Mechanism explainer
Evening Wind-Down Routine for Better Sleep: Evidence-Based Steps and Timing
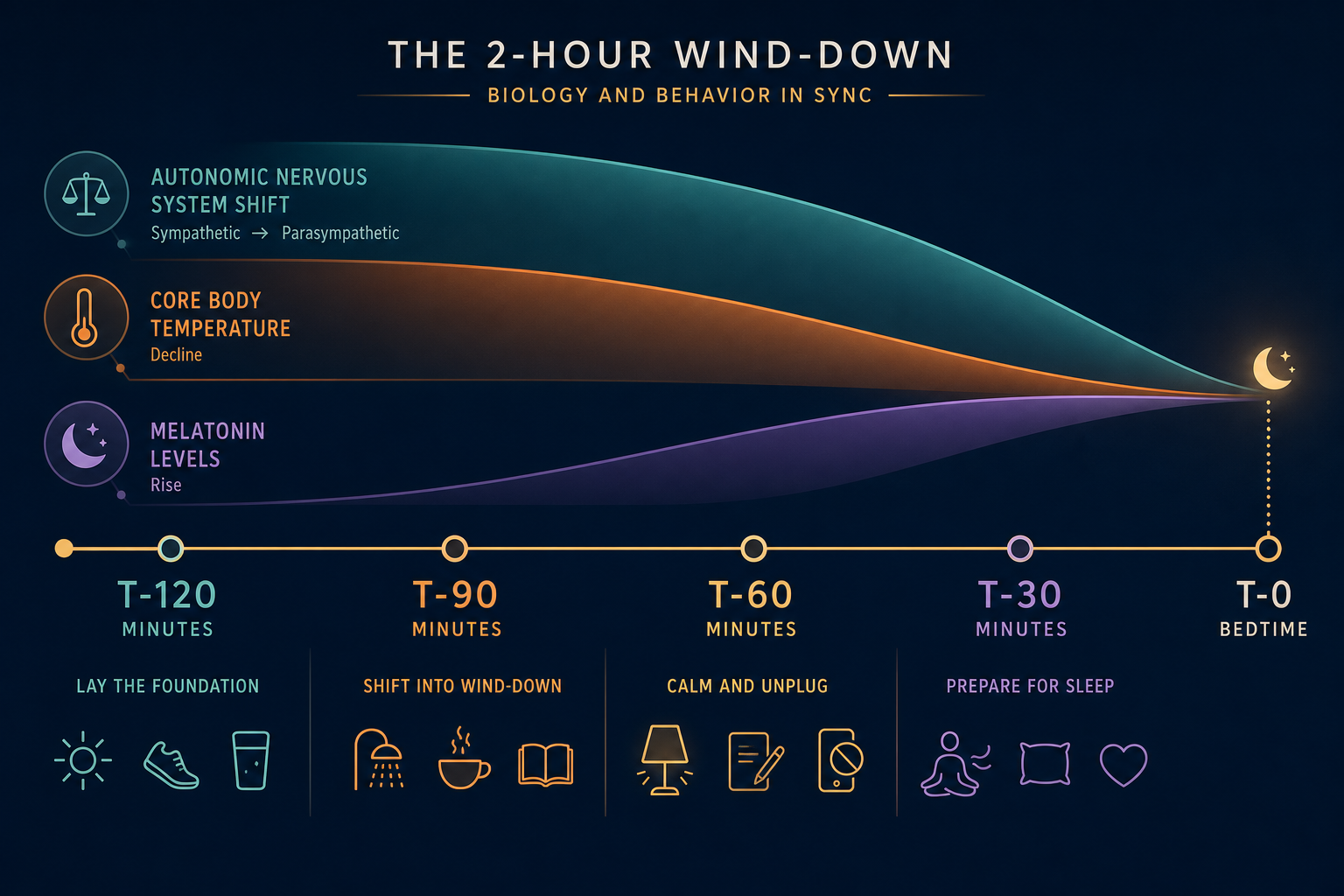
A reliable evening wind-down routine is not a collection of calming activities but a sequenced protocol aligned with three overlapping physiological transitions — autonomic nervous system downshift, core body temperature decline, and melatonin rise. This guide explains the biology behind each transition and provides a phase-gated 2-hour countdown with specific, evidence-grounded actions and timing rationale at each phase.

