The connection between sleep duration and stroke risk is not a simple more-is-better story. The curve is U-shaped: risk is lowest around 7 to 8 hours and rises when sleep slips under 6 hours or climbs beyond 9 hours [1]. The tails do not mean the same thing. Short sleep looks like a modifiable exposure; long sleep more often looks like a clue.

Why the short-sleep side gets the most attention
The 2025 GeroScience meta-analysis is the clearest quantitative anchor here. It pooled 34 cohorts for stroke incidence and 9 for mortality, and found that short sleep under 6 hours was associated with higher stroke incidence (HR 1.29, 95% CI 1.19-1.40) and higher stroke mortality (HR 1.12), while long sleep over 8 to 9 hours showed still larger associations for incidence (HR 1.46, 95% CI 1.33-1.60) and mortality (HR 1.45) [1]. The same analysis reported substantial heterogeneity (I2 = 74% to 75%) and publication bias, so the pooled effects may be inflated rather than exact.
That warning matters, but it does not erase the pattern. Most sleep-duration studies still rely on self-report, which tends to overestimate sleep, especially in people who are actually short sleepers [1]. Even so, the short-sleep signal keeps showing up: the AASM REGARDS analysis found that under 6 hours topped stroke risk in a low-risk population [3], and an EPIC-Potsdam result summarized in a NIH review linked under 6 hours to about a twofold increase in stroke risk [4].
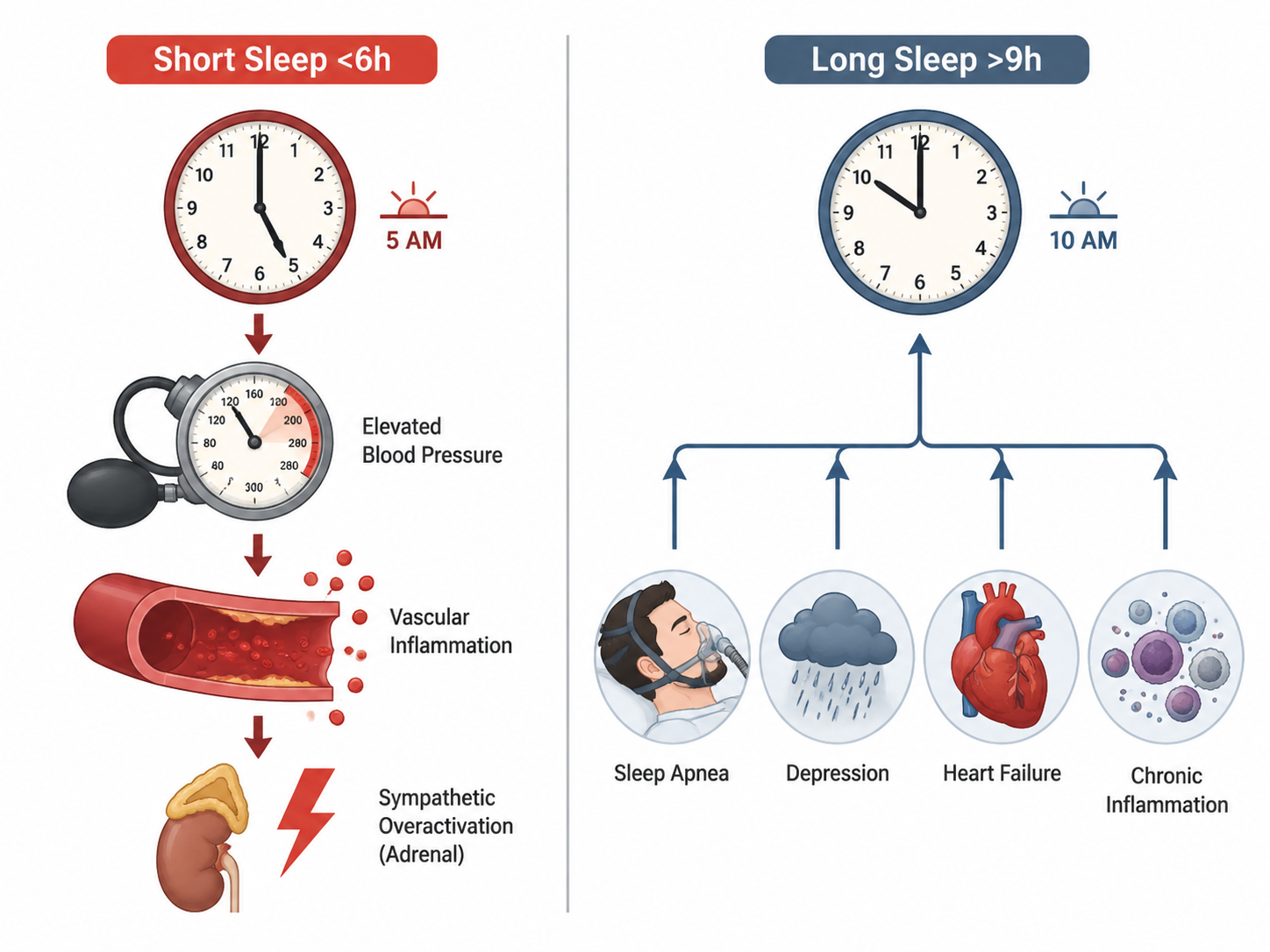
The biology is also more straightforward at this end of the curve. Too little sleep raises sympathetic nervous system activity, pushes nocturnal blood pressure upward, and is associated with systemic inflammation and insulin resistance, all of which are relevant to cerebrovascular injury [4]. That makes short sleep a chain of effects a person can actually try to interrupt: less stress signaling, better blood pressure control, less inflammatory load, and more stable metabolic regulation.
Why long sleep is a different signal
Long sleep is not just the mirror image of short sleep. In a 2019 Stroke analysis of about 32,000 adults, sleeping at least 9 hours was associated with 23% higher stroke risk compared with less than 8 hours; naps of 90 minutes or more carried 25% higher risk, and the combination of long sleep plus long naps reached 85% higher risk [2].
That association should not be read as proof that extending sleep is harmful in the same way that short sleep is harmful. Long sleep is often tangled up with reverse causation, fragmented sleep architecture, or illness severity rather than functioning as a simple exposure. In other words, the extra time in bed may be the symptom, not the cause.
That is why the long-sleep tail belongs with underlying conditions such as sleep apnea, depression, heart failure, and chronic inflammation [4]. A person sleeping more than 9 hours may need evaluation, not a goal to sleep even longer.
What the curve means in practice
No randomized trial has shown that changing sleep duration lowers stroke incidence, so the evidence stays observational. That limitation does not flatten the practical advice; it sharpens it. If you are consistently under 6 hours, treat it as a modifiable risk factor and work on the reason you are shorting sleep. If you are regularly over 9 hours, do not assume more sleep is the answer. Ask what is driving it, and whether a clinician should look for sleep apnea, depression, heart failure, or another illness [4].
References
- Inadequate sleep increases stroke risk: evidence from a comprehensive meta-analysis of incidence and mortality — GeroScience, 2025, link
- Sleep and Stroke — Stroke (AHA Journals), link
- Under 6 Hours of Sleep Tops Risks for Stroke in a Low-Risk Population — American Academy of Sleep Medicine, link
- Sleep Disturbances as a Risk Factor for Stroke — PMC/NIH, link
Comments
Join the discussion with an anonymous comment.