Sleep Apnea FAQ: Symptoms, Diagnosis, CPAP, and When to See a Doctor

Quick-Answer Summary: What You Need to Know About Sleep Apnea
- Sleep apnea causes breathing to stop (apnea) or become severely restricted (hypopnea) during sleep, often dozens or hundreds of times per night.
- Snoring is not required for OSA — many people with sleep apnea, especially women, never snore loudly.
- Diagnosis requires a sleep test — either a home sleep apnea test (HSAT) or an in-lab polysomnography (PSG). Symptoms alone are not sufficient to confirm OSA.
- CPAP (continuous positive airway pressure) is the AASM-recommended first-line treatment for all severity levels of OSA.
- Other options — oral appliances, hypoglossal nerve stimulation, and the recently FDA-approved tirzepatide — expand the treatment landscape for patients who cannot tolerate CPAP or have obesity as a contributing factor.
- If you feel unrefreshed after a full night's sleep, or a bed partner has noticed breathing pauses, a conversation with your primary care physician is the right first step.
What Is Sleep Apnea? OSA, CSA, Apneas, and Hypopneas Explained
Sleep apnea is defined by repeated interruptions to breathing during sleep. There are two main types, and understanding the difference matters for diagnosis and treatment.
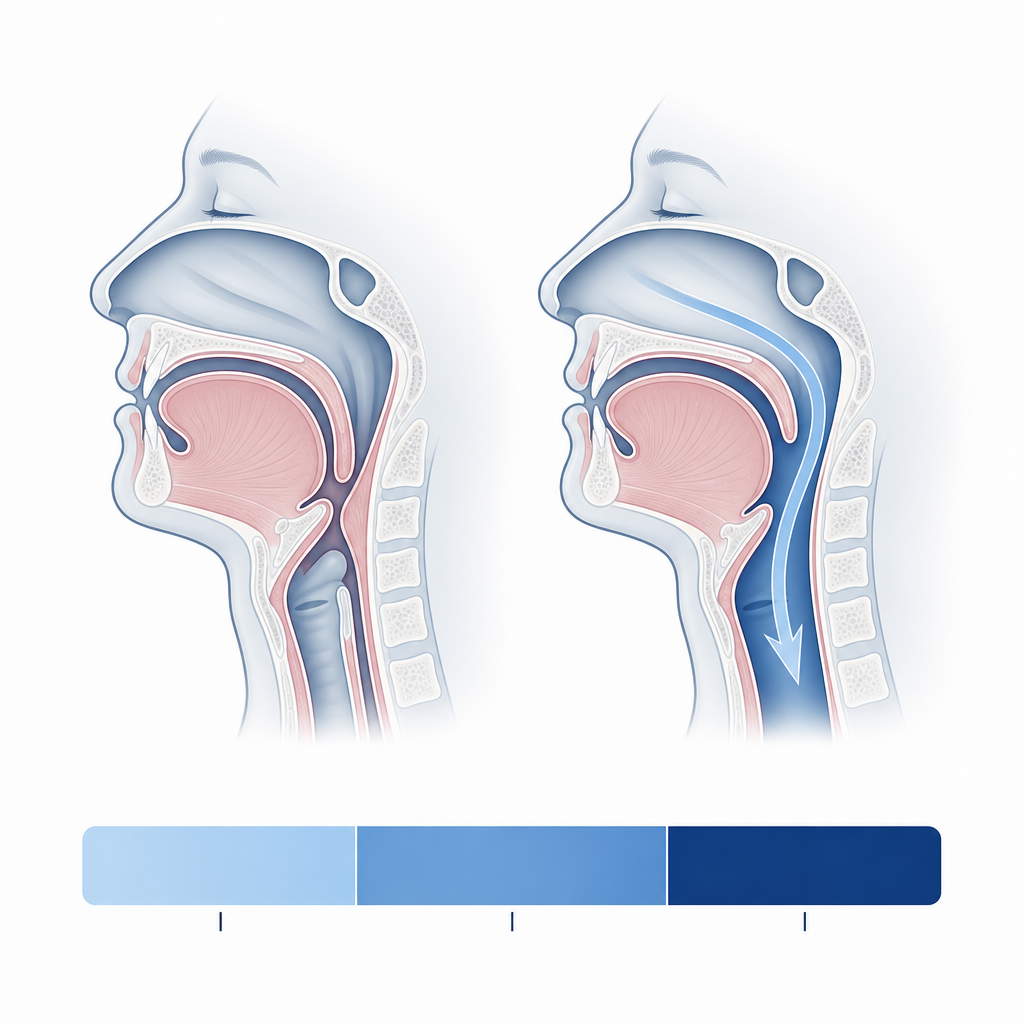
Obstructive sleep apnea (OSA) is by far the more common form. It occurs when the muscles of the upper airway relax during sleep, allowing soft tissue — including the tongue, soft palate, and throat walls — to collapse inward and block airflow. The brain eventually registers the oxygen drop and triggers a brief arousal (often too short to remember) that restores normal breathing. This cycle can repeat hundreds of times per night without the person ever waking fully.
