Mechanism explainer
How Sleep Position Affects Sleep Quality and Health: The Mechanisms Behind the Mattress
Sleep position is a nightly physiological intervention — not just a comfort preference — that operates through four distinct biological mechanisms affecting airway patency, spinal load, gastroesophageal anatomy, and glymphatic transport. This mechanistic guide explains the science behind position-dependent health effects and maps evidence-grounded recommendations to specific conditions including OSA, GERD, back pain, and pregnancy.
You Change Position 11–13 Times a Night — Does It Matter Where You Land?
Most adults think of sleep position as a comfort preference — something settled before the lights go out and maintained until morning. The biology is more complicated. Wearable sensor research shows that people shift position between 1.86 and 2.40 times per hour during sleep — roughly 11 to 13 transitions across a full night. No one holds a single position from lights-out to alarm. The mechanistic question, then, is not which position to lock into, but which positions produce better physiological outcomes when you land in them.
Position is a modifiable variable that operates through at least four distinct biological pathways. Each pathway has its own evidence base, its own set of conditions it affects, and its own clinical weight. Understanding those mechanisms — rather than following a generic "best position" recommendation — is what allows for evidence-grounded, condition-specific adjustment.
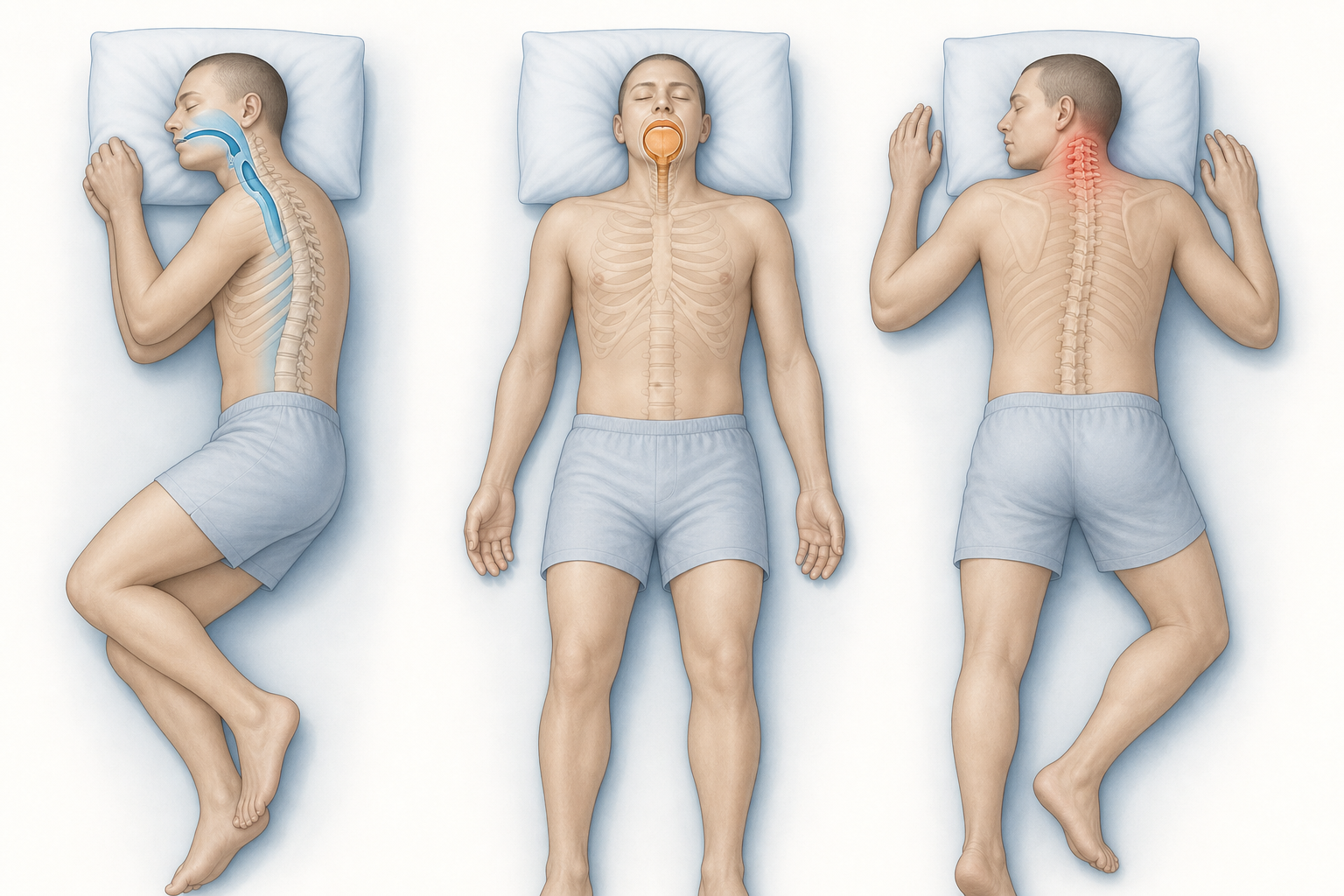
Mechanism 1 — Airway Patency: How Gravity Determines Whether You Breathe Freely
When you lie on your back, gravity acts directly on the soft tissue structures at the back of the throat — the tongue, soft palate, uvula, and surrounding musculature. These structures shift posteriorly, narrowing the pharyngeal airway. In people with obstructive sleep apnea (OSA), this narrowing can become a complete obstruction, producing the apnea events that fragment sleep and reduce blood oxygen saturation.
"Most people with sleep apnea have much, much worse sleep apnea when they sleep on their back versus on their sides." — Dr. Susan Redline, Brigham and Women's Hospital, Harvard Medical School
The clinical term for this is positional obstructive sleep apnea (POSA) — OSA whose severity is significantly worse in the supine position. Population-based cohort data suggest POSA affects approximately 50% of people with mild OSA, around 20% with moderate OSA, and roughly 7% with severe OSA. Across the broader OSA population, positional sensitivity is the rule rather than the exception.
