Insomnia FAQ: Causes, Duration, Treatment, Sleep Aids, and When It Becomes a Disorder

What Actually Makes Poor Sleep 'Insomnia'?
Not every stretch of poor sleep is insomnia. The clinical definition requires two things to be true at the same time: difficulty sleeping at night and meaningful impairment the next day. If you sleep badly but wake up feeling reasonably functional — no significant effects on your mood, concentration, work, or relationships — you do not meet the diagnostic threshold for insomnia disorder, regardless of how tired you feel at 3 a.m.
This distinction matters because it separates a normal human stress response from a clinical condition. Sleep medicine physicians are explicit on this point: the daytime impairment criterion is what elevates poor sleep to a diagnosable disorder. Most adults will experience a run of bad nights at some point — during a difficult work period, a health scare, or a major life event. That is not insomnia disorder. Insomnia disorder is when the difficulty persists, recurs at least three nights per week, and produces real functional consequences during waking hours.
What Causes Insomnia?
Sleep medicine uses a three-factor framework — commonly called the 3P model — to explain how insomnia develops and why it persists in some people but not others. The three factors are predisposing traits, precipitating events, and perpetuating behaviors. All three typically need to be present for a short-term sleep disruption to cross into chronic insomnia disorder.
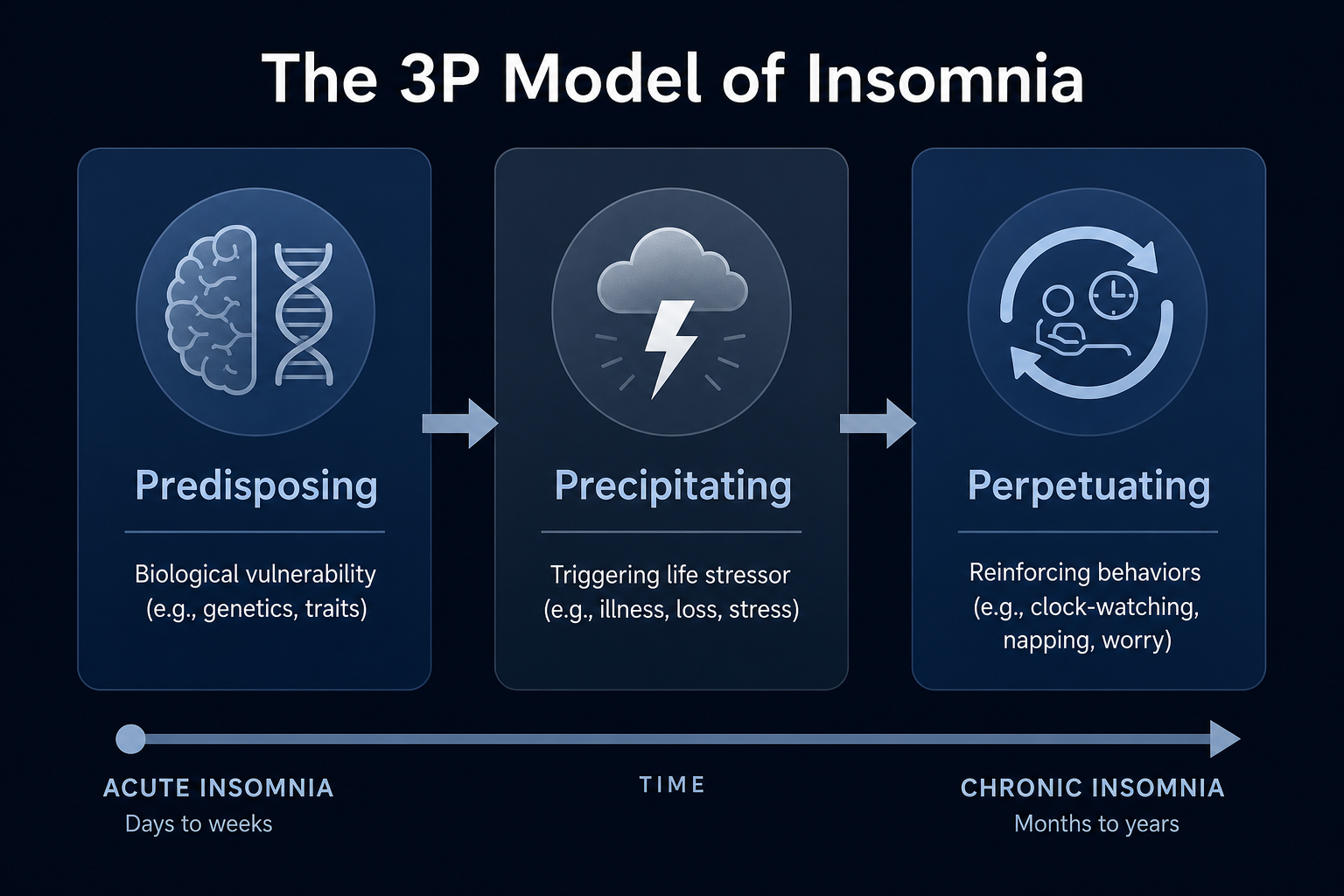
- Predisposing factors are the biological and psychological traits that lower your threshold for sleep disruption. These include a naturally light or short sleep pattern, a tendency toward hyperarousal, a history of anxiety, or a genetic predisposition to sleep reactivity. A person with these traits is not destined to develop insomnia — but they are more vulnerable when a stressor arrives.
