Mechanism explainer
Sleep Hygiene Fundamentals and an Evidence-Based Bedtime Routine
A mechanistic guide for adults who have seen generic sleep tips and want to understand why each behavior works — covering the two biological processes that govern sleep, a prioritized evidence-ranked framework of core hygiene practices, a step-by-step 60-minute bedtime routine, and honest guidance on when sleep hygiene alone is not enough to address chronic insomnia.
What Sleep Hygiene Actually Is — and What It Is Not
Sleep hygiene refers to a set of behavioral and environmental practices that support the biological conditions your body needs to fall asleep and stay asleep. The term is used loosely in popular culture — often as shorthand for any sleep advice — but it has a more specific meaning that is worth establishing before anything else.
Sleep hygiene is not the same as cognitive behavioral therapy for insomnia (CBT-I). CBT-I is a structured, multi-component clinical protocol that includes sleep hygiene education alongside stimulus control therapy, sleep restriction, cognitive restructuring, and relaxation training. Sleep hygiene is one part of that protocol — not the whole thing.
This distinction matters because the two are often conflated, and the conflation leads to unrealistic expectations. When someone with chronic insomnia tries a list of sleep hygiene tips and finds they do not work, the failure is often attributed to the individual rather than to the mismatch between the intervention and the problem.
This article is for adults who want to understand why specific sleep behaviors work — not just that they work. That mechanistic grounding is what allows you to prioritize intelligently, build a routine that holds up over time, and recognize when the problem requires a different approach.
The Biology Behind the Habits: How Sleep Is Actually Regulated
To understand why any sleep hygiene behavior works, you need a basic map of how sleep is regulated. Sleep researchers describe this through a two-process model, and once you understand it, the logic behind almost every behavioral recommendation becomes obvious.
The first process is homeostatic sleep pressure, sometimes called Process S. From the moment you wake up, your brain accumulates a chemical called adenosine. Adenosine is a byproduct of neural activity — the longer you are awake, the more of it builds up, and the stronger the drive to sleep becomes. When you sleep, adenosine clears. This is the mechanism behind why you feel progressively sleepier across the day and why a full night of sleep leaves you feeling restored.
The second process is circadian timing, called Process C. Your brain contains a master clock — the suprachiasmatic nucleus (SCN) — located in the hypothalamus. The SCN responds to light and dark signals detected by specialized cells in your retina called intrinsically photosensitive retinal ganglion cells (ipRGCs). In the evening, as light fades, the SCN triggers the pineal gland to release melatonin, which signals to the body that it is time to prepare for sleep. In the morning, rising light suppresses melatonin and increases cortisol and body temperature, promoting wakefulness.