Lateral positioning — either left or right side — reduces the gravitational load on pharyngeal soft tissue and keeps the airway more patent. For OSA management, both sides are therapeutically equivalent in terms of airway mechanics. Elevation of the head and torso by 30–45 degrees provides an additive benefit by further reducing the posterior displacement of soft tissue.
Prone (stomach) sleeping does reduce airway collapse to some degree by preventing the tongue from falling backward. However, the cervical and lumbar costs of prone positioning — covered in the next section — make it a poor clinical trade-off for the vast majority of adults. It is not recommended as a primary positional strategy for OSA.
Mechanism 2 — Spinal Load and Musculoskeletal Health: Why Prone Sleeping Is the Worst-Case Scenario
Every sleep position creates a different intradiscal pressure profile and a different load on the cervical and lumbar spine. The differences are not trivial — spending six to nine hours in a position that misaligns spinal structures accumulates mechanical stress that can contribute to waking pain and long-term musculoskeletal dysfunction.
Prone sleeping is consistently identified across clinical sources — including Harvard Health, Johns Hopkins, and Mayo Clinic — as the position most associated with neck and low back pain risk. The reason is structural: when lying face-down, the head must rotate to one side for breathing, placing the cervical spine in sustained rotation and hyperextension for hours at a time. Simultaneously, the lumbar spine is compressed without the neutral curvature that upright or supine positions maintain. There is no pillow configuration that fully corrects cervical rotation in the prone position.
Supine sleeping, when properly supported, maintains the closest approximation to the spine's neutral alignment. A low-loft pillow that keeps the cervical spine level with the thoracic spine — rather than pushing the head forward — is the critical variable. Without appropriate pillow support, even supine sleeping can create cervical flexion stress.
Lateral sleeping distributes spinal load differently across the two sides of the body. The key support variable is the space between the knees: without an inter-knee pillow, the upper leg drops toward the mattress, creating a rotational torque through the lumbar spine and hip. An inter-knee pillow maintains pelvic alignment and reduces that rotational load, making lateral sleeping well-tolerated for most people with chronic low back or hip pain.
