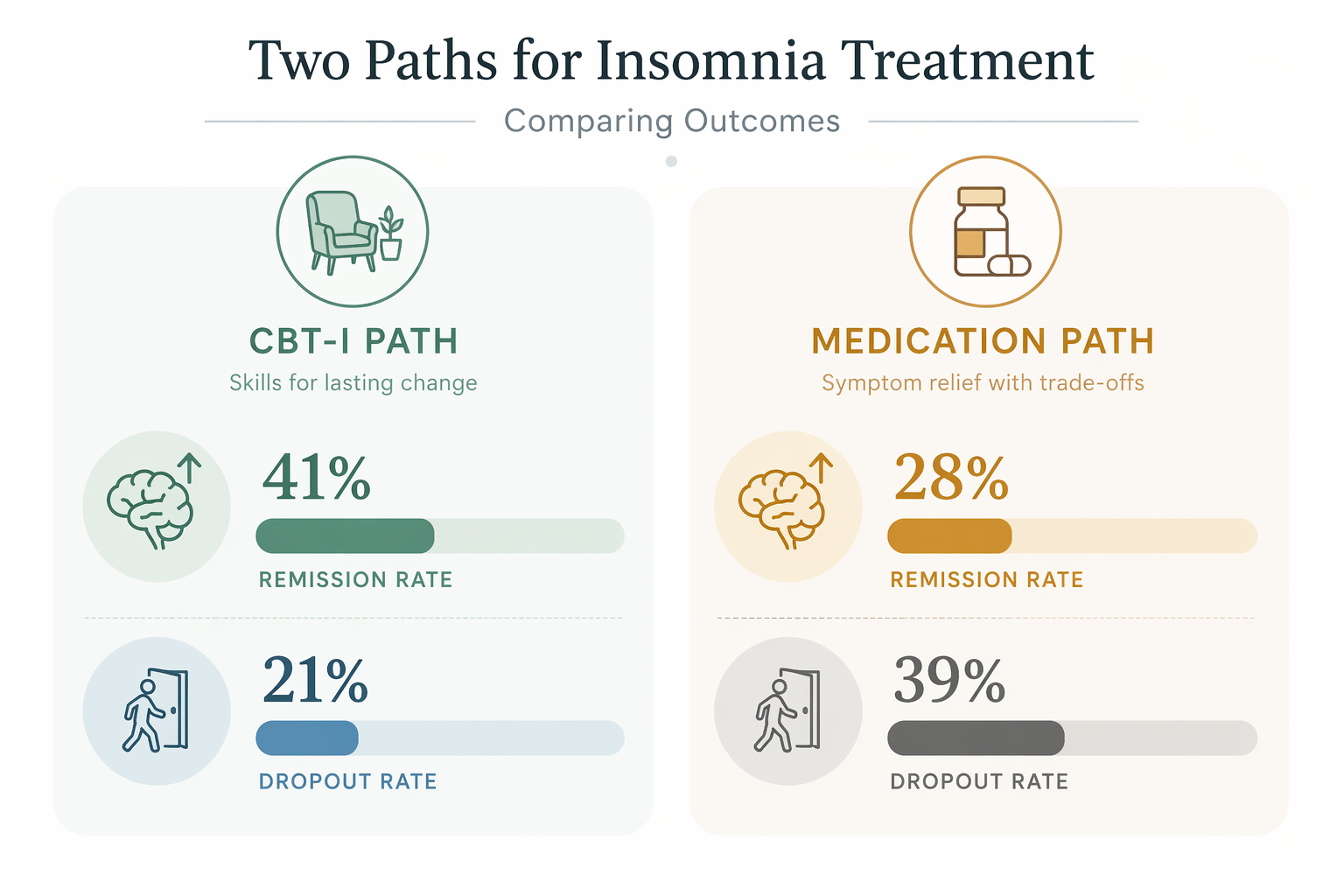
If you are choosing between online CBT-I vs sleep medication, the cleanest answer is not the most comfortable one: online CBT-I has the stronger long-term evidence, while medication may feel easier in the first several weeks. In a 2024 network meta-analysis, starting with CBT-I was associated with long-term remission in 41% of adults, compared with 28% for medication; dropout was also lower with CBT-I, 21% versus 39% with medication.[1]
That does not make sleep medication a failure or a weakness. A prescription can be the difference between functioning tomorrow and unraveling at 3 a.m. But the question here is not only “What helps me sleep this week?” It is also “What leaves me better off when the refill, dose adjustment, or anxious bedtime calculation is no longer the center of the plan?”