Why Routines Fail: The Timing and Sequencing Gap
Most people who try a wind-down routine pick reasonable activities — putting the phone down, dimming the lights, maybe reading for a few minutes. The problem is rarely what they choose. It is when they start and in what order they do it.
The sympathetic nervous system — the branch responsible for alertness, vigilance, and stress response — does not stand down on command. Once it is activated by a stressful email, a tense news cycle, or a late workout, returning to a baseline calm state takes between 30 and 90 minutes for most adults. Willpower cannot compress that timeline. Trying to fall asleep 10 minutes after closing a work laptop is physiologically similar to trying to stop a moving car by wishing it to stop.
The second failure mode is sequencing: doing calming activities in the wrong order, or mixing arousing and calming behaviors within the same window. Checking one last email at 10:45 PM while lying in bed undoes the dimming and quiet that preceded it. The nervous system reads that email as a signal to stay alert, regardless of how tired you feel.
This article is organized around a different approach: a phase-gated 2-hour countdown that aligns specific behaviors with three overlapping physiological transitions that must occur before sleep onset. Understanding those transitions — and why each phase of the countdown targets a different one — is what separates a routine that works from one that feels like it should work but doesn't.
The Three Physiological Targets Your Routine Must Hit
Sleep onset is not a single switch. It requires three overlapping biological transitions to converge — and each one has its own timeline. A wind-down routine that addresses only one or two of them will feel incomplete.
- Autonomic nervous system shift — from sympathetic (alert, reactive) to parasympathetic (calm, restorative) dominance. This transition takes 30 to 90 minutes under normal conditions and cannot be accelerated by effort alone. It requires the absence of activating inputs, not just the presence of calming ones.
- Core body temperature decline — a drop of approximately 0.5 to 1°F that begins roughly 60 to 90 minutes before habitual sleep onset. This cooling is driven by the body redirecting blood flow from the core to the extremities (hands and feet), which dissipates heat outward. Without this drop, sleep initiation is delayed.
- Melatonin rise — the pineal gland begins releasing melatonin approximately 2 hours before habitual sleep onset under dim-light conditions. This timing point is called dim-light melatonin onset (DLMO). Light exposure — especially short-wavelength blue light — suppresses melatonin secretion and can delay DLMO by 30 to 60 minutes or more.
These three transitions are overlapping, not sequential. Melatonin begins rising while the autonomic shift is still underway. Core temperature starts declining before melatonin has fully risen. This is precisely why a single pre-bed activity — even a good one — cannot do the job. A 2023 review in Sleep Medicine Clinics by Swanson and Raglan confirmed that falling body temperature and rising melatonin together herald sleep onset, and that misalignment between behavioral sleep timing and circadian propensity is a primary driver of sleep-onset insomnia.
The 2-Hour Countdown: What to Do at Each Phase
The countdown below is anchored to your target bedtime — the time you want to be asleep, not just in bed. Each phase targets one or more of the three physiological transitions with specific actions and a mechanistic reason for the timing.
T-120 Minutes: Begin the Physiological Transition
Two hours before bed is when the wind-down must actually start — not when you begin to feel tired. At this point, melatonin onset is approximately 2 hours away under ideal conditions, and any activating input now will delay it.
- Dim the lights to 50 lux or below. This is roughly the level of a single table lamp with a warm-toned bulb, not overhead lighting. Research confirms that dim-light conditions of 50 lux or less should begin at least 90 minutes before bed and ideally 120 minutes for people with sleep-onset difficulty.
- Stop emotionally arousing content. News, social media feeds, intense TV drama, and work email are not neutral — they produce cortisol responses that actively oppose the autonomic downshift you need. Cortisol follows a natural circadian decline through the evening; these inputs interrupt that decline at precisely the wrong time.
- Finish your last heavy meal if you have not already. Digestion elevates core body temperature and metabolic activity, working against the temperature decline needed for sleep. Aim to finish eating 2 to 3 hours before bed.
T-90 Minutes: The Warm Bath Window
This is the most precisely timed intervention in the entire protocol, and the one with the strongest research backing.
A systematic review and meta-analysis by Haghayegh and colleagues examined 5,322 candidate studies on water-based passive body heating before sleep. When a warm bath or shower at 40–42.5°C (104–108.5°F) was scheduled 1 to 2 hours before bedtime and lasted at least 10 minutes, it significantly shortened sleep onset latency — by approximately 10 minutes on average — and improved self-rated sleep quality and sleep efficiency.