- Prone: worst-case for cervical and lumbar alignment; sustained cervical rotation unavoidable; not recommended for adults with neck or back pain.
- Supine: neutral spinal alignment when supported by a low-loft pillow; compromised by excessive pillow height or no lumbar support on soft mattresses.
- Lateral: good spinal alignment when an inter-knee pillow maintains pelvic level; pillow loft should be higher than for supine to fill the shoulder-to-head gap.
- Mattress firmness and pillow loft are independently adjustable variables that modify position-specific spinal outcomes — the same position can be well- or poorly-supported depending on these factors.
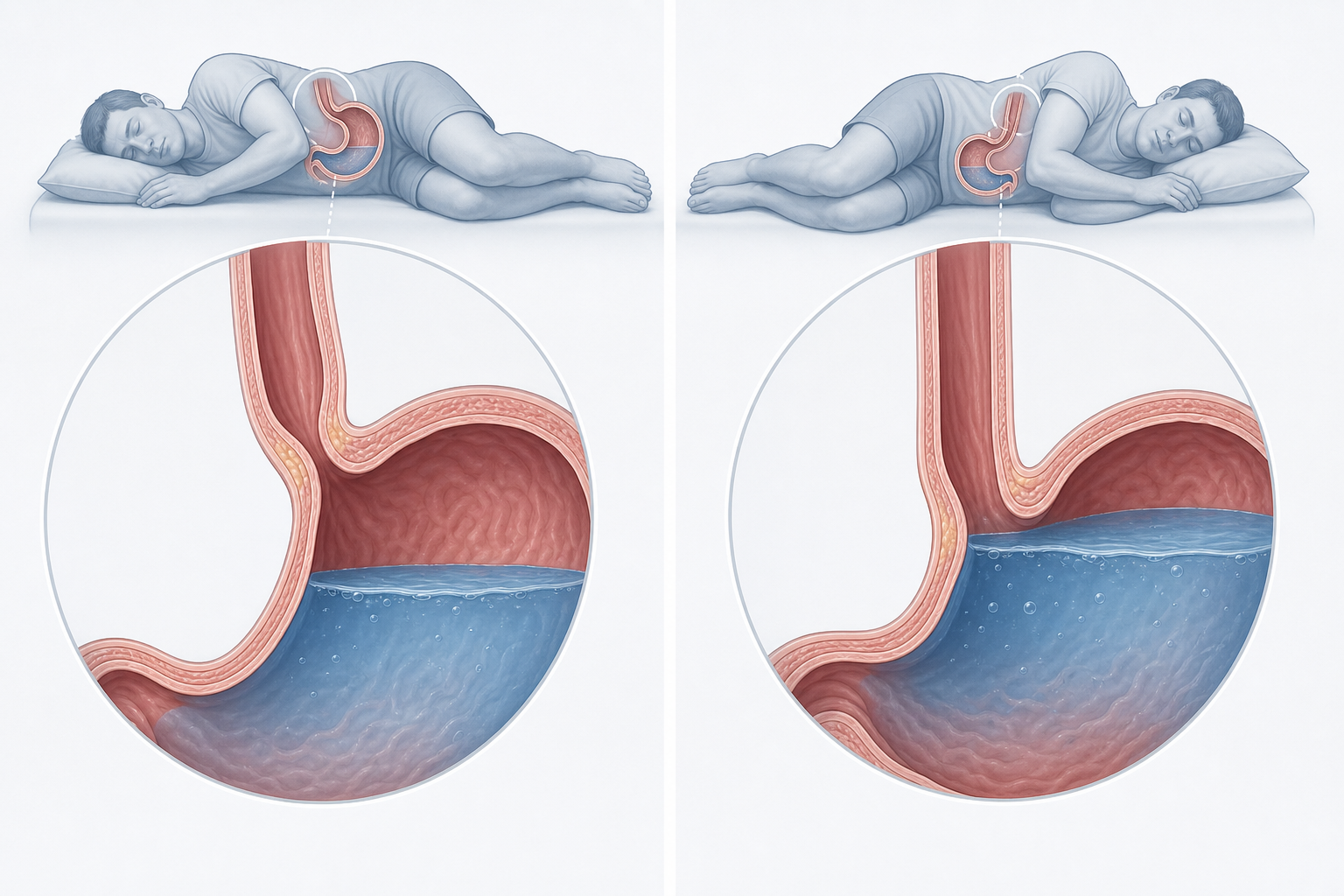
Mechanism 3 — Gastroesophageal Anatomy: Why Left Lateral Specifically Reduces Acid Exposure
The effect of sleep position on gastroesophageal reflux disease (GERD) is not simply a matter of lying flat versus elevated — the side you lie on produces dramatically different outcomes, for a clear anatomical reason.
