Mechanism explainer
Circadian Rhythm and Light Exposure: How Light Affects Sleep
Light is the most powerful signal controlling when your body clock tells you to sleep — and its effects depend on timing, intensity, and wavelength across the entire day, not just evening screen habits. This guide explains the biology behind light-driven circadian anchoring and translates it into a practical daily light protocol for adults who want deeper, better-timed sleep.

Light Is the Primary Lever — Not Supplements, Not Trackers
Most sleep advice concentrates on what to avoid in the evening — blue light, caffeine, screens. That advice is not wrong, but it addresses only half the problem. The more powerful and less discussed intervention happens in the morning, and it requires nothing more than getting outside.
Light is the single most powerful signal your body uses to set its internal clock. Not melatonin supplements. Not sleep trackers. Not wind-down routines. The timing, intensity, and wavelength of light you encounter across the full day — from the moment you wake to the moment you fall asleep — determines whether your circadian rhythm is well-anchored or gradually drifting toward later, fragmented, or misaligned sleep.
This guide explains the biology behind that claim, then translates it into a structured daily light protocol. The goal is to replace generic advice with specific, dose-response behavioral levers that you can act on today.
How Light Signals the Brain's Clock: ipRGCs, Melanopsin, and the SCN
Your eye contains a dedicated, non-visual pathway whose sole purpose is to tell your brain what time of day it is. This pathway begins with a specialized class of retinal cells called intrinsically photosensitive retinal ganglion cells (ipRGCs). Unlike the rods and cones that handle vision, ipRGCs contain a photopigment called melanopsin, which is most sensitive to light around 480 nanometers — the short-wavelength, blue-green portion of the visible spectrum.
When light hits these cells, they send signals along the retinohypothalamic tract directly to the suprachiasmatic nucleus (SCN) in the hypothalamus — a paired cluster of roughly 20,000 neurons that functions as the body's master pacemaker. The SCN then coordinates downstream signals that govern cortisol release, core body temperature, melatonin onset, and dozens of other physiological rhythms.
One critical nuance: ipRGCs are not isolated sensors. They also receive input from rods and cones, which means they act as integrators of the entire light environment across a broad range of wavelengths. The practical implication is significant: total light level matters, not just blue light alone. Filtering blue wavelengths without reducing overall brightness has a much smaller effect on the circadian system than simply dimming the light source.
The SCN runs on a molecular feedback loop — involving genes including CLOCK, BMAL1, PER, and CRY — that generates an internal rhythm of approximately 24 hours. Light exposure via ipRGCs is what resets and synchronizes this loop to the actual solar day. For a detailed account of the molecular oscillator and how it interacts with the homeostatic sleep drive, see the companion article on circadian rhythm mechanisms and how your body clock controls sleep and wake cycles. This article focuses on light as the intervention — how to use it, when, and at what dose.
The Phase Response Curve: Why Timing Determines When You Can Fall Asleep
The most important concept for understanding how to use light behaviorally is the phase response curve (PRC). It describes how the circadian clock responds to light at different times of day — and the response is not uniform. The same light source, at different times, produces opposite effects on your sleep timing.
