence barrier
- Structured patient education about the mechanism and long-term benefits
Oral Appliances (Mandibular Advancement Devices)
Mandibular advancement devices (MADs) are custom-fitted oral appliances that reposition the lower jaw and tongue forward during sleep, increasing the posterior airway space and reducing collapsibility. The American Academy of Sleep Medicine recommends MADs as an alternative to CPAP, particularly for patients with mild-to-moderate OSA or for those with moderate-to-severe OSA who cannot tolerate PAP therapy.
The response to MADs is variable and patient-dependent. Across studies, roughly one-third of MAD users achieve complete resolution of OSA (AHI below 5), another third achieve a clinically meaningful reduction of 50% or more, and the remaining third show minimal improvement. Careful patient selection — including consideration of dental health, jaw anatomy, and baseline AHI — is important.
Importantly, long-term randomized trial data show that MADs produce neurobehavioral outcomes — including cognitive performance, mood, and quality of life — equivalent to CPAP at 10-year follow-up. This parity likely reflects higher real-world adherence with MADs offsetting their somewhat lower per-night AHI reduction compared to CPAP. For patients who will not consistently use CPAP, a well-fitted MAD may deliver better real-world outcomes.
Hypoglossal Nerve Stimulation (Upper Airway Stimulation)
Upper airway stimulation (UAS), marketed as Inspire, is an implanted neurostimulation device that delivers mild electrical stimulation to the hypoglossal nerve in synchrony with each breath, activating the genioglossus and other tongue muscles to maintain airway patency during sleep. It is FDA-approved for moderate-to-severe OSA in patients who cannot adequately use PAP therapy.
In the pivotal STAR trial, UAS reduced AHI by a median of 68% — from approximately 29.3 to 9.0 events per hour. Eligibility criteria are specific: AHI between 20 and 65, BMI at or below 32, documented CPAP intolerance, and absence of complete concentric palatal collapse on drug-induced sleep endoscopy. Patients outside these parameters are unlikely to achieve the same outcomes.
Surgical Options
Several surgical procedures address OSA by modifying airway anatomy. Uvulopalatopharyngoplasty (UPPP) removes excess soft palate tissue and the uvula; it is most effective in patients with retropalatal obstruction and is generally considered for patients with BMI below 40 who cannot use PAP. Maxillomandibular advancement (MMA) surgically repositions the upper and lower jaw to expand the skeletal airway space and is one of the most effective surgical options for anatomically appropriate candidates. Tracheostomy bypasses the upper airway entirely and is reserved for the most severe, refractory cases. Surgical outcomes are anatomy-dependent and should be discussed with a specialist in a multidisciplinary setting.
Positional Therapy and Lifestyle Modifications
For patients whose OSA is predominantly or exclusively positional — occurring primarily in the supine position — positional therapy (devices or strategies that prevent back-sleeping) can meaningfully reduce event frequency. This is rarely sufficient as a standalone treatment for moderate-to-severe OSA but may be a useful adjunct.
Weight loss is recommended in the management of OSA for more than 80% of cases. Even a 5–10% reduction in body weight reduces upper airway collapsibility and lowers AHI. For patients with significant obesity, weight loss may produce sustained remission of OSA, though it does not reliably eliminate the condition in all cases and should not be used as a reason to delay PAP therapy. Alcohol avoidance in the hours before sleep is also recommended, given alcohol's direct effect on upper airway muscle tone.
| Treatment | First-Line? | AHI Reduction | Key Consideration |
|---|---|---|---|
| CPAP / APAP | Yes — most efficacious | Near-complete elimination when used | ~50% discontinue within first month; adherence strategies are essential |
| Oral appliance (MAD) | AASM-recommended alternative | Variable: ~1/3 complete resolution, ~1/3 ≥50% reduction | 10-year RCT parity with CPAP on neurobehavioral outcomes; higher adherence |
| Hypoglossal nerve stimulation (Inspire) | For CPAP-intolerant patients with AHI 20–65, BMI ≤32 | Median 68% reduction (STAR trial) | Requires drug-induced sleep endoscopy to confirm eligibility; surgical implant |
| Surgical (UPPP, MMA, tracheostomy) | For specific anatomical cases | Variable; MMA among most effective surgical options | BMI, anatomy, and comorbidities determine candidacy |
| Positional therapy | Adjunct for positional OSA | Moderate for supine-predominant OSA | Rarely sufficient alone for moderate-to-severe OSA |
| Weight loss | Recommended in >80% of cases | Proportional to weight reduction achieved | 5–10% body weight reduction reduces pharyngeal collapsibility; does not replace PAP |
A New Pharmacological Option: Tirzepatide (Zepbound)
On December 20, 2024, the FDA approved tirzepatide, sold under the brand name Zepbound, as the first medication ever approved for the treatment of obstructive sleep apnea. This is a genuinely new development in OSA management, and its scope and limitations deserve careful explanation.
Tirzepatide is a dual GIP and GLP-1 receptor agonist that reduces appetite and food intake, producing significant weight loss. The FDA approval is specifically for adults with obesity and moderate-to-severe OSA, to be used in combination with a reduced-calorie diet and increased physical activity. The mechanism of benefit is primarily through weight reduction and the associated decrease in pharyngeal soft tissue pressure — not a direct pharmacological effect on airway tone.