In the left lateral decubitus (LLD) position, the geometry of the stomach and esophagus places the lower esophageal sphincter (LES) above the level of gastric fluid. Acid must travel upward against gravity to reach the esophagus. In the right lateral decubitus (RLD) position, the anatomy is reversed: the LES sits below the gastric fluid level, and acid pools directly against the sphincter, making reflux mechanically easier.
A 2023 systematic review and meta-analysis published in the World Journal of Clinical Cases quantified these differences. The analysis found that LLD reduced acid exposure time (AET) by approximately 2% compared to RLD and by approximately 2.71% compared to supine. Acid clearance time — how long the esophagus takes to neutralize each reflux episode — was reduced by roughly 82 seconds per episode in LLD versus RLD. Critically, the analysis found no statistically significant difference in AET or acid clearance time between right lateral and supine positions. Right lateral sleeping offers no meaningful GERD benefit over lying on your back.
The 2022 American College of Gastroenterology (ACG) clinical guidelines explicitly endorse left lateral decubitus sleep positioning as an evidence-supported lifestyle modification for GERD management. Head-of-bed elevation (raising the head end of the mattress by 6–8 inches, or using a wedge pillow) provides an additive benefit by further reducing the gravitational gradient for acid reflux.
Mechanism 4 — Glymphatic Transport: What the Rodent Data Shows and What It Doesn't
The glymphatic system is a brain-wide fluid transport network that clears metabolic waste — including amyloid-beta and tau proteins implicated in neurodegenerative disease — primarily during sleep. It operates through cerebrospinal fluid (CSF) exchange with interstitial fluid (ISF) along perivascular channels, and is most active during NREM slow-wave sleep (N3), when neural activity is low and interstitial space expands.
A 2015 study published in the Journal of Neuroscience used dynamic-contrast-enhanced MRI and radiotracer methods in anesthetized rodents to compare glymphatic transport efficiency across sleep positions. The findings showed that lateral positioning produced more efficient CSF-ISF exchange than supine, and that prone position showed the worst glymphatic transport — with the highest tracer retention and increased CSF efflux along cervical vasculature rather than into brain tissue. The authors explicitly noted that their findings awaited testing in humans.
A 2025 review in Frontiers in Neurology confirmed the broader picture: glymphatic activity is primarily driven by NREM N3 sleep quality and low arousal state, with sleep position as a secondary influencing factor. The review also noted that OSA — which fragments N3 sleep — is associated with reduced glymphatic function, connecting airway mechanics and brain waste clearance through a shared pathway.
"I don't think there's anything ready for prime time." — Dr. Devin Brown, University of Michigan, on the clinical applicability of glymphatic-position research in humans
Sleep Quality Metrics: What Sensor Data Shows About Position, Slow-Wave Sleep, and Turning Frequency
Beyond the mechanistic pathways, a 15-night wearable sensor study published in Sensors in 2022 examined how preferred sleep position relates to objective and subjective sleep quality measures in healthy adults. The study is small — 13 subjects with a mean age of 24, none with sleep disorders — so its findings are directional rather than definitive, and should not be generalized to clinical populations.
