For a daylight saving time sleep schedule in 2026, the calendar matters first. In the United States, daylight saving time began on Sunday, March 8, 2026, at 2:00 a.m., when clocks moved forward one hour. That date has already passed as of July 9, 2026. The practical target now is Sunday, November 1, 2026, at 2:00 a.m., when clocks move back one hour.[1]
The spring plan below is still worth keeping: it is the protocol to reuse before the next spring-forward cycle. But for current readers, the November fall-back change is the one to prepare for. The goal is not to turn a one-hour clock change into a personal project. It is to keep one predictable disruption from becoming several bad nights, a foggy commute, or a harder Monday than necessary.

The 2026 DST Dates and What to Do With Them
| Transition | 2026 date | Clock change | Status on July 9, 2026 | Main sleep problem |
|---|---|---|---|---|
| Spring forward | Sunday, March 8, 2026, at 2:00 a.m. | Clocks moved ahead 1 hour | Already passed | Lost sleep and a forced earlier wake time |
| Fall back | Sunday, November 1, 2026, at 2:00 a.m. | Clocks move back 1 hour | Upcoming | A later-feeling body clock, earlier-feeling evenings, and disrupted timing despite the apparent extra hour |
The spring change is harsher for most sleep schedules because the clock removes an hour. One commonly cited estimate is that the average person gets about 40 minutes less sleep on the Monday after springing forward; the figure is useful as a warning sign, not a universal prediction for every sleeper.[2]
Fall back looks easier because the clock appears to give an hour back. That is only partly true. Many people do not actually sleep the extra hour, and some feel off for days because their internal clock, light exposure, meals, school runs, work start times, and social obligations do not all move together.[5]
Your Fall-Back Plan for November 1, 2026
For November 1, treat the change as a timing adjustment, not a sleep bonus. If your schedule is flexible, you can shift gradually. If your wake time is fixed by work, caregiving, school, or transit, protect the wake time first and adjust light and bedtime around it.
| When | Bedtime | Wake time | Light cue | Main instruction |
|---|---|---|---|---|
| Wednesday, Oct. 28 | Move 15–20 minutes later if your schedule allows | Move 15–20 minutes later only if you can | Get outdoor light soon after waking | Begin nudging the body clock without sleeping in wildly |
| Thursday, Oct. 29 | Move another 15–20 minutes later | Keep the new wake time or stay consistent if fixed | Use morning light within 30 minutes of waking | Do not compensate with a late nap |
| Friday, Oct. 30 | Move another 15–20 minutes later | Keep the shift modest | Keep evenings dimmer than mornings | Avoid turning the weekend into a large schedule swing |
| Saturday, Oct. 31 | Aim close to the post-change bedtime by the clock | Set alarms for the new clock time | Prepare for bright morning light on Sunday | Do not stay up an extra hour just because the clock changes |
| Sunday, Nov. 1 | Use the new clock time | Wake at the planned new clock time | Get sunlight or bright outdoor light within 30 minutes | Anchor the new schedule immediately |
| Monday, Nov. 2 | Keep bedtime steady | Keep wake time steady | Repeat morning light exposure | Give driving, mood, and demanding work extra margin |
The fall-back mistake is spending the extra hour at night and expecting the body to behave as if it was used for sleep. A person who normally goes to bed at 11:00 p.m. may see 10:00 p.m. on the clock after the transition and not feel sleepy; a morning lark may wake too early by the new clock and fail to return to sleep. Short sleepers, especially those already averaging under 7.5 hours, can feel the mismatch more than the calendar implies.[5]
If you cannot move bedtime later before fall back, keep the plan simple: hold your wake time steady, get outside soon after waking, keep caffeine out of the late day, and avoid long naps on Sunday. For a deeper routine reset beyond DST week, use a basic evidence-based bedtime routine rather than adding a new set of rules in the middle of the transition.