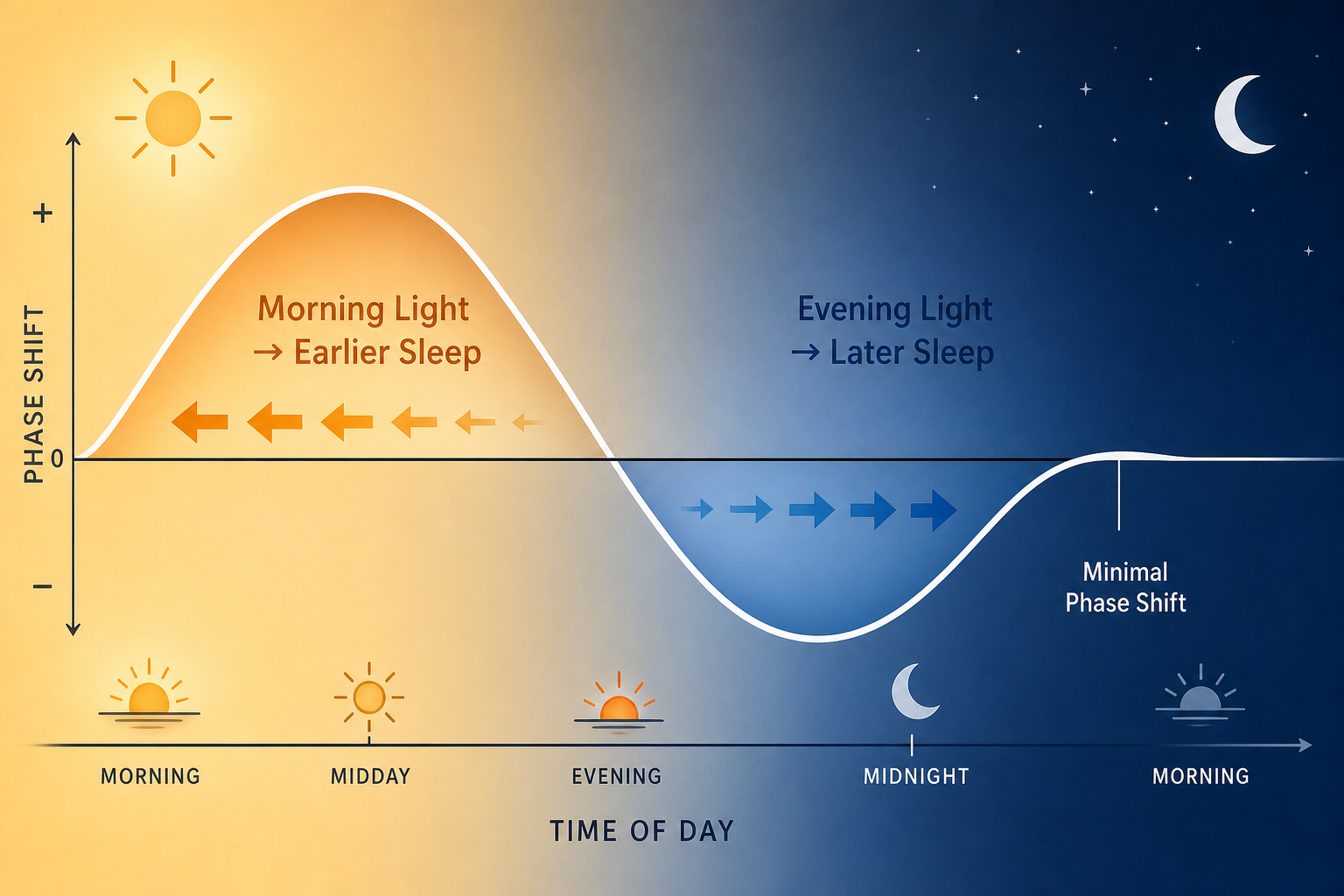
The pattern works as follows:
- Morning light (around wake time and the hours following) advances the clock — it shifts sleep onset and wake time earlier. Morning light can shift the circadian system approximately 1 hour earlier per day.
- Early evening light (roughly 2 hours before and after habitual bedtime) delays the clock — it pushes sleep onset and wake time later. Evening light can shift the circadian system approximately 2 hours later per day.
- Light in the late biological night (after roughly 3 a.m.) causes a phase advance — the same direction as morning light, but from an unusual timing that can disrupt the following night's sleep.
- Midday light has the smallest effect on clock timing, though it still contributes to the photic history effect described below.
This asymmetry — evening light being roughly twice as powerful at shifting the clock as morning light — is why modern adults so commonly drift toward later sleep timing. Indoor environments in the evening are often bright enough to delay the clock, while morning environments are often dim enough to provide no corrective advance. The result is a slow, chronic phase delay that makes falling asleep at a reasonable hour genuinely difficult, not just a matter of willpower.