| Decision point | Online CBT-I | Sleep medication |
|---|---|---|
| Long-term remission | 41% in the 2024 network meta-analysis | 28% in the same analysis |
| Dropout | 21% | 39% |
| Early sleep gain | Can be slower because sleep restriction is part of treatment | May provide about 20 more minutes of sleep in the first 8 weeks |
| Durability | Built around skills that can continue after the program | Benefit can depend on continuing the medication plan |
| Side-effect burden | No medication side effects, but the early behavioral work can be hard | Side effects, next-day impairment, interactions, and dependence concerns require medical review |
The long-term result favors starting with CBT-I
The most useful part of the 2024 comparison is that it looked at what happens when people start with different treatment strategies. That matters because many insomnia decisions are made under pressure: a person is already exhausted, already missing work or snapping at family, and already afraid of another bad night. The treatment that feels merciful in that moment is not always the one with the best odds months later.
In that analysis, CBT-I produced a 41% long-term remission rate, while medication produced 28%. Combination therapy did not improve on CBT-I alone: remission was 40% with combined CBT-I plus medication versus 41% with CBT-I alone.[1] That does not mean no individual person ever benefits from a temporary combined plan. It means the broader evidence does not support the idea that adding medication automatically makes the long-term outcome stronger.
Dropout belongs in the same conversation as remission. People do not drop out of insomnia care because they are lazy. They drop out because the plan is too hard, too expensive, too inconvenient, too frightening, too sedating, or simply not helping fast enough. A 21% dropout rate for CBT-I compared with 39% for medication is not a footnote; it is part of the outcome.[1]
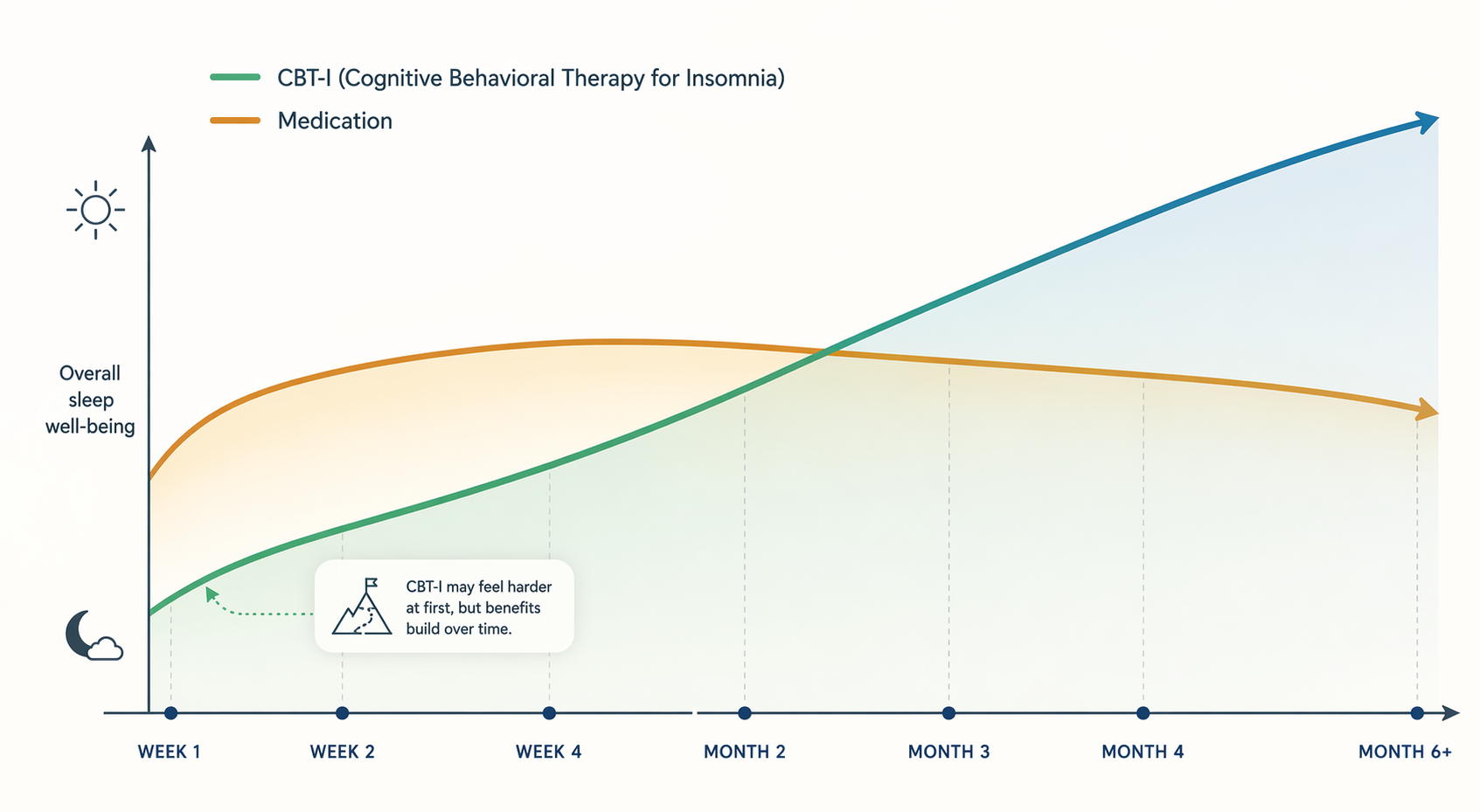
Real-world data point in the same direction, though with the usual caution that cohort studies are not randomized trials. In a JAMA Network Open study of 4,052 patients, digital CBT-I users improved on the Pittsburgh Sleep Quality Index from 13.51 to 7.15, while medication users improved from 12.85 to 8.92. The medication group improved early, then leveled off after months 1 to 2 and worsened after months 4 to 5; the digital CBT-I group continued improving over time.[2]
A 2025 systematic review of fully automated digital CBT-I found 29 randomized controlled trials with 9,475 participants. The pooled effect on insomnia severity was SMD = −0.71, and effects were sustained beyond 6 months at SMD = −0.76 with I² = 0%.[3] Those numbers are not a promise that every app works, and they are not a promise that every person will remit. They do show that the digital version of CBT-I is not merely “sleep hygiene with notifications.” When properly built and studied, it can produce durable clinical change.