- Precipitating factors are the events or circumstances that trigger the initial sleep disruption: a bereavement, a job change, a medical diagnosis, relationship stress, or a shift in living situation. Almost anyone will sleep worse in response to a major stressor. For most people, sleep returns to normal once the stressor resolves.
- Perpetuating factors are the behaviors and thought patterns that keep insomnia going after the original trigger has passed. Clock-watching during the night, spending extra time in bed to compensate for lost sleep, daytime napping, using alcohol to fall asleep, and developing anxious anticipation of another bad night all reinforce the sleep problem. These are the most actionable lever — they are also the primary target of effective treatment.
A concrete example: someone who is naturally a light sleeper (predisposing) loses a family member (precipitating) and begins staying up late watching television and drinking wine to wind down (perpetuating). The stressor may eventually pass, but the behavioral patterns have now taken hold — and the sleep problem continues long after the grief has eased. This is the typical pathway from acute to chronic insomnia.
How Long Does Insomnia Usually Last?
The duration question has two very different answers depending on whether the insomnia is acute or chronic.
| Type | Duration threshold | Typical trajectory |
|---|---|---|
| Acute insomnia | Less than 3 months | Often self-resolving — even without treatment, sleep typically returns to normal as the triggering stressor recedes |
| Chronic insomnia disorder | 3 months or longer, at least 3 nights per week | Tends to persist; a significant proportion of people continue to meet diagnostic criteria year after year without treatment |
Acute insomnia is a normal biological response to stress. Most people who experience a difficult sleep period during a challenging life event will find their sleep normalizes within weeks to a few months, without any formal intervention. This is expected and does not require clinical treatment in most cases.
Chronic insomnia follows a different pattern. A large prospective study by Morin and colleagues, published in JAMA Network Open in 2020 and cited in StatPearls, found that 37.5% of people with insomnia continued to meet diagnostic criteria at each annual follow-up assessment over five years. The same study found that 13.9% of people who were good sleepers at the start of the study developed insomnia syndrome during that period. Chronic insomnia is not simply a phase that resolves on its own for most people who develop it.
When Does Poor Sleep Become Insomnia Disorder?
The current clinical standard for diagnosing insomnia disorder comes from both the International Classification of Sleep Disorders (ICSD-3-TR) and the DSM-5. The core criteria are consistent across both systems. A clinician will look for all of the following before making a diagnosis:
- Criterion A — Sleep difficulty: Dissatisfaction with sleep quantity or quality, characterized by difficulty falling asleep, difficulty staying asleep (frequent awakenings or trouble returning to sleep), or early-morning awakening with an inability to return to sleep.
- Criterion B — Daytime impairment: The sleep disturbance causes clinically significant distress or impairment in social, occupational, educational, or other important areas of functioning. This might include fatigue, difficulty concentrating, mood disturbance, reduced performance at work, or increased errors.
- Criterion C — Frequency: The sleep difficulty occurs at least three nights per week.
- Criterion D — Duration: The sleep difficulty has been present for at least three months (for the 'persistent' specifier).
- Criterion E — Adequate opportunity: The sleep difficulty occurs despite adequate opportunity and circumstances for sleep. Someone who cannot sleep because of an excessively noisy environment or a forced early schedule does not meet this criterion.
- Criteria F–H — Not better explained by: Another sleep disorder, a substance or medication, a coexisting mental disorder, or a medical condition that fully accounts for the sleep complaint.
One important shift in the DSM-5 framework compared to the older DSM-IV is that insomnia disorder can now be diagnosed as a comorbid condition alongside other mental or medical disorders — not only when it stands alone. Under DSM-IV, a clinician had to determine whether insomnia was 'primary' (independent) or 'secondary' (caused by another condition) before diagnosing it. DSM-5 removed that distinction. If someone has both depression and insomnia, both can be diagnosed and treated directly.