The mechanism is not sedation. Hot water raises skin temperature, which triggers the thermoregulatory system to increase blood perfusion to the palms and soles. This peripheral vasodilation dissipates body heat outward, accelerating the core temperature decline that the circadian system is already trying to produce. The warm bath does not replace that decline — it amplifies and advances it, so the temperature drop aligns with bedtime rather than lagging behind it.
T-60 Minutes: Protect the Melatonin Window
By now the autonomic shift should be underway and core temperature should be declining. The priority at this phase is protecting melatonin onset by maintaining dim-light conditions and avoiding any re-activation.
- Continue the dim-light environment established at T-120. Avoid turning on overhead lights, opening bright app screens, or moving to a brightly lit room.
- Read a physical book. This is one of the few cognitively engaging activities that does not produce cortisol elevation or light-based melatonin suppression. It occupies the mind without activating it.
- Gentle stretching or light household tasks (folding laundry, tidying) are acceptable if they are not mentally stimulating. The goal is low-arousal physical activity, not exercise.
- No screens. Even with night-mode or blue-light filters, the interactive nature of phones and computers produces cognitive activation that is separate from the light issue.
T-30 Minutes: Cognitive Offloading
The final phase addresses the most common remaining barrier: a mind that is physiologically calm but still running through tomorrow's tasks, unresolved problems, or anxious loops. This is the cognitive vigilance problem, and it requires a specific technique — not just relaxation.
- Tomorrow's to-do list journaling. Write out the specific tasks you need to complete the next day — not a reflection on today, not problem-solving, just a concrete list of next steps. Research by Scullin and colleagues (2018, Journal of Experimental Psychology) found that writing a future-oriented to-do list before bed significantly reduced sleep onset latency. The effect was specific to writing future tasks; journaling about past events did not produce the same benefit. The mechanism is externalization — writing the list offloads the brain's need to keep rehearsing the tasks to avoid forgetting them.
- Breathwork for parasympathetic acceleration. Several breathing patterns have evidence for rapid autonomic downshift. The physiological sigh — a double nasal inhale followed by a long, slow exhale — deflates collapsed alveoli and activates the parasympathetic branch quickly. Box breathing (inhale 4 counts, hold 4, exhale 4, hold 4) and the 4-7-8 pattern (inhale 4, hold 7, exhale 8) are also commonly used. Any of these, practiced for 3 to 5 minutes, can accelerate the shift that has been building across the prior 90 minutes.
| Phase | Time Before Bed | Primary Target | Key Actions |
|---|---|---|---|
| T-120 | 2 hours | Melatonin onset protection; cortisol decline | Dim lights to 50 lux; stop screens and emotionally arousing content; finish last heavy meal |
| T-90 | 90 minutes | Core body temperature decline | Warm bath or shower at 104–108.5°F (40–42.5°C) for 10–20 minutes |
| T-60 | 1 hour | Melatonin window maintenance; continued autonomic shift | Maintain dim light; physical book reading; gentle stretching; no screens |
| T-30 | 30 minutes | Cognitive arousal / vigilance loops | Tomorrow's to-do list journaling; breathwork (physiological sigh, box breathing, or 4-7-8) |
The Stop-Doing List: Specific Cutoff Times That Matter
The countdown above tells you what to do. This section consolidates what to stop doing, with specific usable numbers rather than vague guidance. Each cutoff is tied to a physiological mechanism.
| Behavior | Cutoff Before Bed | Why It Matters |
|---|---|---|
| Bright light / screens | 90–120 minutes | Light at 50 lux or above suppresses melatonin secretion; bright light exposure as late as 10 PM can delay DLMO by 30–60 minutes after exposure ends |
| Emotionally arousing content (news, social media, intense drama) | 120 minutes | Produces cortisol spikes during the window when cortisol should be declining; delays autonomic downshift |
| Vigorous exercise | 120 minutes minimum | Raises core body temperature and cortisol for 1–3 hours post-exercise; both oppose the transitions needed for sleep onset |
| Heavy meals | 2–3 hours | Digestion elevates metabolic heat production and delays core temperature decline; can also cause discomfort that fragments early sleep |
| Alcohol | Avoid in wind-down window entirely | Initial sedation is followed by stimulation as alcohol metabolizes; disrupts REM sleep architecture and increases nighttime waking |
On alcohol specifically: Harvard Health notes that while alcohol can make you feel sleepy initially, after a few hours it becomes stimulating, worsens snoring, and reduces REM sleep. It is not a wind-down aid — it is a sleep disruptor with a delayed onset.