Why medication can look better in the first weeks
The short-term advantage of medication deserves to be stated plainly. In the first 8 weeks, medication may give about 20 more minutes of sleep than CBT-I, largely because CBT-I often begins with sleep restriction.[1] If you are already running on fumes, 20 minutes is not trivial. It can change a morning commute, a shift at work, a school drop-off, or the ability to hold a conversation without feeling brittle.
Sleep restriction is badly named for how it feels. It does not mean depriving someone of sleep as punishment. It means temporarily limiting time in bed to better match the amount of sleep the person is actually getting, then gradually expanding the sleep window as sleep becomes more consolidated. On paper, that is a behavioral technique. In real life, it can feel like being asked to give up the only safe place you have been clinging to.
That early phase is where many people need the most support. A person who has been lying in bed for 9 hours and sleeping 5 may be asked to spend much less time in bed at first. Even when the plan is clinically appropriate, the first week can feel alarming: more structure, less room for desperate catch-up sleep, and a sharper awareness of the clock. Calling this “not a side effect” may be technically correct, but it can miss the burden the patient actually carries.
Medication avoids that specific discomfort. It does not ask you to compress your sleep window, track stimulus control, or sit with the fear that tonight may be even shorter. That is why it can feel like the more humane option at the beginning. The tradeoff is that early sleep extension is not the same as remission, and relief that depends on continuing a drug plan has to be judged differently from relief that comes from learning how to rebuild sleep drive and reduce conditioned arousal.
Side effects, adherence, and what “no side effects” does not mean
Online CBT-I does not carry medication side effects. There is no next-day drug hangover, no pharmacologic interaction with alcohol or other prescriptions, and no dose escalation question built into the treatment itself. But that should not be stretched into “CBT-I is easy.” The burden is behavioral: staying out of bed when you are exhausted, getting up at a consistent time, reducing naps, and continuing the plan when the first few nights make you doubt the whole idea.
Medication has a different burden. The prescribing clinician has to consider age, fall risk, other sedating medicines, pregnancy status, substance use history, breathing disorders, work safety, driving, and the specific drug’s risk profile. Some people tolerate a sleep medication well for a short period. Others feel dulled the next day, become worried about sleeping without it, or find that the original dose no longer feels as reliable. Those are not moral issues. They are treatment issues.
This is also why dropout is more than an administrative number. If a person stops medication because of side effects, or stops CBT-I because sleep restriction feels unbearable, the treatment did not simply “work in theory.” It failed to fit the patient’s life at that moment. The better first choice is the one with evidence and a realistic path through the hard part.
Not every online CBT-I program deserves the same trust
The evidence for digital CBT-I should not be handed over to every app that uses the language of CBT-I. A structured digital program is different from a sleep tips app, a meditation library, or a habit tracker with a bedtime reminder. The programs with stronger published support include Somryst, Sleepio, and CBT-I Coach, while many apps listed or marketed as insomnia tools do not have the same randomized trial record.
A credible online CBT-I program should do more than give generic advice. It should assess insomnia symptoms, guide sleep scheduling, address time-in-bed patterns, teach stimulus control, work with unhelpful sleep beliefs, and adjust recommendations based on sleep data. If the program never changes course when your sleep pattern changes, it may be education rather than treatment.
- Look for published clinical studies on the specific program, not just claims about CBT-I as a category.