Diagnosis is clinical. A doctor or sleep specialist will typically conduct a structured interview and ask the patient to keep a sleep diary for 7 to 14 days before or during the evaluation. Validated screening tools such as the Insomnia Severity Index (ISI) are commonly used to grade severity. Polysomnography — an overnight sleep study — is not required to diagnose insomnia disorder. It is only indicated when a comorbid sleep disorder such as obstructive sleep apnea or periodic limb movement disorder is suspected.
What Are the Recommended Treatments for Insomnia?
For chronic insomnia disorder, the first-line treatment endorsed by both the American Academy of Sleep Medicine (AASM) and the European Insomnia Guidelines is Cognitive Behavioral Therapy for Insomnia (CBT-I) — not medication, and not supplements. This recommendation reflects the evidence base: CBT-I produces durable improvements that last after treatment ends, whereas pharmacological effects typically diminish when the drug is stopped.
CBT-I is a structured, multi-component program. Its core components include:
- Stimulus control: Rebuilding the association between the bed and sleep by restricting bed use to sleep and sex only — not reading, watching television, or lying awake anxiously. If you cannot sleep after approximately 20 minutes, you leave the bed and return only when sleepy.
- Sleep restriction therapy: Temporarily limiting time in bed to match actual sleep time, which consolidates sleep and builds sleep pressure. This is counterintuitive but well-supported by evidence — spending less time in bed initially increases sleep efficiency.
- Sleep hygiene as a component: Behavioral practices such as consistent wake times, limiting caffeine, and managing light exposure. Critically, sleep hygiene alone — without the behavioral and cognitive components of CBT-I — has minimal effectiveness for chronic insomnia disorder. It is a supporting element, not a standalone treatment.
- Cognitive restructuring: Identifying and reframing unhelpful beliefs about sleep — such as catastrophizing the consequences of a bad night — that fuel the hyperarousal cycle.
Approximately 70 to 80 percent of patients who complete a structured CBT-I program respond favorably, and some achieve full remission from insomnia disorder. Digital and app-based CBT-I programs have expanded access significantly — they deliver the same core components in a self-guided format and are a viable option for people who cannot access in-person therapy.
Pharmacological treatments — including sedative-hypnotics, low-dose antidepressants with sedating properties, and orexin receptor antagonists — are considered second-line options. They may be appropriate for patients who cannot engage with CBT-I, those who remain symptomatic after completing CBT-I, or those who need short-term pharmacological support alongside behavioral therapy. Prescription sleep medications are outside the scope of this FAQ; they require clinical evaluation and prescribing by a qualified clinician.
What Can OTC Sleep Aids Actually Do — and What Can't They Do?
Over-the-counter sleep aids are widely used, but the evidence for their effectiveness in diagnosed insomnia is considerably weaker than their market presence suggests. There are three main categories worth understanding.
Antihistamines: Diphenhydramine and Doxylamine
Diphenhydramine (found in ZzzQuil, Benadryl, and many store-brand sleep aids) and doxylamine (found in Unisom SleepTabs) are first-generation antihistamines. They cause drowsiness as a side effect of blocking histamine receptors in the brain — they were not developed as sleep medications. Their use for insomnia is essentially repurposed from their allergy and cold applications.
A systematic review of OTC sleep agents identified only three qualifying polysomnography (PSG) studies of diphenhydramine. The largest well-designed study in that review found no significant differences between diphenhydramine and placebo on key objective sleep measures — including sleep onset latency, sleep efficiency, and total sleep time. Next-day psychomotor impairment was confirmed: reduced wakefulness and impaired working memory the following day. The review's overall conclusion was 'limited support' for diphenhydramine as a sleep aid. It is worth noting that one co-author of this review was a Pfizer employee and the research was Pfizer-funded, which is a relevant conflict of interest when interpreting the findings.
Tolerance is a significant practical problem. As Mayo Clinic notes, the sedating effect of antihistamines diminishes with repeated use — the longer you take them, the less likely they are to make you sleepy. This makes them unsuitable for ongoing use even if they provide some initial benefit.
Melatonin
Melatonin is not a sedative hypnotic. It is a hormone produced by the pineal gland that signals to the brain that darkness has arrived — it helps regulate the timing of sleep, not the depth or quality of sleep itself. This distinction matters for understanding what melatonin can and cannot do.
