The problem with most things to help sleep is that they assume the same fix should work for everyone. That is why one person swears by tea, another by a weighted blanket, and a third gets nowhere. The better question is not what helped somebody else, but which sleep bottleneck is actually keeping your body awake.

Use the quick match below first, then read the section that fits most closely. If you want a deeper comparison between trouble falling asleep and trouble staying asleep, this companion guide is a useful next stop: Trouble Falling Asleep vs. Staying Asleep: Why the Difference Matters for Treatment.
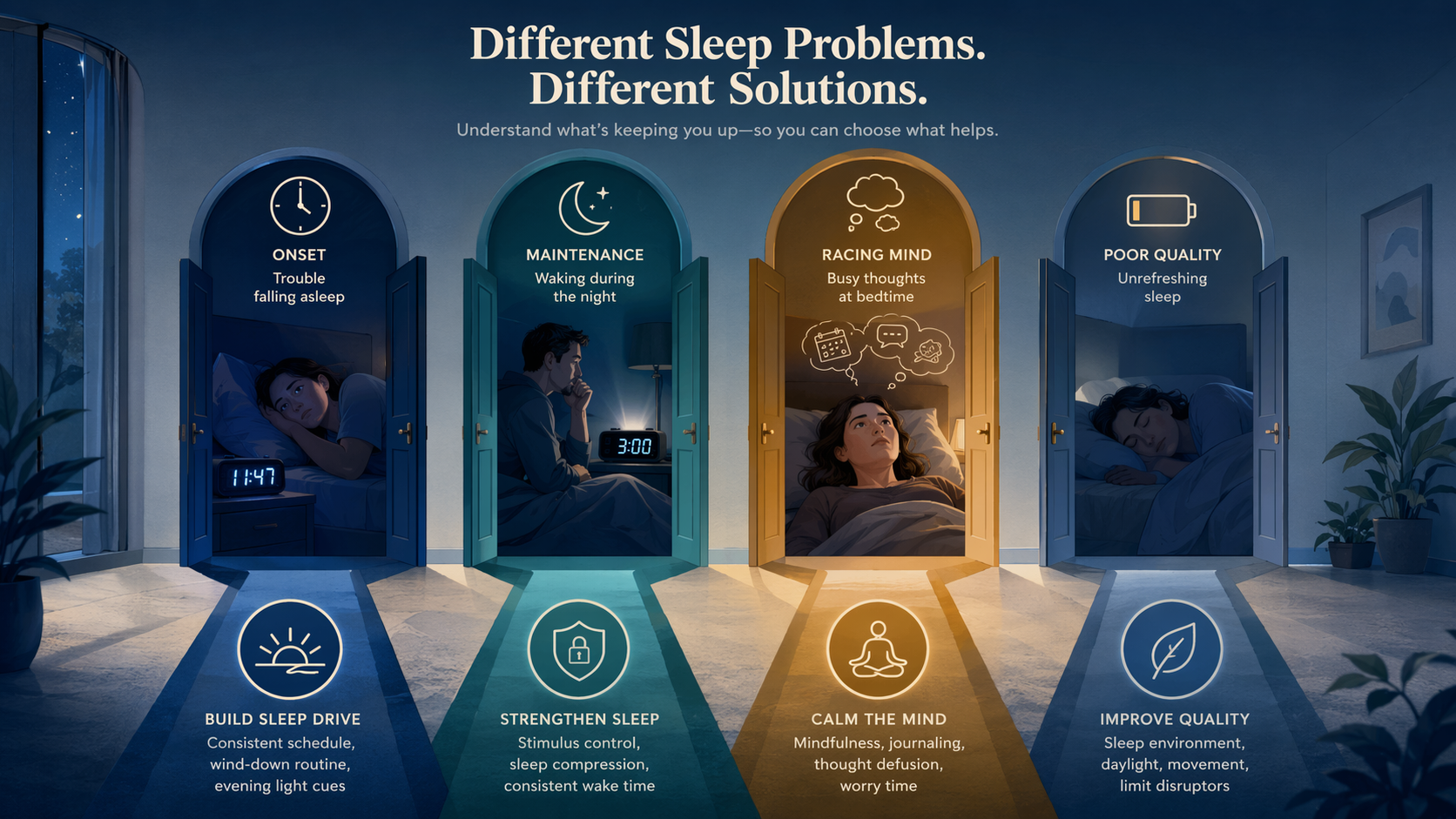
| If this is your main problem | Start with |
|---|---|
| You lie awake at bedtime | Stimulus control, then the specific to-do list tool |
| You fall asleep, then wake in the night | Caffeine timing, alcohol timing, and bedroom temperature |
| Your mind will not shut off | Worry writing, mindfulness, and a short cognitive reset |
| You sleep, but wake unrefreshed | Exercise timing, morning light, and a check for something beyond routine habits |
Can't fall asleep
When the bed has turned into a wakefulness cue, the problem is often conditioned arousal. The bedroom starts predicting frustration instead of sleep, so the body learns to stay alert the moment you lie down. That is why stimulus control is such a strong match: if you are still awake after roughly 20 to 25 minutes, get out of bed, do something quiet and dim, and return only when you feel sleepy again. Keeping the bed for sleep and sex is part of the same reset. Multicomponent CBT-I for primary insomnia is where the often-quoted 70% to 80% improvement figure belongs, not sleep hygiene alone.[1]
A useful self-check is sleep latency, or how long it takes you to drift off. Sleep Foundation notes that normal sleep latency is usually around 15 to 20 minutes; falling asleep in under 10 minutes on a regular basis can mean you are sleep deprived rather than unusually efficient, while consistently taking much longer points toward insomnia rather than a missing lavender spray.[2]
For a bedside reset, a specific five-minute to-do list can help more than generic journaling. In the Scullin study summarized by Sleep Foundation, writing down concrete unfinished tasks before bed sped sleep onset compared with writing about completed activities.[2] That fits the mechanism here: you are not trying to become more productive at night, just getting the brain to stop holding tomorrow open in working memory.