Within that sample, subjects with a right-lateral sleeping preference showed the longest slow-wave sleep duration (274 minutes versus 245 minutes for supine-preferring subjects and 231 minutes for left-lateral-preferring subjects) and the fewest nocturnal awakenings (0.23 per night versus 0.80 for supine). Left lateral preference fell between the two in both metrics. The reasons for the right-lateral advantage in this specific sample are not fully explained by the study design, and the sample size is too small to draw firm conclusions.
The study also found that turning frequency — how often subjects changed position during the night — was inversely correlated with subjective sleep quality (Karolinska Sleepiness Scale correlation r = −0.65; Morning Sleepiness scale r = −0.55). The important interpretive point is the direction of causation: poor sleep drives more turning, not the reverse. Position changes are a symptom of disrupted sleep, not its cause. Attempting to restrict position changes would not improve sleep quality and could worsen comfort.
"I've interpreted thousands of sleep studies, and rarely do you see someone sleeping in the same position all night long. We all have 90-minute sleep cycles, and when we change sleep stages, we often punctuate those shifts with a position change." — Dr. John Winkelman, Harvard Medical School Division of Sleep Medicine
Condition-Specific Position Guidance: A Reference Table
The table below maps specific health conditions to evidence-grounded positional recommendations. Evidence strength reflects the quality of the underlying research, not the certainty of individual outcomes. Caveats are included where the recommendation is condition-asymmetric or where clinical oversight is essential.
| Condition | Recommended Position(s) | Evidence Strength | Key Caveats |
|---|---|---|---|
| Obstructive sleep apnea (OSA) | Lateral (either side); head/torso elevation 30–45° | Strong — supported by clinical guidelines and cohort data | Both sides reduce airway collapse; positional therapy is an adjunct to, not a replacement for, CPAP in moderate-to-severe OSA |
| GERD / acid reflux | Left lateral specifically; add head-of-bed elevation | Strong — 2023 meta-analysis; 2022 ACG guideline endorsement | Right lateral shows no benefit over supine; do not substitute right-lateral for left-lateral in GERD management |
| Chronic low back pain | Lateral with inter-knee pillow; or supine with lumbar support | Moderate — clinical consensus from multiple sleep medicine sources | Pillow between knees is essential for lateral sleeping to prevent pelvic rotation |
| Neck pain | Supine with low-loft pillow maintaining neutral cervical curve | Moderate — clinical consensus | Pillow loft is the critical variable; excessive loft creates cervical flexion stress even in supine |
| Hip pain | Lateral on unaffected side with inter-knee pillow | Moderate — clinical consensus | Lying on the affected hip increases joint compression; inter-knee pillow reduces lumbar torque |
| Pregnancy (second and third trimester) | Left lateral | Strong — ACOG guidance; vena cava anatomy | Supine contraindicated: uterine weight compresses inferior vena cava, reducing venous return; left lateral supports healthy fetal blood flow |
| Shoulder pain | Supine; or lateral on unaffected shoulder | Moderate — clinical consensus | Lying on the affected shoulder increases compressive load on the joint |
| Heart failure | Right lateral or semi-recumbent (clinician guidance essential) | Moderate — clinical observation; individual variation is high | Many heart failure patients experience dyspnea worsening on the left side; this is the opposite of GERD guidance — clinician input is essential before making positional changes |
Practical Adjustment Toolkit: Structural Aids and Behavioral Shaping
Because people naturally shift position 11–13 times per night, positional strategies should focus on starting position and structural support — not on demanding all-night positional maintenance, which is neither realistic nor necessary. The goal is to reduce time spent in high-risk positions (supine for OSA, right lateral for GERD, prone for spinal alignment) rather than to achieve perfect positional consistency.
- Pillow loft for cervical alignment: Low-loft pillow for back sleepers (keeps the cervical spine level with the thoracic spine). Medium-to-high loft for side sleepers (fills the gap between shoulder and ear). Using the wrong loft for your position creates cervical flexion or lateral bending stress during sleep.
- Wedge pillow: Elevates the head and torso at a stable angle for GERD management and OSA reduction. More effective than stacking standard pillows, which compress and shift during the night. Useful for people who need both head elevation and lateral positioning.