The AASM clinical practice guideline is explicit: clinicians should not use melatonin to treat chronic insomnia disorder. Melatonin has evidence-based support for circadian timing problems — jet lag and shift work disorder — but not for the type of insomnia most adults experience. Using melatonin to treat chronic insomnia is applying a circadian-timing tool to a problem that is primarily behavioral and neurobiological.
Consumer melatonin doses are also far higher than what is physiologically needed. The dose required to shift the circadian clock is approximately 0.3 milligrams. Most OTC melatonin products contain 5, 10, or even 20 milligrams — doses that exceed the physiological threshold and increase the risk of side effects including vivid dreams and next-day grogginess.
There is an additional quality control problem specific to melatonin as a dietary supplement. A 2017 study published in the Journal of Clinical Sleep Medicine and cited by the AASM found that melatonin content in OTC supplements deviated from the label claim in more than 71% of products tested. Actual content ranged from 83% less to 478% more than stated, with lot-to-lot variability of up to 465% within the same brand. This is not a minor labeling imprecision — it means consumers cannot reliably know what dose they are actually taking.
OTC Sleep Aids at a Glance
| Agent | Mechanism | PSG evidence for insomnia | Key limitations | Suitable for |
|---|---|---|---|---|
| Diphenhydramine | Antihistamine (sedating side effect) | Weak — no significant improvement on key PSG parameters in largest qualifying study | Tolerance develops quickly; next-day impairment; avoid in adults 65+ | Occasional short-term use only; not for diagnosed chronic insomnia |
| Doxylamine | Antihistamine (sedating side effect) | Limited; similar profile to diphenhydramine | Same tolerance and impairment concerns; avoid in adults 65+ | Occasional short-term use only; not for diagnosed chronic insomnia |
| Melatonin | Circadian timing hormone — shifts sleep-wake timing | AASM advises against use for chronic insomnia disorder | High consumer doses; >71% of products inaccurate on label; not a sedative hypnotic | Jet lag; shift work disorder; circadian timing adjustment — not chronic insomnia |
When Should You See a Doctor About Sleep Problems?
Many people wait far longer than necessary before seeking evaluation for sleep problems — often because they assume poor sleep is normal, or because they have been managing with OTC aids and caffeine. There are clear signals that indicate it is time to talk to a clinician rather than continue self-managing.
The NHLBI frames it directly: if not getting enough sleep is affecting your daily activities, talk to your doctor.
- Sleep difficulty at least 3 nights per week for 3 months or longer. This meets the frequency and duration threshold for chronic insomnia disorder and warrants clinical evaluation.
- Meaningful daytime dysfunction. Difficulty concentrating at work, reduced performance, persistent fatigue, mood disturbance, or increased irritability that you attribute to poor sleep are all forms of daytime impairment that should be evaluated.
- Comorbid anxiety or depression symptoms. Insomnia and anxiety or depression frequently co-occur and can reinforce each other. Both conditions can be diagnosed and treated simultaneously under current clinical guidelines — neither needs to be resolved first.
- Snoring, gasping, or witnessed breathing pauses during sleep. These symptoms suggest obstructive sleep apnea, a separate and serious sleep disorder that requires different evaluation and treatment. Sleep apnea also disrupts sleep quality and can produce insomnia-like symptoms, but it will not respond to CBT-I or OTC sleep aids.
- Restless or uncomfortable sensations in the legs at night. This pattern may indicate restless legs syndrome, another condition that requires clinical assessment distinct from insomnia disorder.
Where to Go From Here
This FAQ covers the clinical threshold, causal model, duration patterns, treatment hierarchy, and OTC evidence in summary form. Each of these areas has considerably more depth available depending on what you need next.
- If you want the full clinical picture of insomnia disorder — definition, prevalence, diagnostic criteria in detail, all treatment options, and when to seek care — the insomnia condition reference page covers the complete clinical architecture.
- If you want to understand CBT-I in depth — how stimulus control works mechanistically, how sleep restriction is implemented, what a full CBT-I program looks like week by week — the CBT-I guide in the Sleep Hygiene section covers the protocol as a structured multi-component treatment.
- If you want to compare OTC sleep aids at the ingredient level — mechanism of action, dosage ranges, FDA regulatory status, evidence quality ratings, and full population safety notes — the Sleep Aids section has per-ingredient explainer pages for diphenhydramine, doxylamine, melatonin, magnesium glycinate, and others.
- If you want to build better behavioral sleep practices — not as a substitute for CBT-I if you have chronic insomnia, but as an evidence-grounded foundation — the Sleep Hygiene section covers the physiological mechanisms behind each practice, not just the recommendations.
Read the full guide: Chronic Insomnia Disorder: Definition, Causes, Diagnosis, and Treatment