A breathing pattern such as 4-7-8 can still be useful if it helps your body downshift, but it is better treated as a relaxation tool than as a proven cure. If you have been forcing sleep harder and harder, the better read is often that the bed has become a signal to perform, which is why trying harder usually backfires. This article on the cycle is the more direct match: Why Trying Harder to Fall Asleep Backfires — and How to Break the Cycle.
Can't stay asleep
Maintenance insomnia often has a different set of suspects. Late caffeine can be enough to fragment the second half of the night even when it does not stop you from falling asleep at all. In Drake's study, caffeine consumed six hours before bed cut total sleep time by more than an hour; a 2023 review summarized by Sleep Foundation found about 45 minutes less total sleep and 7% lower sleep efficiency with late caffeine use.[3] If you wake at 3 a.m. after an afternoon coffee, that is not a mystery problem.
Alcohol can do the same kind of damage in a different way: you may feel sleepy faster, then wake more often later in the night. If the second half of the night keeps getting choppy after evening drinks, that is a useful clue, not a discipline failure.
Temperature matters here too. Harvard Health puts the best sleep range around 65 to 68°F, which matches the body’s normal nighttime cooling pattern.[4] If your room is warmer than that, or if your bedding traps heat, the fix is usually practical before it is philosophical: cool the room, lighten the covers, and stop treating a hot room as a minor detail.
This is also the section where generic bedtime rules tend to misfire. If the real issue is that caffeine, alcohol, or heat keeps cutting sleep into pieces, a longer wind-down routine is not the bottleneck. Move the stimulant earlier, change the evening drink pattern, or change the room first.
Racing thoughts at bedtime
This version of insomnia is less about the bed itself and more about cognitive hyperarousal. The brain keeps rehearsing tomorrow, re-litigating today, or scanning for unfinished business when it should be letting go. A short written dump works better than an open-ended journal prompt for many people because it gives the mind a place to put loose ends. The Scullin to-do list finding matters here too, because the mind often settles when it no longer has to keep tasks active in memory.[2]
Mindfulness meditation and cognitive restructuring can help when the loop is worry, not just alertness. The key is to keep them simple enough that they do not become another performance task before bed. If the mind is demanding certainty, answer with something concrete: write the worry down, decide whether there is an action for tomorrow, and stop there.
One cross-sectional study in a Tabuk City sample of 384 adults found that poor sleep hygiene was associated with more depression and more excessive daytime sleepiness, but that is an association, not proof of cause.[5] The useful point is narrower: when sleep and mood are both fraying, bedtime habits may be part of the picture, but they are not always the whole story.
Wake up unrefreshed
If you are technically sleeping enough but still wake flat, the problem may be less about falling asleep and more about sleep quality and circadian anchoring. Regular exercise and morning light exposure are the simplest levers to try here. Morning light helps set the clock for the day, and movement tends to help sleep most when it is not pushed too close to bedtime for your own body.
Do not overread this pattern as a routine problem if you are already doing the obvious things. Waking unrefreshed despite enough time in bed can mean the issue is not just habits, which is why this pattern deserves a lower threshold for evaluation than a simple "sleep hygiene" fix.
If you want the baseline routine before you go any further, start here: Sleep Hygiene Fundamentals and an Evidence-Based Bedtime Routine. If you are already looking beyond routines and want to compare supplement options by mechanism, that is a separate guide: How to Choose a Sleep Supplement Based on Your Specific Sleep Problem.
When to escalate
Some symptoms should not be treated as a self-optimization project. Loud snoring with gasping or choking, excessive daytime sleepiness even when you are spending 7 to 9 hours in bed, and symptoms that keep going for more than three months despite consistent changes are all reasons to stop tinkering and get evaluated.
The point is not that sleep problems are rare. Harvard Health summarizes CDC data showing that 14.5% of U.S. adults have trouble falling asleep and 17.8% have trouble staying asleep.[4] Johns Hopkins also notes that more than 60 million Americans have poor sleep quality.[6] Common is not the same as harmless.
If you have already covered the matched intervention and the problem still looks the same, that is where the limits of sleep hygiene start to matter more than the next tip. This is the point to read: The Hidden Limits of Sleep Hygiene: When Healthy Habits Aren't Enough and What to Try Instead.
The useful thing to help sleep is not the most popular tip in the aisle. It is the intervention that fits the mechanism keeping this particular reader awake.
References
- Cognitive Behavioral Therapy for Insomnia (CBT-I) — Sleep Foundation — sleepfoundation.org
- How to Fall Asleep Fast — Sleep Foundation — sleepfoundation.org
- 15 Proven Tips to Sleep Better — Healthline — healthline.com
- 8 Secrets to a Good Night's Sleep — Harvard Health Publishing — health.harvard.edu
- Cross-sectional study on sleep hygiene, depression, and excessive daytime sleepiness — PMC — pmc.ncbi.nlm.nih.gov
- Natural Sleep Aids — Johns Hopkins Medicine — hopkinsmedicine.org
Comments
Join the discussion with an anonymous comment.