Why 'Best' Is the Wrong Question
If you search for "best sleep supplement," you will find dozens of articles claiming a single winner. The problem is that sleep disruption is not a single condition. Trouble falling asleep, waking up at 3 a.m. with a racing mind, age-related light sleeping, and jet lag are physiologically distinct problems. A supplement that helps one can be useless — or counterproductive — for another.
Melatonin, for example, is well-supported for sleep-onset insomnia and jet lag, but it does not reliably help people who wake up in the middle of the night. Magnesium glycinate targets age-related sleep changes and stress-related muscle tension, but it will not fix a circadian rhythm disorder. L-theanine calms an overactive mind without causing daytime drowsiness, yet it does not shorten the time it takes to fall asleep.
Nearly 70 million U.S. adults are affected by poor sleep, and roughly 18% use a sleep aid regularly, according to a 2024 review in PMC. Yet most people pick a supplement based on brand recognition or a friend's recommendation rather than matching it to their actual sleep problem. The result is wasted money, unnecessary side effects, and continued poor sleep.
The sections below walk through five common sleep problem profiles. Each includes the supplement with the best evidence for that profile, a typical dose range, and the safety caveats you need to know before trying it.
Quick Self-Assessment: Identify Your Primary Sleep Problem
Before reading the detailed sections, take 30 seconds to identify which profile fits you best. Be honest about your dominant symptom — most people have more than one, but one is usually the primary driver.
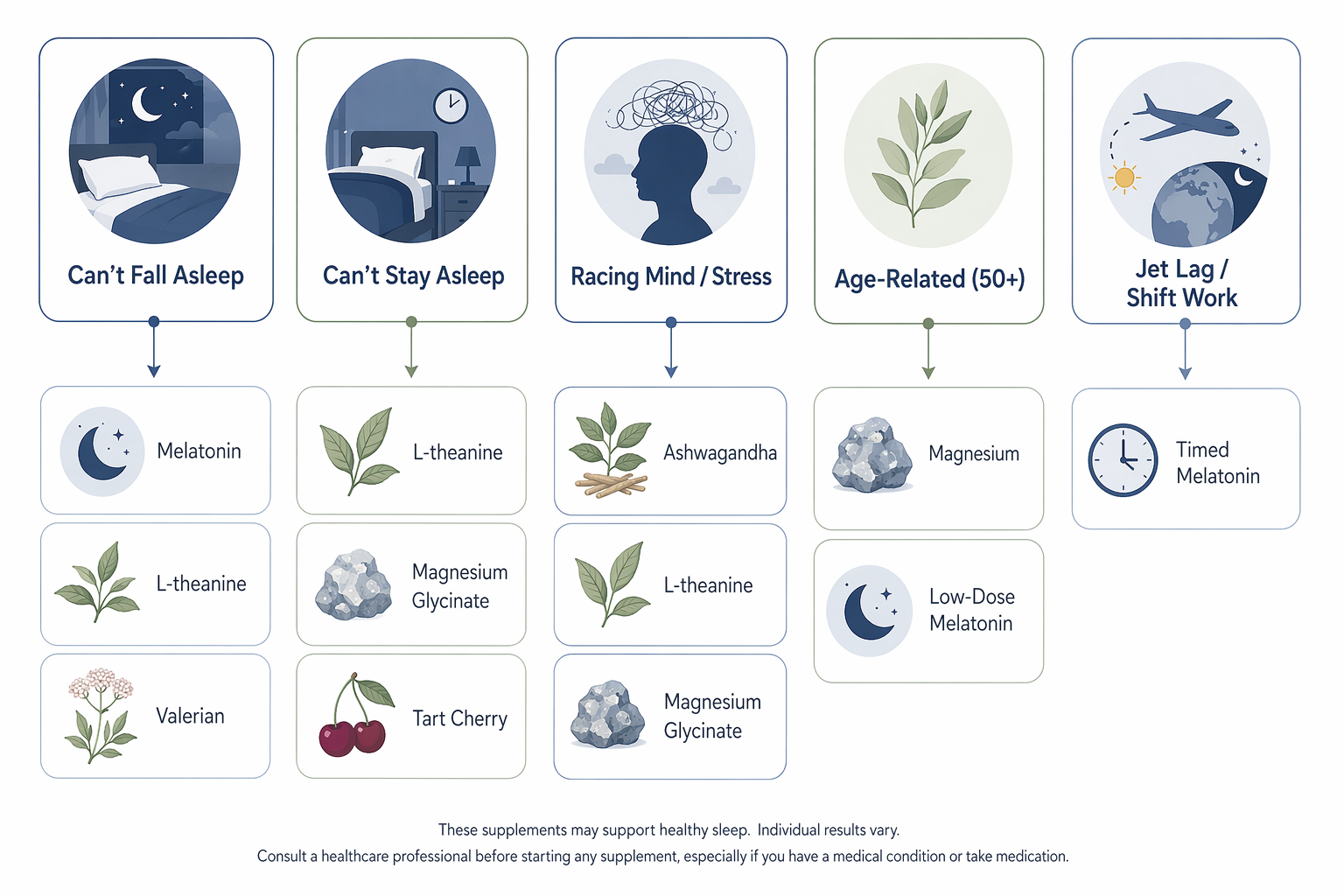
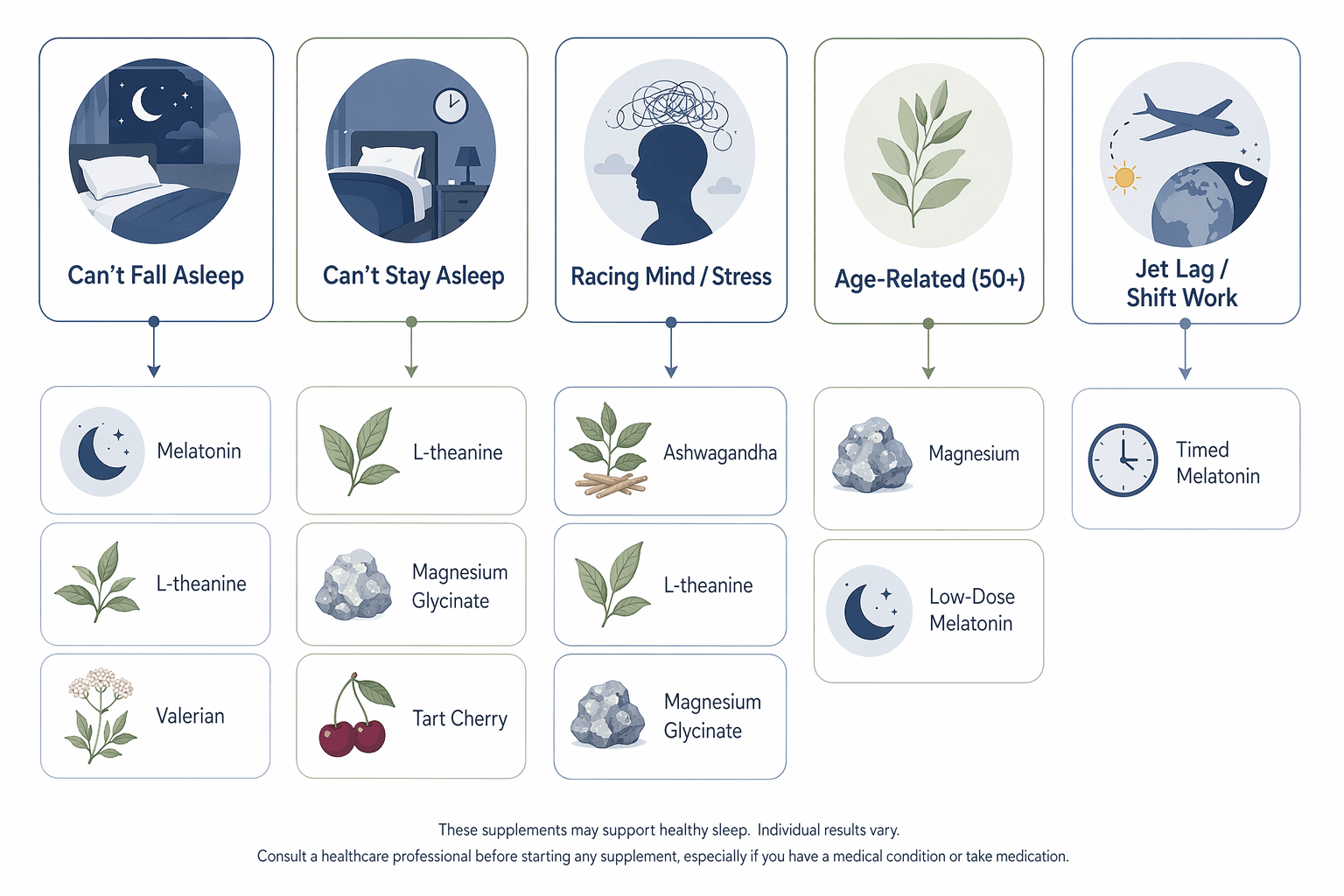
- Problem 1: Can't fall asleep. You lie in bed for 30 minutes or more before sleep comes. Your mind may be quiet, but sleep simply does not arrive.
- Problem 2: Can't stay asleep. You fall asleep fine but wake up once or multiple times during the night and struggle to get back to sleep.
- Problem 3: Racing mind, stress, or anxiety. Your body is tired, but your brain will not shut off. You replay the day or worry about tomorrow. Cortisol is likely elevated in the evening.
- Problem 4: Age-related sleep changes (50+). You sleep less deeply than you used to, wake more easily, and may feel that your sleep is lighter and less restorative. Melatonin production naturally declines with age.
- Problem 5: Jet lag or shift work. Your sleep problem is tied to a disrupted circadian rhythm — traveling across time zones or working nights. Your body wants to sleep at the wrong time.
If you are unsure, start with Problem 1 or Problem 3 — those are the most common profiles among adults who search for sleep supplements. If your sleep problem has lasted more than three months and significantly affects your daytime function, see the note at the end of this guide about when supplements are not the answer.
Problem 1: Can't Fall Asleep (Sleep-Onset Insomnia)