The supporting evidence comes from the SURMOUNT-OSA phase 3 trials, two randomized, double-blind, placebo-controlled studies enrolling adults with moderate-to-severe OSA and obesity, none of whom had type 2 diabetes. At 52 weeks:
- In trial 1 (PAP-naive participants), tirzepatide reduced AHI by approximately 25.3 events per hour more than placebo
- In trial 2 (participants using PAP therapy), the reduction was approximately 29.3 events per hour more than placebo
- Body weight decreased by approximately 17.7% in trial 1 and 19.6% in trial 2, compared to 1.6–2.3% in placebo groups
- Up to 50.2% of tirzepatide-treated participants achieved the combined endpoint of AHI below 5 or AHI 5–14 with an Epworth Sleepiness Scale score of 10 or less
- Mean systolic blood pressure reductions were approximately 9.5 and 7.6 mmHg in the two trials
The most common adverse effects in the trials were gastrointestinal: diarrhea (23.9%), nausea (23.5%), constipation (15.4%), and vomiting (13.2%). Tirzepatide is contraindicated in patients with a personal or family history of medullary thyroid carcinoma or multiple endocrine neoplasia syndrome type 2 (MEN2).
Health Consequences of Untreated OSA
The consequences of unmanaged OSA extend well beyond daytime sleepiness. Each apnea event triggers a cascade of physiological responses — intermittent hypoxemia, surges in sympathetic nervous system activity, and the release of inflammatory mediators — that accumulate into systemic disease over years.
- Hypertension: Approximately 50% of people with OSA have hypertension. The sympathetic activation triggered by each apnea event raises heart rate and blood pressure throughout the night, and this nocturnal pressure load persists into waking hours. OSA is one of the most common identifiable causes of resistant hypertension.
- Atrial fibrillation: Acute apneic episodes cause hypoxia, hypercapnia, and autonomic dysregulation that promote structural remodeling of the atria. OSA is an independent risk factor for AF and is present in a large proportion of patients with recurrent AF after cardioversion or ablation.
- Stroke and coronary artery disease: Chronic intermittent hypoxemia and systemic inflammation accelerate atherosclerosis and increase stroke risk. OSA prevalence reaches 40–80% in patients with hypertension, heart failure, coronary artery disease, and stroke.
- Type 2 diabetes: Intermittent hypoxemia impairs insulin sensitivity and glucose metabolism through multiple pathways, including cortisol elevation and sympathetic activation.
- Mortality: Severe OSA is associated with increased all-cause and cardiovascular mortality in meta-analyses. PAP therapy is associated with a 42% lower mortality rate in patients with severe OSA — though this risk reduction was not observed until 6–7 years of follow-up, underscoring the importance of long-term adherence.
- Drowsy driving: Excessive daytime sleepiness from untreated OSA significantly increases the risk of motor vehicle accidents. This is a public safety issue as well as a personal health risk.
The cardiovascular burden of OSA is not a distant or theoretical risk. The American Heart Association's 2021 Scientific Statement on OSA and cardiovascular disease concludes that OSA is often underrecognized and undertreated in cardiovascular practice despite its high prevalence in these populations, and recommends routine screening for OSA in patients with resistant hypertension, pulmonary hypertension, and recurrent atrial fibrillation after cardioversion or ablation.
When to See a Doctor
Most people with OSA do not recognize it in themselves. The clearest path to diagnosis is knowing which signals warrant a clinical conversation.
- A bed partner has witnessed you stop breathing, gasp, or choke during sleep — this is one of the strongest clinical indicators and should prompt evaluation promptly
- You snore loudly most nights, particularly if accompanied by daytime sleepiness or unrefreshing sleep
- You score 3 or higher on the STOP-BANG questionnaire, especially if you have unexplained fatigue, morning headaches, or mood changes
- You have resistant hypertension, recurrent atrial fibrillation, or unexplained heart failure — OSA should be ruled out as a contributing cause
- You are a woman with unexplained fatigue, insomnia, depression, or anxiety that has not responded to standard treatment — atypical OSA presentation should be considered
- You have PCOS, hypothyroidism, or are postmenopausal and experiencing significant sleep disruption
- You have fallen asleep while driving or nearly done so — this is a safety emergency and warrants immediate evaluation
For most adults without significant cardiopulmonary or neuromuscular comorbidities, a home sleep apnea test ordered by a primary care physician or sleep specialist is a reasonable first step. If the HSAT is negative but clinical suspicion remains high, in-lab polysomnography should follow — a negative home study does not rule out mild OSA.
The primary obstacle for most people with OSA is not the condition itself — it is the gap between symptoms and diagnosis. OSA is diagnosable with a single overnight study and treatable with options that have decades of evidence behind them. The 80–90% of people with undiagnosed OSA are not a medical mystery; they are people who have not yet connected their symptoms to a sleep study.
Explore the mechanism
Next step
Spot an error or have clinical feedback?
Because this article covers clinical, medication, or safety information, we use a moderated correction channel instead of open public comments. Let us know if something about “Obstructive Sleep Apnea: Symptoms, Causes, Diagnosis, and Treatment Options” needs a closer look.
Send feedback on this article