The Three Variables That Determine Circadian Impact: Wavelength, Intensity, and Photic History
Not all light affects the circadian system equally. Three independent variables determine how strongly any given light exposure shifts your clock or suppresses melatonin.
Wavelength
Melanopsin in ipRGCs peaks at approximately 480 nm — short-wavelength blue-green light. This is why the circadian system is more sensitive to cool white LED and fluorescent light sources, which are rich in short wavelengths, than to warm or incandescent sources.
Research on home lighting types found that cool white LED lamps induced considerably greater melatonin suppression than warm white LED, warm white CFL, or incandescent lamps. Tunable LED lamps adjusted to a warm 2100 K color temperature reduced estimated melatonin suppression to near zero compared to the same lamp at a cool 5700 K setting. However, because ipRGCs integrate rod and cone signals across wavelengths, wavelength is only one variable — intensity and timing remain equally important.
Intensity (Lux)
Lux is the measure of light intensity reaching the eye. The difference between indoor and outdoor environments is far larger than most people appreciate — and it has direct consequences for circadian anchoring.

| Light Environment | Approximate Lux | Circadian Significance |
|---|---|---|
| Bedroom at night (minimal sources) | < 10 lux | Even this level can fragment slow-wave sleep and suppress melatonin |
| Standard indoor office | 200–500 lux | Insufficient for strong circadian entrainment |
| Cloudy outdoor daylight | ~10,000 lux | Effective for morning anchoring |
| Light therapy lamp (clinical-grade) | 7,000–10,000 lux | Validated substitute for outdoor morning light |
| Clear outdoor daylight | 25,000–100,000 lux | Maximum circadian signal; ideal for morning exposure |
Photic History
The circadian system's sensitivity to light is not fixed — it depends on how much light you have already seen that day. This is the photic history effect: bright daytime light exposure reduces the circadian system's sensitivity to evening light, making the same evening light source less disruptive.
This creates a second, independent reason to prioritize morning bright light — beyond its direct clock-advancing effect. People who spend most of their day in dim indoor environments arrive at evening with a highly light-sensitive circadian system, making ordinary household lighting far more clock-disrupting than it would be for someone who had spent time outdoors during the day.
Morning Light: The Highest-Leverage Circadian Anchor
Of all the behavioral changes covered in this article, morning light exposure has the strongest and most consistent evidence base. It works through two mechanisms simultaneously: it directly advances the circadian clock (phase advance), and it builds the photic history that buffers against evening light disruption.
Population-level data from Roenneberg and colleagues found that each additional hour spent outdoors during the day was associated with approximately 30 minutes of earlier sleep timing. A 2025 cross-sectional study of 1,762 adults found that every 30-minute increment of morning sunlight before 10 a.m. was associated with a 23-minute reduction in sleep midpoint — meaning earlier, better-timed sleep — along with significantly improved overall sleep quality scores.
The same study found that afternoon sun (after 3 p.m.) also reduced sleep midpoint, though less strongly, while midday exposure showed no significant association with sleep timing. This pattern is consistent with the phase response curve: morning and late-afternoon exposures fall on the advance-promoting portion of the curve, while midday light has minimal phase-shifting effect.
Evidence-based recommendations from Brown et al. (2022, PLoS Biology), cited as the primary authority in the 2025 sunlight study, specify outdoor light exposure within the first 30–60 minutes of waking, targeting intensities above 1,000 lux — a threshold easily met outdoors even on overcast days, but rarely reached by indoor lighting.
When Outdoor Morning Light Isn't Possible
Indoor workers, people in northern latitudes during winter, and those with early morning schedules that precede sunrise all face a genuine barrier to outdoor morning light. Light therapy lamps rated at 7,000–10,000 lux are a validated substitute. The standard protocol is 30–60 minutes of exposure in the morning, positioned within the lamp's recommended distance (typically 16–24 inches from the face), with eyes open and directed toward — but not directly at — the lamp.