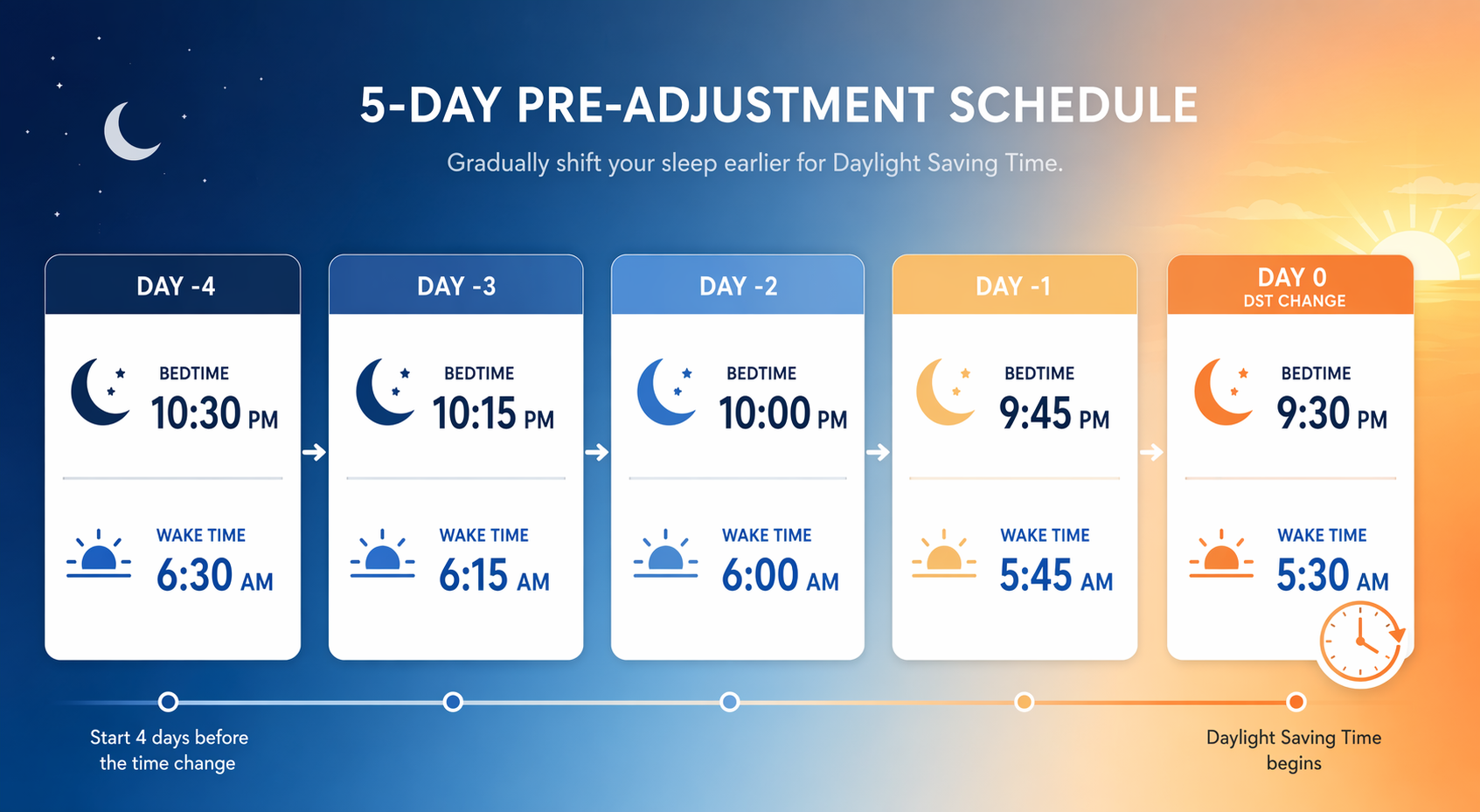
The Spring-Forward Plan to Reuse Before March 2027
March 8, 2026, is now reference material, but the spring-forward protocol is the one most people need to take seriously next year. The direction is different from fall back: you are asking the body to fall asleep earlier and wake earlier. That is harder than delaying sleep for many adults, and it is especially hard when the prior week has already produced sleep debt.
| When | Bedtime | Wake time | Morning light | Why it matters |
|---|---|---|---|---|
| Wednesday before spring forward | 15–20 minutes earlier | 15–20 minutes earlier | Outdoor light within 30 minutes of waking | Starts the advance before the clock forces it |
| Thursday | Another 15–20 minutes earlier | Another 15–20 minutes earlier | Repeat bright morning light | Uses a small shift the circadian system can handle |
| Friday | Another 15–20 minutes earlier | Another 15–20 minutes earlier if possible | Do not delay light until late morning | Reduces the size of the Sunday jump |
| Saturday | Keep the earlier bedtime even if it feels unnecessary | Avoid sleeping in late | Get daytime light; dim the evening | Prevents Saturday from undoing the adjustment |
| Sunday after the change | Use the new clock time | Wake by the new clock time | Get light soon after waking | Locks in the new morning signal |
| Monday | Keep bedtime conservative | Do not chase lost sleep with a very late wake time | Prioritize morning light again | The first workday is when the mismatch usually becomes visible |
AASM and clinical sleep experts commonly recommend shifting bedtime and wake time by about 15–20 minutes for several nights before the transition, rather than trying to absorb the full hour at once.[1][3][4] Morning sunlight within 30 minutes of waking is the strongest practical cue in this plan because light early in the day helps advance the internal clock; caffeine may make a person feel more alert, but it does not reset the clock in the same way.[3][4]
The preceding week matters. If you enter spring forward already short on sleep, the missing hour lands on top of an existing deficit. That is where “sleep banking” is useful in a modest, non-heroic sense: go to bed a little earlier for several nights, keep alcohol and late caffeine from cutting into sleep quality, and avoid treating Friday and Saturday as recovery nights that can be spent first and repaired later. For the recovery mechanics behind that idea, see sleep debt and recovery science.
