What Is MidNite? Ingredients and Formulation
MidNite is a branded dietary supplement marketed for occasional sleeplessness. Unlike many OTC sleep aids that rely on antihistamines, MidNite uses melatonin as its primary active ingredient — specifically 1.5 mg per serving. The product line includes the Original quick-dissolve tablet, a Back to Sleep variant, and Gummies (which contain 3 mg melatonin).
The Original and Back to Sleep formulations each deliver 1.5 mg of melatonin plus a proprietary botanical blend of lemon balm, chamomile, and lavender. The Gummies contain 3 mg of melatonin with a 10 mg blend of chamomile and lavender. All variants are labeled as non-habit forming, gluten-free, lactose-free, vegetarian, and vegan. The manufacturer advises adults 18 and older to dissolve one tablet in the mouth without water and allow at least three hours of sleep afterward, with a maximum of two tablets or gummies per 24-hour period.
How Melatonin Differs Pharmacologically from Antihistamine Sleep Aids
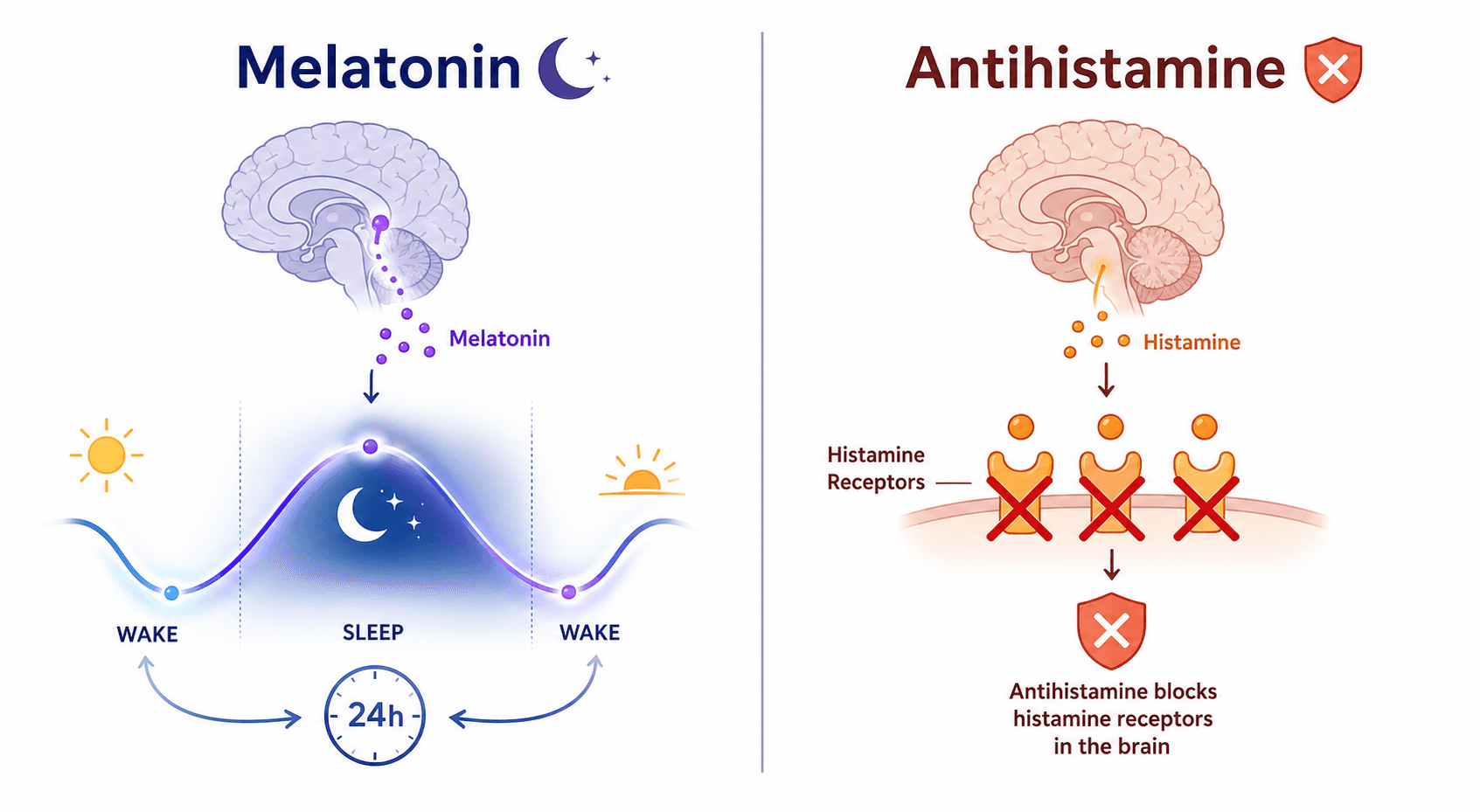
The most common OTC sleep aids — Unisom (doxylamine) and Benadryl (diphenhydramine) — belong to a class called first-generation antihistamines. They work by crossing the blood-brain barrier and blocking histamine H1 receptors, which produces a sedative effect as a side reaction. This mechanism is indirect and comes with several drawbacks: tolerance develops quickly (often within a few days), and the anticholinergic activity of these drugs has been linked to cognitive decline and an increased risk of dementia in older adults.