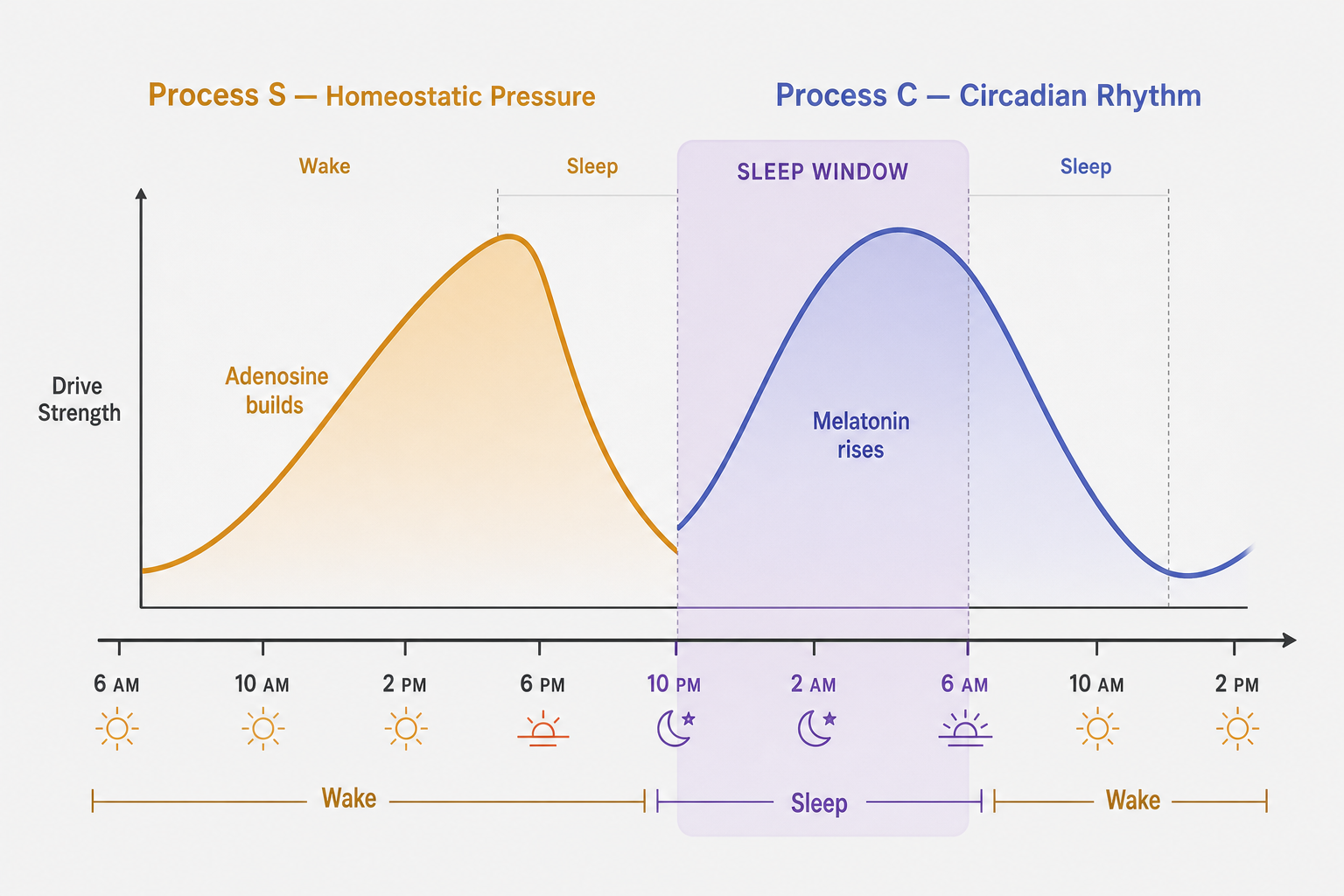
These two processes operate independently but interact. Healthy sleep happens when both processes are aligned — when homeostatic pressure is high enough and the circadian clock is signaling the right time. Sleep hygiene behaviors work by supporting one or both of these processes. The highest-leverage habits are those that affect both simultaneously.
Core Behavioral Pillars, Ranked by Evidence Strength
The six behavioral pillars below are ordered from highest to lowest evidence strength. Each is anchored to the biological process it supports. Starting with the top two will produce the most measurable change; the remaining pillars compound the effect.
1. Consistent Wake Time — Highest Leverage
Waking at the same time every day — including weekends — is the single most impactful sleep hygiene behavior available. It works on both processes simultaneously.
A fixed wake time anchors your circadian clock. The SCN uses consistent light exposure at a predictable time to calibrate melatonin timing. Irregular wake times shift the circadian phase unpredictably, making it harder to fall asleep at your intended bedtime. A consistent wake time also ensures that adenosine pressure accumulates across the same daily window, making sleepiness at bedtime more reliable.
Research on sleep regularity has found it to be a stronger predictor of long-term health outcomes than sleep duration alone. If you can commit to only one change, this is it.
2. Light Exposure Management — Morning and Evening
Light is the primary signal the circadian clock uses to set its timing. Managing your light exposure — both what you get in the morning and what you avoid in the evening — is the behavioral lever with the strongest physiological mechanistic evidence.
In the morning, bright light exposure — ideally natural daylight — activates the ipRGC pathway and tells the SCN to suppress melatonin and advance circadian phase toward earlier sleep timing. In the evening, the reverse is needed: dim, warm-toned light allows melatonin to rise on schedule.
The role of blue light is real but often oversimplified. ipRGCs are maximally sensitive to short-wavelength blue light peaking around 480 nm. A 2024 study in Chronobiology in Medicine found that following two hours of LED tablet exposure, participants showed approximately a 55% decrease in melatonin and a melatonin onset delay of roughly 1.5 hours compared to reading a printed book under low light. Research from Harvard comparing blue and green light exposure found that blue light shifted circadian rhythms by about twice as much as green light of comparable brightness — approximately three hours versus 1.5 hours.