Central sleep apnea (CSA) is a different and less common condition. In CSA, the airway itself is not blocked — instead, the brain temporarily fails to send the correct signals to the breathing muscles. CSA requires specialist evaluation and different treatment approaches than OSA. This FAQ focuses primarily on OSA, which is what the vast majority of people searching these questions are dealing with.
A mixed or complex type — combining obstructive and central features — also exists but is less common and typically identified during formal sleep testing.
Two terms appear throughout any sleep apnea discussion and are worth defining precisely:
- Apnea: A complete stop in airflow lasting at least 10 seconds.
- Hypopnea: A partial reduction in airflow — not a complete stop — accompanied by either a measurable drop in blood oxygen or a brief arousal from sleep.
Both events count toward the apnea-hypopnea index (AHI), which is the primary measure used to diagnose and classify OSA severity. The AHI represents the average number of apnea and hypopnea events per hour of sleep.
Symptoms: What Does Sleep Apnea Actually Feel Like?
OSA symptoms fall into two distinct clusters. The classic picture is well-known. The atypical picture — far more common in women and postmenopausal individuals — is frequently missed, leading to years of misdiagnosis.
Classic Symptoms
- Loud, persistent snoring (often noticed by a bed partner before the person themselves)
- Witnessed breathing pauses during sleep
- Gasping or choking sounds when resuming breathing
- Excessive daytime sleepiness — falling asleep during routine activities, not just when tired
- Waking with a dry mouth or sore throat
- Morning headaches
- Nocturia (waking repeatedly to urinate)
- Difficulty concentrating, memory problems, or irritability
Atypical Symptoms in Women and Postmenopausal Individuals
Women with OSA frequently do not fit the classic picture. Instead of loud snoring and witnessed apneas, they are more likely to present with symptoms that look like other common conditions — which is precisely why OSA is so often missed in this population.
- Insomnia or difficulty staying asleep (rather than obvious daytime sleepiness)
- Persistent fatigue that does not improve with more sleep
- Mood changes — depression, anxiety, or emotional lability
- Morning headaches
- Vivid or disturbing nightmares
- Night sweats and restlessness
Peer-reviewed research shows that women with OSA are frequently misdiagnosed and treated for depression, insomnia, or hypothyroidism — and are diagnosed with OSA later, when they are older and have higher BMI than male patients at the time of diagnosis. The diagnostic gap is not because women have milder disease — research indicates that women with OSA are not less symptomatic than men, even at relatively low AHI levels.
What Bed Partners May Notice
Bed partners often observe OSA before the person with the condition does. Clinically meaningful observations include witnessed breathing pauses (the partner watches the person stop breathing for several seconds), gasping or choking sounds when breathing resumes, and restless or fragmented sleep patterns.
Who Is at Risk? Risk Factors for Obstructive Sleep Apnea
OSA has a well-established risk factor profile, though it is important to note that the condition can affect people of any body size. Obesity increases risk significantly, but it is not a prerequisite.
- Excess weight and obesity: Fat deposits around the upper airway narrow the breathing passage, making collapse more likely during sleep.
- Male sex: Men are approximately 2–3 times more likely to have OSA than women before age 50, likely due to differences in airway anatomy, fat distribution, and hormonal factors.
- Advancing age: Airway muscle tone decreases with age, increasing the likelihood of collapse during sleep.