Melatonin operates through an entirely different pathway. It is a naturally occurring hormone synthesized by the pineal gland in response to darkness. Its primary role is to signal the body that it is time to prepare for sleep by regulating the circadian rhythm — the internal biological clock that governs the sleep-wake cycle. Melatonin does not force sedation the way an antihistamine does; it shifts the timing of sleep readiness. This distinction matters for safety: melatonin is not considered habit-forming, and its side effect profile is generally milder, though not risk-free.
The American Academy of Sleep Medicine (AASM) clinical practice guidelines advise against using melatonin for chronic insomnia, but acknowledge its utility for circadian rhythm-related issues such as jet lag and shift work disorder. Antihistamine-based sleep aids, by contrast, are not recommended by the AASM for insomnia at all, due to their limited efficacy and well-documented side effects.
MidNite vs. Unisom vs. Benadryl vs. High-Dose Melatonin: A Comparison
The following table provides a side-by-side comparison of the most common OTC sleep aid categories. This is the core decision-making tool for readers weighing their options.
| Feature | MidNite (Melatonin) | Unisom (Doxylamine) | Benadryl (Diphenhydramine) | High-Dose Melatonin (5–10 mg) |
|---|---|---|---|---|
| Active Ingredient(s) | 1.5 mg melatonin + botanical blend | 25 mg doxylamine succinate | 25–50 mg diphenhydramine HCl | 5–10 mg melatonin |
| Mechanism | Circadian rhythm signaling (hormonal) | Histamine receptor blockade (sedation) | Histamine receptor blockade (sedation) | Circadian rhythm signaling (hormonal) |
| Onset of Action | 30–60 minutes (timing-dependent) | 15–30 minutes | 15–30 minutes | 30–60 minutes (timing-dependent) |
| Tolerance Risk | Not established (low risk) | Develops within days | Develops within days | Not established (low risk) |
| Next-Day Grogginess | Mild (dose-dependent) | Common (long half-life) | Common (long half-life) | Mild (dose-dependent) |
| Anticholinergic Effects | None | Yes (dry mouth, constipation, urinary retention) | Yes (dry mouth, constipation, urinary retention) | None |
| Dementia Risk (Older Adults) | Not established (see AHA 2025 study below) | Increased risk (anticholinergic burden) | Increased risk (anticholinergic burden) | Not established (see AHA 2025 study below) |
| Regulatory Status | Dietary supplement (DSHEA) | FDA-approved OTC drug | FDA-approved OTC drug | Dietary supplement (DSHEA) |
What the Evidence Says About Low-Dose Melatonin Efficacy
A common misconception is that higher melatonin doses produce better sleep. The evidence points in the opposite direction. Multiple sleep experts and organizations, including the Sleep Foundation, recommend starting with the lowest possible dose — typically 1 mg or less — because going above 2–3 mg is unlikely to work any better and increases the risk of side effects such as headache, daytime sleepiness, and grogginess.
MidNite's 1.5 mg dose falls squarely within the low-dose range (0.3–1.5 mg) that research suggests may be as effective as higher doses for sleep onset. This is a meaningful differentiator in a market where many melatonin products contain 5 mg, 10 mg, or even higher amounts — doses that are rarely necessary and may contribute to next-day drowsiness without additional benefit.