3. Stimulus Control — A CBT-I Component, Not Basic Hygiene
Stimulus control is frequently listed as a sleep hygiene tip, but it is important to label it accurately: it is a formal component of CBT-I with its own evidence base, and it carries significantly stronger evidence than most passive hygiene behaviors.
The principle is straightforward. The bed should be used only for sleep and sex. If you lie awake in bed for extended periods — whether scrolling, watching television, reading, or worrying — your brain learns to associate the bed with wakefulness rather than sleep. Over time, getting into bed becomes a cue for arousal rather than for sleep.
The practical rule: if you have not fallen asleep within approximately 20 minutes, get out of bed and do something quiet and low-stimulation in dim light until you feel genuinely sleepy, then return. This is uncomfortable to implement at first, but it is among the most effective behavioral interventions for insomnia.
Data from a 2026 Sleep Medicine study of 2,895 adults found that arousal-related behaviors — rumination, cognitive activation, anxiety-driven wakefulness — were the most discriminating factor between people with and without chronic insomnia (AUC = 0.824), more prevalent than caffeine or alcohol misuse. Stimulus control directly addresses this pattern.
4. Bedroom Temperature
Core body temperature naturally declines as part of the sleep-onset process. A cool bedroom environment supports this decline. Most sleep research points to 65–68°F (18–20°C) as the optimal range for most adults, with cooler temperatures associated with longer periods of slow-wave (deep) sleep.
This is a relatively easy environmental modification and worth prioritizing if your current sleeping environment is warm. The mechanism is direct: a cooler ambient temperature reduces the work the body has to do to lower its core temperature, facilitating the transition into sleep.
5. Substance Timing: Caffeine and Alcohol
Caffeine works by blocking adenosine receptors — it does not eliminate adenosine, it just prevents you from feeling its accumulating effect. The adenosine is still building. When caffeine clears, that accumulated pressure hits suddenly, which is one reason an afternoon coffee can still impair sleep even if you do not feel stimulated at bedtime. Research suggests avoiding caffeine after noon increases the likelihood of falling asleep at your intended time.
Alcohol is frequently misunderstood as a sleep aid because it produces sedation. It does help some people fall asleep faster. But it disrupts sleep architecture across the night: it suppresses REM sleep, causes mid-night awakenings as it is metabolized, and can worsen snoring. A 2025 systematic review found these disruptive effects occur even at low doses. Alcohol-assisted sleep is lighter, more fragmented, and less restorative than unassisted sleep.
6. Wind-Down Relaxation
The transition from wakefulness to sleep requires a reduction in cognitive and physiological arousal. Two specific techniques have meaningful research support.
First, writing a specific to-do list before bed. A polysomnographic study by Scullin et al. (2018) found that spending five minutes writing a list of tasks to be completed in the coming days — rather than journaling about completed activities — significantly shortened sleep onset latency. The proposed mechanism is cognitive offloading: externalizing pending tasks reduces the mental rehearsal loop that keeps many people awake.
Second, a warm bath or shower 60–90 minutes before bed. The mechanism here is counterintuitive: warm water causes blood vessels in the hands and feet to dilate, which accelerates the transfer of heat away from the body's core. This drop in core temperature is a physiological signal that facilitates sleep onset. A systematic review and meta-analysis of 13 trials (Haghayegh et al., 2019, Sleep Medicine Reviews) found that water-based passive body heating at 40–42.5°C, scheduled 1–2 hours before bedtime, was associated with a meaningful reduction in sleep onset latency — approximately 36% — along with improved sleep quality and efficiency.
| Behavioral Pillar | Biological Process Supported | Evidence Strength | Time to Effect |
|---|---|---|---|
| Consistent wake time | Process S + Process C | Very strong — RCT and longitudinal data | 1–2 weeks |
| Light exposure management (morning + evening) | Process C (circadian phase) | Strong — mechanistic and RCT evidence | Days to 1–2 weeks |
| Stimulus control (CBT-I component) | Arousal / conditioned wakefulness | Strong — formal CBT-I evidence base | 2–4 weeks |
| Bedroom temperature (65–68°F) | Core temperature decline | Moderate — observational and experimental | Immediate to 1 week |
| Substance timing (caffeine before noon; limit alcohol) | Process S (adenosine); REM architecture | Moderate to strong — systematic review support | 1–3 days |
| Wind-down relaxation (to-do list; warm bath) | Cognitive and physiological arousal | Moderate — RCT support for both specific techniques | Days to 2 weeks |
Building Your 60-Minute Pre-Sleep Routine: A Step-by-Step Framework
The behaviors above become most effective when sequenced into a consistent pre-sleep window. The following framework structures the 60 minutes before your target bedtime into a practical, mechanistically grounded routine. The steps are ordered to address the highest-leverage variables first.