- Check whether the program includes sleep restriction or sleep compression, not only relaxation exercises.
- Make sure there is guidance for worsening sleep, excessive sleepiness, mental health symptoms, or safety concerns.
- Prefer programs that explain when to involve a clinician rather than pretending insomnia is always self-managed.
Cost and access can change the best answer
A treatment cannot be first-line in any meaningful way if the patient cannot get it. Online CBT-I exists partly because therapist-led CBT-I is hard to access in many areas. Digital programs can reduce the travel, scheduling, and specialist shortage problems, but they introduce other barriers: cost, insurance coverage, language, digital literacy, privacy comfort, and the ability to follow a structured plan without live coaching.
Cost claims need particular caution. Some digital CBT-I programs are free or low cost; others require payment, employer access, prescription routing, or insurance coverage. Medication may be inexpensive for some people and costly for others, especially if visits, follow-ups, side effects, or longer-term use are included. Product-specific savings estimates should not be treated as universal savings for every digital CBT-I program.
Access also affects safety. Someone with severe depression, bipolar disorder, active substance use concerns, untreated sleep apnea symptoms, high fall risk, or a job where sleepiness endangers others should not have to sort this out from an app alone. In those situations, the decision is less “online program or pills?” and more “what supervised plan keeps me safe while treating the insomnia?”
Who might reasonably start with online CBT-I
Online CBT-I is the stronger first choice when the main goal is durable remission and the person can tolerate a structured early phase. That does not mean the person feels fine. It means they have enough safety, support, and flexibility to get through the first weeks without the plan becoming dangerous or impossible.
- You want the best long-term odds rather than the fastest first-week relief.
- You can accept that sleep may feel more restricted before it feels more stable.
- You prefer a treatment that leaves you with skills after the program ends.
- You have access to a credible digital CBT-I program with enough guidance to keep you engaged.
- You do not have urgent medical or psychiatric factors that require closer clinical supervision.
For this person, the early discomfort is not ignored; it is planned for. The first weeks may require choosing a start date carefully, warning a partner or family member, avoiding major life crunch periods when possible, and knowing in advance when to contact a clinician. The evidence favors CBT-I, but adherence often depends on how honestly the hard part is prepared.
Who might reasonably discuss medication first
Medication may be a reasonable first discussion when immediate functioning is the dominant problem. That might include a person who is at risk of losing a job, cannot safely care for dependents, is in an acute crisis, or has become so fearful of sleep restriction that they are unlikely to start CBT-I at all. In those cases, the medication conversation should be clinical, specific, and time-aware.
The important distinction is between using medication as a short-term bridge and treating it as the better durable solution. A bridge has a purpose: stabilize the next few nights or weeks, reduce immediate risk, and create enough room to begin a longer-term insomnia plan. It also has review points. The prescriber and patient should know what benefit they are looking for, what side effects would stop the plan, and when the strategy will be reassessed.
For some people, the safest path may be medication plus a plan to begin CBT-I once the acute pressure drops. The 2024 evidence does not show added long-term remission from combination therapy over CBT-I alone, but that is different from saying medication can never help someone enter treatment.[1] The job of a short-term medication plan is not to win the long-term evidence contest. It is to keep the person functioning while the durable treatment becomes possible.
A practical way to choose
Start with the time horizon. If you need the strongest chance of long-term remission and can get through the early sleep restriction period with a credible program, online CBT-I is the better first choice. The remission, dropout, real-world trajectory, and sustained digital CBT-I findings all point in that direction.[1][2][3]
If the next several nights are the emergency, medication may deserve a careful conversation with a clinician. That conversation should not stop at “Can I sleep?” It should include the medication choice, dose, expected duration, next-day safety, interactions, stopping plan, and whether CBT-I will be started alongside or after the acute period.
The fairest comparison is not skills good, pills bad. It is this: medication may help sooner, while online CBT-I is more likely to help insomnia remit and stay improved. The best first step depends on whether your biggest risk is tonight’s functioning, the next six months of treatment, or the lack of access to a plan you can actually complete.
References
- Comparative efficacy and acceptability of psychological, pharmacological, and combined interventions for insomnia: A systematic review and network meta-analysis, Psychiatry and Clinical Neurosciences, 2024, https://doi.org/10.1111/pcn.13730
- Comparison of Digital Cognitive Behavioral Therapy vs Medication Therapy Among Patients With Insomnia, JAMA Network Open, 2023, https://pmc.ncbi.nlm.nih.gov/articles/PMC10091171/
- Effectiveness of fully automated digital cognitive behavioral therapy for insomnia: A systematic review and meta-analysis, npj Digital Medicine, 2025, https://www.nature.com/articles/s41746-025-01514-4
Comments
Join the discussion with an anonymous comment.