The AASM notes that melatonin can be a treatment option for jet lag and shift work disorder, but it is not recommended for chronic insomnia. For occasional sleeplessness — the target use case for MidNite — low-dose melatonin may help shift the sleep rhythm and reduce the time it takes to fall asleep, particularly when taken 1–2 hours before the desired bedtime.
Safety Profile, Contraindications, and Who Should Avoid MidNite
Melatonin is generally well-tolerated in the short term. The most commonly reported side effects include headache, dizziness, daytime sleepiness, grogginess, and nausea. These are typically mild and dose-dependent. Because melatonin has a short half-life, next-day grogginess is less pronounced than with antihistamine-based aids, but it can still occur, especially at higher doses.
However, melatonin is not risk-free, and certain populations should exercise caution or avoid it entirely:
- Pregnant or nursing women: The MidNite manufacturer explicitly advises against use during pregnancy and breastfeeding. No adequate safety data exist for these populations.
- Older adults: The AHA 2025 observational study raises a potential signal for increased heart failure risk and all-cause mortality with long-term use. While the study has limitations (observational, not yet peer-reviewed), it warrants caution, especially for older adults who may already have cardiovascular risk factors.
- Individuals with autoimmune conditions: Melatonin can modulate immune function. Those with autoimmune disorders should consult a healthcare provider before use.
- Children and adolescents: The 2025 PMC review documented a 530% increase in calls to US Poison Control Centers for pediatric melatonin ingestions between 2012 and 2021, resulting in thousands of emergency department visits and hospitalizations. MidNite is labeled for adults 18 and older only.
By contrast, the risks of antihistamine-based sleep aids are well-established and more severe for certain groups. The Mayo Clinic notes that these drugs are not recommended for people with closed-angle glaucoma, peptic ulcer, or urinary retention. For adults over 65, the anticholinergic effects of diphenhydramine and doxylamine are linked to an increased risk of dementia and falls. The Harvard Health review emphasizes that tolerance to antihistamine sleep aids develops quickly — often within a few days — making them unsuitable for regular use.
Label Accuracy Concerns: Why Brand Reliability Matters
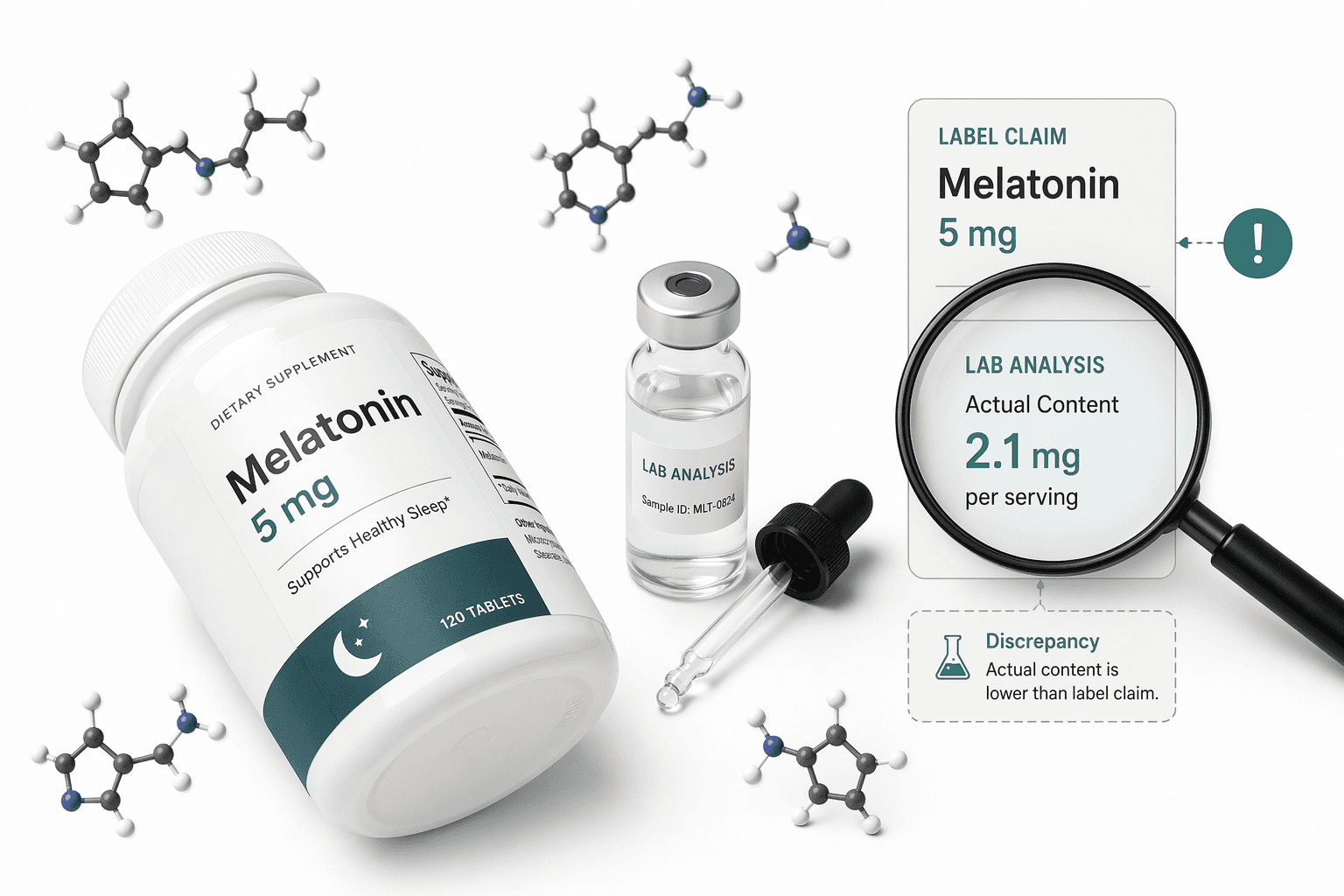
One of the most significant concerns with melatonin supplements — and one that directly affects the reliability of any product, including MidNite — is the widespread problem of inaccurate labeling. Multiple studies have documented that the majority of melatonin supplements on the market do not contain the amount of melatonin stated on the label.