T-60 minutes: Begin the wind-down
- Dim the lights throughout your home. Bright overhead lighting suppresses melatonin. Switching to lower-intensity, warmer-toned lamps signals to the SCN that evening is progressing. This is more effective than relying solely on night mode on your devices.
- Turn off screens or move to passive, low-engagement content only. The goal is to reduce both blue light exposure and cognitive stimulation simultaneously. If you use a device, reduce brightness to its lowest setting and avoid content that generates emotional engagement or decision-making.
- Write your to-do list for the next day. Take five minutes to write down specific tasks you need to complete tomorrow. This is not journaling — it is forward-looking task capture. The Scullin et al. (2018) research found this specific format shortens sleep onset latency by externalizing the mental agenda that otherwise replays at bedtime.
T-60 to T-90 minutes before bed: Warm bath or shower
If you plan to take a warm bath or shower, this is the optimal window. Water temperature of 40–42.5°C (104–108°F) for at least 10 minutes initiates the vasodilation response in the hands and feet that accelerates core temperature decline. Timing matters: taking the bath or shower too close to bedtime does not allow sufficient time for the temperature drop to occur before you lie down.
T-30 minutes: Low-stimulation activity
- Read a physical book or low-engagement material in dim light. Reading serves as a cognitive bridge — it occupies the mind enough to prevent rumination without generating the arousal associated with screens or emotionally charged content.
- Prepare your bedroom environment. Set the thermostat to 65–68°F if possible. Ensure the room is dark — blackout curtains or an eye mask eliminate light that would otherwise reach the retina during sleep. Address noise with earplugs or a white noise source if your environment is not reliably quiet.
- Optional: a brief relaxation practice. Progressive muscle relaxation, slow diaphragmatic breathing, or a body scan are low-evidence in terms of large RCTs but have plausible physiological rationale (reducing sympathetic nervous system activation) and are low-risk. If you find them helpful, they fit well in this window. Chamomile tea, aromatherapy, and similar comfort practices have minimal controlled research support — they may help via placebo or comfort mechanisms, but should not be treated as evidence-based interventions.
Key do-not-do items for the pre-sleep window
- Do not check email or work messages after T-60. Cognitive engagement with unresolved tasks is one of the most reliable ways to delay sleep onset.
- Do not eat a large meal. Digestion increases core body temperature and metabolic activity at a time when both need to decline.
- Do not exercise vigorously. Intense exercise raises core temperature and heart rate. Moderate exercise earlier in the day improves sleep quality; vigorous late-evening exercise can delay it.
- Do not lie in bed awake for more than 20 minutes. If sleep does not come, apply stimulus control: get up, move to another room, do something quiet in dim light, and return when genuinely sleepy.
When Sleep Hygiene Is Not Enough: Recognizing Chronic Insomnia
Sleep hygiene education has a real but limited role in treating insomnia. Understanding that limit is as important as understanding the behaviors themselves.
A 2025 systematic review and meta-analysis published in Sleep Medicine Reviews analyzed 42 randomized controlled trials involving 4,245 adults. The pooled results showed that sleep hygiene education produced meaningful pre-to-post improvement in insomnia severity — but was significantly inferior to CBT-I, partial CBT-I, exercise, and even acupressure as standalone interventions. The mean difference in Insomnia Severity Index scores between sleep hygiene education and CBT-I was 3.8 points, favoring CBT-I.
The American Academy of Family Physicians (AAFP) 2024 guidance is unambiguous: CBT-I is the first-line treatment for chronic insomnia. The American Academy of Sleep Medicine (AASM) states that the evidence for sleep hygiene alone is weak and recommends it be used alongside the other components of CBT-I rather than as a standalone intervention. The VA/DoD 2025 Clinical Practice Guideline for Chronic Insomnia similarly recommends against single-component sleep hygiene education for chronic insomnia.