- Inter-knee pillow: Placed between the knees during lateral sleeping to maintain pelvic alignment and reduce rotational stress on the lumbar spine and hip. Particularly important for people with low back pain, hip pain, or sciatica.
- Body pillow: A full-length body pillow acts as a positional anchor, reducing the likelihood of rolling from lateral to supine during the night. Useful for people with OSA or GERD who need to maintain lateral positioning but find themselves waking in the supine position.
- Positional vibration devices and the tennis ball technique: For positional OSA, vibration-based wearable devices detect supine positioning and provide a gentle tactile prompt to shift. The tennis ball technique — securing a ball to the back of a sleep shirt — is a lower-cost behavioral aid with the same goal. Both are adjuncts to clinical OSA management, not substitutes for CPAP therapy.
- Starting position focus: Establishing the correct starting position before sleep onset, combined with appropriate structural support, is more effective and realistic than attempting to maintain position throughout the night. Natural position changes during sleep cycle transitions are normal and should not be suppressed.
Evidence Quality Summary: What Is Established, What Is Preliminary, and What Lacks Support
| Evidence Tier | Claims Included | Basis |
|---|---|---|
| Strong | Lateral position therapy for positional OSA; left lateral specifically for GERD (ACG 2022 guideline); prone sleeping as worst-case for cervical-lumbar spinal alignment | Clinical guidelines, systematic reviews, cohort studies, anatomical rationale |
| Moderate | Supine's dual role: neutral spinal alignment benefit vs. worsening of OSA, GERD, and late-pregnancy safety; inter-knee pillow for lateral spinal load; head elevation for GERD and OSA | Clinical consensus across multiple authoritative sources; mechanistic plausibility; limited primary research specifically on these interventions |
| Preliminary | Lateral sleeping and glymphatic transport efficiency (human benefit unproven as of 2026); right-lateral preference associated with longer slow-wave sleep and fewer awakenings (13-subject study) | Rodent MRI data (Lee et al. 2015); single small wearable study (Zhang et al. 2022); mechanistic plausibility from human glymphatic imaging |
| Absent or unsupported | Sleep position and wrinkle formation as a health concern; sleep position as a personality-type indicator; right-lateral glymphatic benefit as a clinical recommendation | No credible research basis; outside the scope of evidence-anchored sleep science |
When to Consult a Clinician
Positional self-management is a useful adjunct for many sleep-related conditions, but it has clear limits. The following situations warrant professional evaluation rather than positional adjustment alone.
- Suspected OSA: If you or a bed partner have observed loud snoring, witnessed breathing pauses, or you experience significant daytime sleepiness despite adequate time in bed, a sleep study is needed. Position therapy does not diagnose OSA and does not adequately treat moderate-to-severe OSA.
- GERD unresponsive to positional and dietary modification: Persistent reflux symptoms despite consistent left lateral positioning and head elevation should prompt evaluation. Untreated chronic GERD carries risks including esophageal inflammation and Barrett's esophagus.
- Pregnancy: If you are in the second or third trimester and uncertain about safe sleeping positions, or if you experience dizziness or shortness of breath in any position, discuss this with your obstetric provider. ACOG advises against supine sleeping in late pregnancy due to vena cava compression.
- Heart failure or cardiovascular conditions: Sleep position can meaningfully affect symptom burden in heart failure, and the optimal position varies by individual. Do not apply the general GERD or OSA lateral guidance without clinician input.
- Persistent neck or back pain attributed to sleep position: If positional adjustments and pillow changes do not relieve waking musculoskeletal pain within a few weeks, a physiotherapy or orthopedic evaluation may identify structural issues that require targeted treatment.
Supports these guides
Spot an error or have clinical feedback?
Because this article covers clinical, medication, or safety information, we use a moderated correction channel instead of open public comments. Let us know if something about “How Sleep Position Affects Sleep Quality and Health: The Mechanisms Behind the Mattress” needs a closer look.
Send feedback on this article