If you regularly lie awake for 30 minutes or more before falling asleep, you are dealing with sleep-onset insomnia. The goal here is to reduce the time it takes to transition from wakefulness to sleep — not necessarily to change sleep depth or duration.
Primary Recommendation: Melatonin
Melatonin is the most studied supplement for sleep-onset problems. A meta-analysis of 19 RCTs found that melatonin significantly reduces sleep latency and increases total sleep time in primary insomnia, with the strongest effects in older adults and people with delayed sleep phase syndrome. A separate PLOS ONE meta-analysis calculated that melatonin helps people fall asleep about 7 minutes faster on average.
The effective dose range is 0.5 to 3 mg, taken 30 to 60 minutes before bed. Higher doses (above 5 mg) are rarely needed and may increase the risk of next-day drowsiness and headache. A 2017 study in the Journal of Clinical Sleep Medicine found that more than 71% of melatonin supplements contained amounts that differed from their label by more than 10%, with actual content ranging from 83% less to 478% more than stated. Choose a brand that uses third-party testing if label accuracy matters to you.
For a detailed breakdown of how to match melatonin dose and timing to your specific sleep problem, see our Melatonin Dosage Guide.
Secondary Options: L-Theanine and Valerian
L-theanine (100–200 mg) does not directly induce sleep, but it increases GABA production and promotes a calm, relaxed state that can make it easier to fall asleep. It is a good option if your sleep-onset difficulty is accompanied by mild tension rather than full-blown anxiety.