- Outdoor exposure within 30–60 minutes of waking is the first choice. Even a 10-minute walk outside on a cloudy day provides far more lux than indoor environments.
- A 10,000-lux light therapy lamp for 20–30 minutes is a clinically validated substitute for days when outdoor access is impossible.
- Sitting near a window is better than nothing but delivers substantially less light than direct outdoor exposure, particularly in winter or in rooms with north-facing windows.
- Timing matters more than duration: 15 minutes of outdoor light at 7 a.m. is more clock-advancing than 30 minutes at 10 a.m., because of where those times fall on the phase response curve.
Evening and Nighttime Light: Phase Delay, Melatonin, and Sleep Architecture
Artificial light in the evening affects sleep through two distinct mechanisms, and understanding both matters for choosing the right interventions.
The first is the phase delay mechanism: light in the 2-hour window around habitual bedtime shifts the circadian clock later, delaying melatonin onset and pushing the physiological window for sleep onset toward a later hour. Typical evening light exposure can delay the clock by up to 2 hours per day — a substantial shift that compounds over days if light habits remain consistent.
The second mechanism is more surprising. A controlled experiment published in PNAS found that one night of moderate room light (100 lux) during sleep — not just before sleep, but throughout the sleep period — increased next-morning insulin resistance and elevated sympathetic nervous system activity (measured by heart rate and sympathovagal balance). Critically, melatonin levels were similar in both the room-light and dim-light conditions. The effect was not primarily melatonin-mediated: it was driven by sympathetic nervous system activation that persisted throughout sleep and into the following morning.
This finding matters because it means the consequences of nighttime light exposure extend beyond sleep quality into metabolic function — and they occur at light levels (100 lux) that are common in many bedrooms with streetlights, nightlights, or partially covered windows.
Night Mode and Blue-Light Glasses: What the Evidence Actually Shows
Two popular interventions for evening light management deserve honest assessment, because both are frequently overstated.
- Dim screens to minimum brightness in the 2 hours before sleep — this has a larger circadian effect than enabling night mode at full brightness.
- Switch to warm-toned (2700 K or lower) bulbs in rooms used in the evening; cool white LEDs and CFLs suppress melatonin considerably more than warm or incandescent sources.
- Reduce overall room lighting intensity in the evening — a single dimmed lamp is preferable to overhead lighting at full intensity.
- If using BLF glasses for circadian purposes, look for brown-tinted lenses that specifically target the 460–530 nm range; standard clear BLF lenses are unlikely to provide meaningful benefit.
Downstream Consequences of Chronic Light Misalignment
Poor sleep quality is the most immediate consequence of chronic light misalignment, but it is not the only one. A growing body of evidence links nighttime light exposure to cardiovascular and metabolic outcomes that extend well beyond how rested you feel in the morning.
A large prospective cohort study of 88,905 UK Biobank participants, published in JAMA Network Open in October 2025, examined the relationship between nighttime light exposure and cardiovascular disease over approximately 9.5 years of follow-up. The findings showed a clear dose-response relationship: compared to those in the darkest 50th percentile of nighttime light exposure, participants in the 51st–70th percentile had 20% higher heart attack risk; those in the 71st–90th percentile had 27% higher risk; and those in the brightest 91st–100th percentile had 47% higher risk. Elevated risks were also observed for stroke, heart failure, atrial fibrillation, and coronary artery disease.
Critically, these associations were independent of sleep duration, smoking, alcohol consumption, diet, and physical activity. The mechanism implicated is circadian disruption itself — not sleep deprivation as an intermediary. The circadian system reaches peak light sensitivity between midnight and 6 a.m., meaning that even low-level light during this window carries disproportionate biological weight.