The relationship between sleep hygiene and CBT-I is worth clarifying. Within CBT-I, sleep hygiene education is one of five components — the others being stimulus control, sleep restriction, cognitive restructuring, and relaxation training. Sleep restriction alone is identified as the most effective single component. This means that practicing sleep hygiene within a CBT-I framework is valuable and appropriate; practicing sleep hygiene in isolation and expecting CBT-I-level outcomes is not.
- Escalation signal: Sleep difficulties have persisted for three or more months despite consistent hygiene practice.
- Escalation signal: Sleep problems are causing significant daytime impairment — cognitive difficulty, mood disruption, or functional limitations at work or in relationships.
- Escalation signal: You are developing anxiety about sleep itself — clock-watching, dreading bedtime, or preoccupying thoughts about whether you will sleep.
- Escalation signal: A bed partner has observed pauses in your breathing, gasping, or loud snoring — these may indicate obstructive sleep apnea, which requires clinical evaluation independent of hygiene.
Common Myths and Misconceptions
Myth 1: You can catch up on sleep over the weekend
The 2023 National Sleep Foundation consensus statement suggests that after a week of insufficient sleep, some recovery sleep on weekends may be beneficial. This is a nuanced finding, not a blanket endorsement of sleeping in on weekends.
Significantly extending weekend sleep — by two hours or more — shifts your circadian phase later, creating a pattern sometimes called social jet lag. When Monday arrives, your body clock is misaligned with your required wake time, making the early week harder. Consistent daily wake time remains the priority. Limited recovery sleep after a genuinely insufficient week is a pragmatic acknowledgment of human variability, not a recommended strategy.
Myth 2: Alcohol helps you sleep
Alcohol produces sedation, which is different from sleep. It suppresses REM sleep in the first half of the night and causes a rebound effect in the second half — increased wakefulness, lighter sleep, and more fragmentation. These effects occur even at low doses. If you regularly use alcohol to fall asleep, the sleep you are getting is measurably less restorative than alcohol-free sleep.
Myth 3: Night mode on your phone solves the evening light problem
Blue light filtering apps and night mode settings reduce short-wavelength light output. They do not reduce screen brightness, and they do not reduce the cognitive stimulation generated by engaging content. Both total light intensity and what you are doing on the screen matter independently of wavelength. A 2024 National Sleep Foundation review found insufficient evidence to attribute sleep disruption specifically to blue light wavelengths when controlling for overall light intensity and content engagement. Night mode is a partial measure, not a complete solution.
Myth 4: Staying in bed will eventually make you sleep
Lying awake in bed for extended periods does the opposite of what most people intend. It trains the brain to associate the bed with wakefulness and frustration rather than with sleep. This is precisely the pattern that stimulus control therapy is designed to reverse. The discomfort of getting out of bed when you cannot sleep is real — but staying in bed and hoping for sleep to arrive is one of the most counterproductive behaviors for people with persistent insomnia.
How to Start: Implementation Without Overwhelm
The most common mistake in implementing sleep hygiene changes is attempting too many simultaneously. Behavioral change is more durable when introduced incrementally. Starting with one or two modifications — ideally consistent wake time and evening light reduction, since these have the highest leverage — and holding them for two weeks before adding more gives you enough time to observe a real effect without creating an unsustainable overhaul.
A simple sleep diary kept for two weeks is one of the most useful tools available. Record your approximate bedtime, wake time, estimated time to fall asleep, any nighttime awakenings, and a subjective quality rating. This gives you a baseline and makes it easier to identify which changes are producing measurable improvement — and which are not.
- Start with one or two changes, not the full list. Consistent wake time and evening light management are the highest-leverage starting points.
- Keep a two-week sleep diary to track what is changing and what is not.
- Set realistic expectations: sleep schedule consistency and light management typically take one to two weeks to produce measurable change. Bedroom environment changes may produce faster results.
- Forgive slip-ups. Missing a few nights does not erase progress. Return to the practice the following night without extending the disruption.
Supports these guides
Spot an error or have clinical feedback?
Because this article covers clinical, medication, or safety information, we use a moderated correction channel instead of open public comments. Let us know if something about “Sleep Hygiene Fundamentals and an Evidence-Based Bedtime Routine” needs a closer look.
Send feedback on this article