Valerian root (300–600 mg, taken up to an hour before bed) has mixed evidence. A meta-analysis of 18 RCTs found a significant reduction in sleep latency (SMD: -0.71) and improved sleep quality, but the quality of evidence was rated low to moderate. Some people experience next-day grogginess with valerian, which may be a tradeoff worth considering. For a deeper look at the evidence and safety profile, see our Valerian Root for Sleep article.
| Supplement | Typical Dose | Evidence Level | Key Notes |
|---|---|---|---|
| Melatonin | 0.5–3 mg | RCT-supported (19 RCTs) | ~7 min faster sleep onset; most effective for jet lag and delayed phase |
| L-Theanine | 100–200 mg | RCT-supported | Calms without sedation; does not directly induce sleep |
| Valerian Root | 300–600 mg | Moderate (low-quality RCTs) | Reduces sleep latency 15–20 min; may cause next-day grogginess |
Problem 2: Can't Stay Asleep (Sleep-Maintenance Insomnia)
Falling asleep is not the issue — staying asleep is. You wake up once or multiple times during the night and may lie awake for 20 minutes or more before drifting back off. Sleep-maintenance insomnia is often linked to stress, blood sugar fluctuations, or age-related changes in sleep architecture.
Primary Recommendation: L-Theanine
L-theanine stands out for sleep maintenance because it reduces night wakings without causing daytime sleepiness. A 2019 RCT by Hidese et al. found that 200 mg of L-theanine daily significantly improved PSQI scores, decreased stress-related symptoms, and enhanced cognitive function versus placebo. Unlike many sleep aids, L-theanine does not suppress REM sleep or leave you groggy the next morning.
For a full review of the evidence, dosing, and safety profile, see our L-Theanine for Sleep article.
Secondary Options: Magnesium Glycinate, Tart Cherry, and Extended-Release Melatonin
Magnesium glycinate (200–400 mg) supports GABA receptor function and muscle relaxation, which can reduce the likelihood of waking due to muscle tension or restlessness. It is particularly useful if your night wakings are accompanied by physical tension or restless legs.
Tart cherry juice concentrate has a different mechanism: it provides a natural source of melatonin. A 7-day RCT by Howatson et al. in 20 adults found that tart cherry juice concentrate significantly increased total sleep time and sleep efficiency as measured by actigraphy. If you prefer a food-based approach, this is a reasonable option.
Extended-release melatonin is designed to release melatonin gradually throughout the night, which may help with sleep maintenance. Standard immediate-release melatonin is not the best choice here — it peaks quickly and declines, which does not align with the need for sustained coverage across the night.
| Supplement | Typical Dose | Evidence Level | Key Notes |
|---|---|---|---|
| L-Theanine | 200 mg | RCT-supported | Reduces night wakings; no daytime sleepiness |
| Magnesium Glycinate | 200–400 mg | Limited RCTs | Supports GABA and muscle relaxation |
| Tart Cherry Juice | 8–16 oz concentrate | Single RCT | Natural melatonin source; small sample size |
| Extended-Release Melatonin | 1–3 mg | Limited evidence | Better for maintenance than immediate-release |
Problem 3: Racing Mind, Stress, or Anxiety
This profile is distinct from simple sleep-onset insomnia. The body is tired, but the mind is active — replaying conversations, planning tomorrow, or worrying. The driver is often elevated evening cortisol, which conflicts with the natural melatonin rise that should prepare you for sleep. For a deeper look at the physiological mechanism behind this conflict, see our article on Why Anxiety Gets Worse at Night.
Primary Recommendation: Ashwagandha
Ashwagandha is one of the few supplements with direct evidence for stress-related sleep disruption. A meta-analysis of 5 studies published in PLOS ONE in 2021 found that ashwagandha significantly improved overall sleep compared to placebo, with a standardized mean difference of -0.59. The effect was more pronounced in people with insomnia than in those without, and the benefits were strongest after at least 8 weeks of consistent use.