- Menopause: After menopause, women's OSA risk increases substantially — postmenopausal women close much of the sex gap. Hormonal changes appear to affect airway muscle tone and fat distribution.
- Anatomical factors: A large neck circumference (greater than 17 inches in men, greater than 16 inches in women), a naturally narrow airway, enlarged tonsils or adenoids, a recessed chin, or a deviated septum all increase risk.
- Family history: OSA has a heritable component, partly through shared anatomical traits.
- Alcohol and sedative use: These substances relax airway muscles further, worsening or triggering OSA even in people who are not otherwise at high risk.
- Smoking: Smoking causes upper airway inflammation and fluid retention, narrowing the airway.
- Nasal congestion: Chronic nasal obstruction forces mouth breathing and increases airway collapse risk.
- Comorbid conditions: Hypertension, type 2 diabetes, heart failure, polycystic ovary syndrome (PCOS), and thyroid disorders are all associated with elevated OSA prevalence.
Diagnosis: How Is Sleep Apnea Detected and Confirmed?
Diagnosis begins with a clinical evaluation — not a sleep test. Your doctor will take a detailed sleep history, ask about symptoms (and ideally hear from a bed partner if one is available), administer screening questionnaires, and conduct a physical examination of the upper airway.
Screening Questionnaires
Two tools are commonly used before formal sleep testing:
- STOP-Bang questionnaire: Eight yes/no questions covering snoring, tiredness, observed apneas, blood pressure, BMI, age, neck circumference, and sex. A score of 3 or higher indicates elevated OSA risk. Note that STOP-Bang performs better for men than women at standard cutoffs — research suggests gender-specific cutoffs improve its accuracy in female patients.
- Epworth Sleepiness Scale: Rates the likelihood of falling asleep in eight everyday situations. A score above 10 suggests excessive daytime sleepiness warranting further evaluation.
Home Sleep Apnea Test (HSAT)
A home sleep apnea test records airflow, blood oxygen saturation, breathing effort, heart rate, and body position during a night of sleep in your own bed. For moderate-to-severe OSA, HSATs are approximately 90% accurate — making them a reasonable first-line diagnostic tool when OSA is the primary clinical suspicion and no other sleep disorder is suspected.
However, home tests have a meaningful limitation that is worth understanding mechanistically. Most home sleep devices calculate the AHI using total recording time as the denominator rather than total sleep time. Because the device cannot confirm when you are actually asleep versus awake and lying still, it spreads the apnea events over a longer time window — which can underestimate the true AHI by at least 20%. A person with a true AHI of 15 might receive a home test result of 12, shifting their classification from moderate to mild.
In-Lab Polysomnography (PSG)
Polysomnography is the gold standard for sleep apnea diagnosis. Conducted in a sleep lab, PSG adds EEG brain wave monitoring, full sleep stage classification (light sleep, deep sleep, REM), and leg movement tracking to the respiratory measurements captured by a home test. This broader data set allows clinicians to detect other sleep disorders — restless legs syndrome, REM sleep behavior disorder, narcolepsy — that a home test cannot identify.
PSG is typically recommended when: the home test result is unclear or inconsistent with symptoms, a complex case is suspected, another sleep disorder may be present, or the home test was negative but clinical suspicion remains high.
Understanding Your AHI Score
| AHI (events per hour) | Severity | Clinical meaning |
|---|---|---|
| Fewer than 5 | Normal | OSA is not diagnosed in adults at this threshold |
| 5 to 14 | Mild OSA | Treatment is typically recommended, especially with symptoms or cardiovascular comorbidities |
| 15 to 29 | Moderate OSA | Treatment is clearly indicated; CPAP is first-line |
| 30 or more | Severe OSA | Urgent treatment indicated; highest cardiovascular risk |
Treatment: From CPAP to Newer Options — What Actually Works?
OSA treatment has expanded considerably in recent years. CPAP remains the cornerstone, but there are now several well-validated alternatives and one newly approved medication for a specific patient population.