A landmark 2017 study by Erland and Saxena found that over 71% of melatonin supplements were inaccurately labeled, with actual melatonin content ranging from 83% less to 478% more than the label claim. A more recent 2023 study by Cohen et al., published in JAMA, analyzed 25 melatonin gummy products and found that 88% (22 out of 25) were inaccurately labeled. Actual content ranged from 74% to 347% of the labeled quantity. Only three products (12%) were within ±10% of the declared amount.
This variability means that a product labeled as 5 mg could contain anywhere from less than 1 mg to over 17 mg of melatonin. For a low-dose product like MidNite, which relies on the precision of its 1.5 mg dose, label accuracy is not a minor detail — it is central to the product's value proposition.
Practical Guidance: When to Choose MidNite vs. Alternatives
The choice between MidNite, an antihistamine-based sleep aid, or a higher-dose melatonin product depends on your specific situation, risk factors, and the nature of your sleep difficulty. The following guidance is based on the evidence reviewed above.
- Choose MidNite (or another low-dose melatonin product) if: You have occasional sleeplessness related to timing issues — difficulty falling asleep at your desired bedtime, jet lag, or shift work. You want to avoid the tolerance and anticholinergic risks of antihistamines. You are under 65 and have no contraindications (pregnancy, autoimmune conditions, or cardiovascular risk factors). The low 1.5 mg dose aligns with the evidence that more is not better.
- Consider an antihistamine-based aid (Unisom, Benadryl) only for: Very short-term use (1–2 nights) when you need rapid sedation and have no contraindications. Do not use these regularly. Avoid entirely if you are over 65, have glaucoma, peptic ulcer, or urinary retention. The Mayo Clinic and Harvard Health both caution that tolerance develops quickly and the risks outweigh benefits for ongoing use.
- Avoid high-dose melatonin (5–10 mg) if: You are new to melatonin. Start with 1 mg or less. Higher doses do not improve efficacy for sleep onset and increase the risk of side effects like next-day grogginess and headache. Reserve higher doses for specific, medically supervised applications such as delayed sleep-wake phase disorder.
- Consult a healthcare provider if: Your sleeplessness persists for more than four weeks, you have underlying health conditions, or you are taking other medications. Melatonin can interact with blood thinners, immunosuppressants, and diabetes medications.
Comments
Join the discussion with an anonymous comment.