The typical dose is 300–600 mg per day, standardized to withanolide content. Ashwagandha is believed to work by lowering cortisol levels and affecting GABA receptors. It is generally safe for up to 3 months, but it should be avoided during pregnancy and breastfeeding, and by people with thyroid disorders, autoimmune conditions, or prostate cancer. It can interact with medications for high blood pressure, diabetes, and thyroid problems.
Secondary Options: L-Theanine and Magnesium Glycinate
L-theanine (100–200 mg) increases GABA production, which promotes calm without sedation. It works well for mild-to-moderate anxiety-driven wakefulness and can be taken alongside ashwagandha or magnesium glycinate.
Magnesium glycinate (200–400 mg) lowers cortisol and supports the parasympathetic nervous system. It is a good option if your stress-related sleep disruption includes physical tension or muscle tightness.
| Supplement | Typical Dose | Evidence Level | Key Notes |
|---|---|---|---|
| Ashwagandha | 300–600 mg | Meta-analysis (SMD -0.59) | Best for cortisol-driven disruption; takes 8+ weeks |
| L-Theanine | 100–200 mg | RCT-supported | Calms without sedation; safe with other supplements |
| Magnesium Glycinate | 200–400 mg | Limited RCTs | Lowers cortisol; supports muscle relaxation |
Problem 4: Age-Related Sleep Changes (50+)
As we age, sleep architecture changes. Deep sleep (N3) decreases, nighttime awakenings increase, and melatonin production declines. These changes are normal, but they can significantly affect sleep quality. The goal for this profile is to support the physiological systems that decline with age — melatonin production, magnesium status, and vitamin D levels.
Primary Recommendation: Magnesium
Magnesium has the strongest evidence for age-related sleep changes. A 2012 RCT by Abbasi et al. in 46 older adults found that 500 mg of magnesium daily for 8 weeks significantly increased sleep time, sleep efficiency, serum renin, and melatonin levels, while significantly reducing insomnia severity, sleep onset latency, and serum cortisol. This is one of the few RCTs specifically targeting the older adult population.
Magnesium glycinate is the preferred form for sleep because it is well-absorbed and less likely to cause digestive issues than magnesium oxide or citrate. For a detailed comparison of magnesium forms and dosing, see our Magnesium Glycinate for Sleep article.
Secondary Options: Low-Dose Melatonin and Vitamin D
Low-dose melatonin (0.5–1 mg) may be beneficial for older adults who are melatonin deficient. The Mayo Clinic notes that melatonin might be more beneficial for older adults who could be melatonin deficient. Higher doses are not necessary and may increase side effects.
Vitamin D is relevant if you are deficient. A meta-analysis of 9,397 participants found that vitamin D deficiency increased the likelihood of poor-quality sleep and sleep disorders by 1.5-fold. A separate RCT by Majid et al. found that 50,000 IU of vitamin D3 bi-weekly for 8 weeks significantly improved PSQI scores, reduced sleep latency, and decreased sleep disturbances in 20- to 50-year-olds with sleep disorders. If you are over 50 and have not had your vitamin D levels checked recently, it is worth discussing with your doctor.
| Supplement | Typical Dose | Evidence Level | Key Notes |
|---|---|---|---|
| Magnesium (glycinate) | 500 mg | RCT-supported (46 older adults) | Increased sleep time, efficiency, melatonin; reduced cortisol |
| Melatonin (low-dose) | 0.5–1 mg | Expert consensus | May help melatonin-deficient older adults |
| Vitamin D3 | 50,000 IU bi-weekly | RCT-supported (if deficient) | Only if deficient; improves PSQI and sleep latency |
Problem 5: Jet Lag and Shift Work
Jet lag and shift work are circadian rhythm disorders, not sleep disorders per se. The problem is that your internal clock is out of sync with your environment. The goal is to help reset that clock, not to sedate yourself into sleep.
Primary Recommendation: Melatonin (for Jet Lag)
Melatonin is the most evidence-supported supplement for jet lag. A Cochrane review confirmed its efficacy for reducing jet lag symptoms, and the Mayo Clinic states that evidence shows it can improve jet lag symptoms. The dose range is 0.5 to 5 mg, with 3 mg being sufficient for most people. Timing is critical: for eastward travel, take melatonin at the target bedtime in the new time zone; for westward travel, timing is more flexible but still aligned with the new bedtime.