CPAP: The First-Line Standard
Continuous positive airway pressure (CPAP) is the AASM-recommended first-line treatment for all severity levels of OSA. The device delivers a steady stream of pressurized air through a mask worn during sleep. Mechanically, this column of pressurized air acts as a pneumatic stent — it keeps the airway open from within, preventing the soft tissue collapse that causes apneas and hypopneas.
Three device types are used clinically:
- CPAP (fixed pressure): Delivers a single, constant air pressure set by a clinician based on titration study results.
- APAP (auto-adjusting): Automatically adjusts pressure breath-by-breath within a prescribed range, responding to detected airway resistance. Many patients find APAP more comfortable, particularly when pressure needs vary with sleep position or REM sleep.
- BiPAP (bilevel positive airway pressure): Delivers different pressures for inhalation and exhalation. Used when standard CPAP pressure is too high for the patient to exhale comfortably, or in cases of central apnea components.
Common CPAP Problems and Practical Solutions
| Common problem | Practical approach |
|---|---|
| Mask leaks or discomfort | Mask fitting is highly individual — trying multiple mask styles (nasal pillow, nasal, full-face) with a qualified equipment provider is essential before concluding CPAP is intolerable |
| Pressure feels too high | Switching from fixed CPAP to APAP, or adjusting the prescribed range, can significantly reduce the sensation of fighting the machine |
| Dry mouth or nasal dryness | Heated humidification is built into most modern devices and substantially reduces mucosal dryness; a chinstrap can help if mouth breathing is the source |
| Claustrophobia or anxiety with the mask | Desensitization — wearing the mask while awake before attempting sleep — combined with behavioral support can improve tolerance over time |
| Difficulty sleeping with the device | Initial discomfort is common; most patients who continue through the first 2–4 weeks report meaningful improvement in both comfort and sleep quality |
Real-world CPAP adherence averages roughly 40–60% in clinical studies — meaning a meaningful proportion of patients do not consistently use their devices after the first month. Modern APAP technology, heated humidification, and improved mask fitting options have increased tolerance compared to earlier generations of equipment.
Oral Appliance Therapy
For patients with mild-to-moderate OSA, or for those who cannot tolerate CPAP, a custom-fitted oral appliance is the recommended second-line treatment. The most common type is a mandibular advancement device (MAD) — a custom-made mouthguard that holds the lower jaw slightly forward during sleep, which in turn keeps the tongue and soft tissue from collapsing into the airway.
Oral appliances must be fitted by a dentist or oral medicine specialist trained in dental sleep medicine. Over-the-counter boil-and-bite devices are not equivalent to custom-fitted appliances and are not recommended as a substitute.
Hypoglossal Nerve Stimulation (Inspire)
Hypoglossal nerve stimulation is an implanted device that delivers mild electrical stimulation to the hypoglossal nerve — the nerve that controls tongue movement — during sleep. By keeping the tongue in a forward position, it prevents the airway obstruction that drives OSA.
This option is FDA-approved for moderate-to-severe OSA in patients who cannot tolerate CPAP and who meet specific eligibility criteria:
- AHI between 20 and 50 events per hour
- BMI of 32 or below
- Fewer than 25% central or mixed apneas
- No complete concentric collapse at the palate on drug-induced sleep endoscopy (a pre-surgical evaluation)
In clinical follow-up, median AHI has been shown to decrease by approximately 68% at 12 months in eligible patients — from around 29 to 9 events per hour. This is a surgical procedure with a meaningful evaluation process; it is not appropriate for all OSA patients, but it represents an important option for those who genuinely cannot use CPAP.
Tirzepatide (Zepbound): What the 2024 FDA Approval Actually Means
In 2024, the FDA approved tirzepatide (brand name Zepbound) for the treatment of moderate-to-severe OSA in adults with obesity. Clinical trials showed that tirzepatide reduced AHI by approximately 50% in this population — a meaningful result that reflects the medication's mechanism: by reducing body weight, it addresses one of the root causes of airway narrowing in people with obesity-related OSA.
Lifestyle Changes as Adjunctive Measures
Several lifestyle changes reduce OSA severity and are recommended alongside — not instead of — primary treatment:
- Weight loss: Meaningful weight reduction decreases OSA severity in people with obesity, but rarely fully resolves OSA — and OSA can recur with weight regain.