The experimental PNAS findings add a mechanistic layer: a single night of 100-lux room light during sleep increased insulin resistance and sympathetic nervous system activation the following morning. This is a direct, measurable physiological effect from one night of ordinary bedroom light — not a cumulative statistical association. Together, these findings make a strong case for treating sleep environment darkness as seriously as sleep duration.
A Practical Daily Light Protocol
The following protocol consolidates the evidence across the article into a time-anchored daily structure. Lux targets and timing windows are drawn from the Brown et al. 2022 (PLoS Biology) recommendations referenced in the 2025 sunlight study, supplemented by the experimental and cohort data reviewed above.
| Time Window | Target | Lux Goal | Practical Action |
|---|---|---|---|
| Wake to 60 minutes after waking | Morning anchor — phase advance | > 1,000 lux (outdoor); 7,000–10,000 lux (therapy lamp) | Step outside immediately after waking; 10–30 minutes minimum. Use a 10,000-lux therapy lamp if outdoor access is unavailable. |
| Mid-morning to early afternoon | Maintain photic history | As high as possible; outdoor preferred | Work near windows, take outdoor breaks, or use a bright workspace. Reduces evening light sensitivity. |
| 2 hours before habitual bedtime | Begin light reduction | < 100 lux; warm color temperature | Switch to warm-toned (≤ 2700 K) lamps at low intensity. Avoid overhead lighting. Dim screens to minimum. |
| 1 hour before sleep | Minimize clock-disrupting light | < 10 lux; warm sources only | Use a single dim warm lamp or candlelight equivalent. Avoid screens if possible; if used, minimum brightness only. |
| Sleep environment | Near-complete darkness | < 3 lux throughout the sleep period | Blackout curtains or a sleep mask. Cover or remove LED indicator lights on electronics. No nightlights above 1 lux near the bed. |
- Morning substitutions: A 10,000-lux therapy lamp positioned 16–24 inches from the face for 20–30 minutes replaces outdoor morning light on days when outdoor access is impossible. Consistency of timing matters — use it at the same time each morning.
- Evening bulb swaps: Replace cool white LEDs in bedroom and living room fixtures with warm white (2700 K or lower) bulbs. This single change meaningfully reduces melatonin suppression from evening lighting without requiring behavioral discipline each night.
- Sleep environment: Blackout curtains are the most reliable intervention for maintaining bedroom darkness below 3 lux. A well-fitted sleep mask is a lower-cost alternative for renters or travelers. Cover or remove LED indicator lights on chargers, routers, and televisions.
- Screen management: Dim screen brightness to minimum in the 2 hours before sleep. Night mode provides additional benefit at that brightness level but is not a substitute for dimming.
When Light Management Alone May Not Be Enough
For most generally healthy adults, consistent application of the morning light protocol and evening light reduction will produce measurable improvements in sleep timing and quality within 1–4 weeks. The changes are gradual — the circadian clock shifts by roughly 30–60 minutes per week with consistent behavioral input — and they compound over time.
However, some people find that sleep timing remains persistently late or disrupted despite genuine effort with light management. If you consistently cannot fall asleep before 2–3 a.m. regardless of light habits, or if your sleep timing shifts dramatically on weekends versus weekdays, this may reflect a clinical circadian condition rather than a behavioral pattern.
Delayed sleep-phase disorder (DSPD) is the most common of these conditions in adults under 40. Shift work disorder involves circadian misalignment driven by schedule demands rather than intrinsic clock dysfunction. Both require evaluation and management beyond behavioral light protocols. For a detailed account of shift work disorder — including its diagnostic criteria and treatment options — see the article on shift work disorder: symptoms, causes, and treatment.
Supports these guides
Spot an error or have clinical feedback?
Because this article covers clinical, medication, or safety information, we use a moderated correction channel instead of open public comments. Let us know if something about “Circadian Rhythm and Light Exposure: How Light Affects Sleep” needs a closer look.
Send feedback on this article