For a comprehensive review of melatonin evidence across different sleep problems, see our Melatonin for Sleep: Evidence, Dosage, and Safety by Population article.
Shift Work: A Different Story
Melatonin is less clearly effective for shift work disorder. The Mayo Clinic notes that evidence is not clear for shift work disorder. The reason is that shift work involves a conflict between the internal clock and the external environment that is harder to resolve with a single supplement. Behavioral strategies — strategic light exposure, consistent sleep scheduling, and blackout curtains — are the first-line approach for shift workers. Melatonin may be used as an adjunct, but it should not be relied upon as the primary solution.
| Condition | Supplement | Typical Dose | Evidence Level | Key Notes |
|---|---|---|---|---|
| Jet Lag | Melatonin | 0.5–5 mg | Cochrane review confirmed | Timing depends on travel direction |
| Shift Work | Melatonin (adjunct) | 0.5–3 mg | Unclear efficacy | Behavioral strategies are first-line |
Combination Cautions: What Stacks Work and What Doesn't
Combining supplements can be safe and even synergistic when the mechanisms are complementary. But some combinations carry real risks, especially when prescription medications are involved.
Safe Combinations
- Magnesium + L-theanine: These two have complementary mechanisms — magnesium supports GABA and muscle relaxation, L-theanine increases GABA production and promotes calm. They are safe to take together and may be more effective than either alone.
- Magnesium + melatonin + zinc: A 2011 RCT by Rondanelli et al. in 43 older adults with primary insomnia found that a combination of 5 mg melatonin, 225 mg magnesium, and 11.25 mg zinc significantly improved PSQI, sleep quality, morning alertness, and quality of life over 8 weeks. This combination is well-tolerated in the studied population.
Risky Combinations
- Kava + anything with CNS depressant effects: Kava carries a hepatotoxicity risk on its own. Combining it with alcohol, benzodiazepines, or other CNS depressants increases the risk of liver injury and excessive sedation.
- Valerian + benzodiazepines or other CNS depressants: Valerian can potentiate the effects of benzodiazepines and other sedatives, leading to excessive drowsiness and impaired coordination.
- Melatonin + blood thinners or SSRIs: Melatonin may increase bleeding risk when combined with anticoagulants. It should not be combined with the SSRI fluvoxamine, which can cause excessive drowsiness. Caution is also advised with other SSRIs.
- Tart cherry + blood thinners: The quercetin content in tart cherry can interact with anticoagulants and anti-platelet drugs.
Summary Decision Table
Use this table as a quick reference to match your primary sleep problem to the supplement with the strongest evidence, typical dose, and key safety notes.
| Sleep Problem | Recommended Supplement(s) | Typical Dose Range | Evidence Level | Key Safety Notes |
|---|---|---|---|---|
| Can't fall asleep (sleep-onset) | Melatonin | 0.5–3 mg | RCT-supported (19 RCTs) | Avoid with fluvoxamine; caution with blood thinners |
| Can't stay asleep (maintenance) | L-Theanine | 200 mg | RCT-supported | No daytime sleepiness; safe with most supplements |
| Racing mind / stress / anxiety | Ashwagandha | 300–600 mg | Meta-analysis (SMD -0.59) | Avoid in pregnancy, thyroid disorders, autoimmune conditions |
| Age-related changes (50+) | Magnesium (glycinate) | 500 mg | RCT-supported (46 older adults) | Caution in kidney disease; check for drug interactions |
| Jet lag | Melatonin | 0.5–5 mg | Cochrane review confirmed | Timing depends on travel direction |
| Shift work | Melatonin (adjunct) | 0.5–3 mg | Unclear efficacy | Behavioral strategies are first-line |

Comments
Join the discussion with an anonymous comment.