- Positional therapy: OSA is often worse when sleeping on the back (supine position). Sleeping on the side reduces airway collapse for some patients. Positional therapy devices help maintain a side-sleeping position.
- Avoiding alcohol and sedatives before bed: Both relax airway muscles and worsen OSA severity.
- Quitting smoking: Reduces upper airway inflammation over time.
Lifestyle changes are rarely sufficient as a standalone treatment except in very mild OSA, but they can meaningfully reduce the pressure settings needed for CPAP to be effective and improve overall treatment outcomes.
When Should You See a Doctor About Sleep Apnea?
These specific situations warrant a clinical evaluation for sleep apnea:
- You consistently feel unrefreshed after 7–8 hours of sleep, and this has persisted for more than a few weeks
- A bed partner has witnessed you stop breathing during sleep
- You wake gasping or choking
- You experience severe daytime sleepiness — falling asleep during conversations, while driving, or during routine tasks
- You wake regularly with morning headaches
- You have persistent fatigue, mood changes, or insomnia that has not responded to standard interventions — particularly if you are a woman or postmenopausal individual, given the frequency with which these symptoms are misattributed to other conditions
Who to See
Start with your primary care physician. They can order a home sleep test or refer you to the appropriate specialist. Depending on your presentation, you may be referred to:
- Sleep medicine specialist: For complex cases, unclear home test results, or suspected additional sleep disorders
- Pulmonologist: When respiratory complications or lung disease are present
- Cardiologist: When atrial fibrillation, heart failure, or treatment-resistant hypertension is the entry point
- Neurologist: When stroke history or central apnea components are suspected
- Mental health professional: When mood symptoms are prominent — but ideally after OSA has been ruled out or treated, since untreated OSA directly worsens depression and anxiety
What Happens If Sleep Apnea Goes Untreated?
Untreated OSA is not simply a quality-of-life problem. Each apnea event causes a brief oxygen drop and a stress response — a surge of cortisol and adrenaline that raises heart rate and blood pressure. Repeated hundreds of times per night over years, this physiological stress accumulates into measurable systemic harm.
- Hypertension: OSA is one of the most common reversible causes of high blood pressure, including treatment-resistant hypertension that does not respond to multiple medications.
- Atrial fibrillation: OSA is strongly associated with AFib onset and recurrence. Treating OSA reduces AFib recurrence rates.
- Type 2 diabetes and metabolic syndrome: Chronic intermittent hypoxia impairs insulin sensitivity and glucose regulation.
- Stroke: OSA significantly increases stroke risk through multiple pathways including hypertension, atrial fibrillation, and direct vascular effects.
- Heart failure: The repeated pressure changes in the chest during obstructed breathing strain the heart over time.
- Cognitive decline: Emerging evidence links chronic OSA to accelerated cognitive decline and increased dementia risk, likely through the combined effects of chronic sleep fragmentation and intermittent hypoxia on brain tissue.
It is also worth noting that untreated OSA produces a form of chronic sleep deprivation — not because you sleep too few hours, but because the sleep you get is severely fragmented and non-restorative. Understanding how many hours of sleep adults actually need is a useful baseline, but for someone with untreated OSA, hours in bed does not translate to adequate rest.
Next Steps: Where to Go From Here
If you have read this FAQ and recognize your symptoms — or a bed partner's — the most important next step is a conversation with your primary care physician. Bring a list of your symptoms, note how long they have been present, and mention any relevant comorbidities. A home sleep test can often be ordered at that first visit.
For deeper reading on this site:
- Symptom triage and condition detail: Visit the Sleep Conditions section for the full clinical reference page on obstructive sleep apnea, including diagnostic criteria, treatment hierarchy, and when to escalate to a specialist.
- Behavioral and adjunctive strategies: The Sleep Hygiene & Routines section covers positional therapy, alcohol timing, and other adjunctive behavioral approaches that complement OSA treatment.
- Understanding the science: The Sleep Science section explains sleep architecture, oxygen desaturation events, and the physiological mechanisms behind why fragmented sleep causes the symptoms you may be experiencing.
- Supplement and aid safety: If you are considering OTC sleep aids while navigating diagnosis, the Sleep Aids section covers population-specific safety notes — including why sedating antihistamines can worsen OSA severity.