Why the 15–20 Minute Shift Works
The body clock does not move like a phone clock. A device accepts the new time instantly; a person has to adjust sleep pressure, melatonin timing, light exposure, meals, temperature, and social demands. A 15–20 minute shift respects that slower system.
Morning light is the main lever because it tells the brain that the biological day has started. Used consistently, it helps pull sleepiness and alertness earlier after spring forward. After fall back, it helps stabilize the new schedule so the body does not drift into a half-shifted pattern: awake too early, sleepy too early, then pushed later again by evening screens and obligations.
Evening light does the opposite for many people. Bright light late in the evening can make it harder to fall asleep earlier before spring forward and can encourage schedule drift after fall back. This does not require a blackout-level ritual. It usually means lowering bright overhead light, keeping screens from becoming the brightest object in the room, and avoiding a late-night “one more thing” session during the transition window.
If you want the broader framework for why light timing, wake time, meals, and activity cues matter together, the next useful read is circadian hygiene. DST adjustment is a small example of that larger idea: the routine is not just about bedtime comfort; it is about giving the body repeated time cues in the same direction.
The First 48 Hours Deserve Extra Margin
The first two days after the clock change are when small mismatches are most likely to show up in ordinary life: a driver is awake but slower, a teen is technically on time but biologically delayed, a parent is managing a school morning with less patience, or a night worker is trying to make a schedule that was already difficult fit a new clock.
Health-risk findings should be read proportionately. Some studies have found acute cardiovascular and neurologic risk increases around DST transitions, including reports of a higher heart attack rate after spring forward and a higher ischemic stroke rate in the first 48 hours after transitions.[6][1] Those findings are not a reason to panic, and the cardiovascular evidence is not perfectly uniform; a 2024 Duke analysis found no significant heart-attack spike among more than 170,000 patients. The practical conclusion is narrower: vulnerable people should avoid stacking extra strain onto the transition if they can.
- Avoid scheduling the hardest drive of the week for the Monday after spring forward when possible.
- Give medication routines, medical appointments, and caregiving handoffs a second check across the clock change.
- Keep workouts moderate if you feel unusually short on sleep or unusually wired.
- Treat mood irritability and concentration problems as useful warning signs, not personal failures.
Who Should Adjust More Carefully
Most adults can use the same basic protocol. A few groups should start earlier or protect the first 48 hours more deliberately.
- Teens: their biology already tends to run later, so spring forward can hit like an early-start problem layered onto an early-start problem.
- Night shift workers: the clock change can collide with work timing, commute timing, and daytime sleep, so light exposure needs to be planned around the actual sleep episode rather than the public morning.
- Short sleepers: people already sleeping under 7.5 hours have less buffer, especially during fall back when the expected extra sleep may not happen.[5]
- Morning larks: fall back can trigger very early waking by the new clock, followed by evening sleepiness that arrives before social or family schedules allow.[5]
- People with cardiovascular or neurologic vulnerability: the evidence does not justify alarm, but it does justify avoiding unnecessary sleep loss, long drives, or high-stress scheduling immediately after the transition.
If every DST change feels extreme rather than merely annoying—several weeks of mistimed sleep, inability to fall asleep until very late, or repeated failure to wake for required obligations—the issue may be larger than daylight saving time. In that case, read about delayed sleep phase syndrome in adults and consider discussing the pattern with a clinician.
A Simple Rule for the Week of the Change
Do the small things in the same direction. Shift sleep by 15–20 minutes instead of one full hour. Keep wake time consistent. Get outdoor light within 30 minutes of waking. Keep evenings dimmer and quieter than mornings. Do not use the fall-back hour as permission to cut sleep, and do not arrive at spring forward already depleted.
For most adults, the clock change cannot be eliminated. Its impact can be reduced by starting a few nights early, moving gradually, using morning light deliberately, and treating the first 48 hours as the period when sleep, driving, mood, and health deserve extra margin.
References
- Daylight Saving Time, AASM Sleep Education
- How to Prepare for Daylight Saving Time, Sleep Foundation
- How Daylight Saving Time Affects Our Sleep, Cleveland Clinic, February 25, 2026
- Stepping Back Is Best for Springing Forward, Vanderbilt Health, February 27, 2026
- Daylight Saving Time: Fall Back Doesn't Equal Sleep Gain, Harvard Health
- Daylight Saving Time and Myocardial Infarction, JAMA Network Open, 2024
Comments
Join the discussion with an anonymous comment.