When Your Mind Won't Quiet Down: Cognitive Offloading Techniques
For many adults, the barrier to sleep onset is not physical stimulation — it is a mind that keeps running through unfinished tasks, unsettled worries, or low-grade anxiety at the moment of trying to fall asleep. This is a distinct problem from physiological arousal, and it requires a different set of tools.
The cognitive vigilance loop works like this: the brain treats unresolved tasks and unclosed concerns as open files. At sleep onset, when external demands drop away, the brain resurfaces these open files to prevent them from being forgotten. The more you try to suppress the thoughts, the more prominent they become — a well-documented rebound effect.
Three techniques address this directly:
- Tomorrow's to-do list (T-30 minutes). As described in the countdown, writing a specific list of next-day tasks — not a diary entry, not problem-solving — externalizes the vigilance loop. The brain's rehearsal function quiets when it has a record to rely on instead. The key methodological detail from the Scullin et al. research: write concrete future tasks, not reflections on what happened today. The forward orientation is what produces the effect.
- Scheduled worry window (earlier in the evening, around T-90 to T-120). Set aside 15 to 20 minutes earlier in the evening to surface and write down worries, concerns, or unresolved items. The goal is not to solve them — it is to acknowledge them and assign a specific next step. This pre-empts the pillow as the default worry surface. If a worry surfaces at bedtime after you have already done this, you can remind yourself that it has been noted and scheduled.
- Physiological sigh (T-30 minutes or in bed if needed). A double nasal inhale — breathe in through the nose, then take a second short inhale on top of it to fully inflate the lungs — followed by a long, slow exhale through the mouth. This pattern rapidly activates the parasympathetic nervous system by maximizing lung inflation and then triggering the exhale-driven vagal response. It works faster than most deliberate breathing techniques because it addresses the mechanical state of the lungs directly.
"If we can switch off a sense of any threat that's mounted from the day, that will support our sleep." — Allison Harvey, professor and clinical psychologist, UC Berkeley, on the role of wind-down routines in reducing physiological and cognitive arousal before bed.
"This is not the time to check one last email or text with friends about exciting plans." — Allison Harvey, noting that emotionally arousing content — positive or negative — is equally activating in the wind-down window.
Building Consistency: How Repetition Trains Your Biology
A wind-down routine does not only work through its individual components. Over time, the sequence itself becomes a physiological signal.
When the same series of behaviors is repeated consistently before sleep, the brain begins to associate those behaviors with the physiological state of sleep onset — a Pavlovian conditioned response. A 2025 narrative review in Sleep Medicine Reviews by Meneo and Baglioni describes this mechanism directly: positive pre-sleep routines create conditioned learning where bed and bedroom cues, and routine behaviors, become associated with higher sleep propensity. Eventually, beginning the routine starts shifting physiology toward sleep before any individual component completes. The routine stops being something you do to feel sleepy and starts being something that makes you sleepy by virtue of its familiarity.
This conditioning effect takes time to develop — typically 2 to 4 weeks of consistent practice. In the early days, the routine works primarily through its direct physiological mechanisms (light reduction, temperature, breathwork). The conditioned response builds on top of that foundation with repetition.
Why Start Time Matters: The Forbidden Zone
One reason routines fail even when executed correctly is a mismatch between the routine's start time and the individual's circadian phase. The circadian system produces a period of low sleep propensity in the 1 to 4 hours before habitual sleep onset — sometimes called the wake maintenance zone or forbidden zone. For someone who habitually falls asleep around 11 PM, this zone runs roughly from 7 to 10 PM. Trying to fall asleep during this window — regardless of how relaxed you feel — will produce extended sleep onset because the circadian system is actively promoting wakefulness.
This is particularly relevant for people with delayed chronotypes, who have a naturally later melatonin onset. If your dim-light melatonin onset occurs at 11 PM rather than 9 PM, starting a wind-down routine at 8 PM and attempting sleep at 10 PM means trying to sleep during your forbidden zone — a mismatch that no amount of warm baths or journaling will fully overcome. The 2-hour countdown should be anchored to your own melatonin onset window, which varies by chronotype. The Chronotype Guide covers how to identify your chronotype and what it means for your optimal sleep timing.
When the Routine Is Not Enough
A well-executed wind-down routine is a meaningful behavioral intervention for lifestyle-driven sleep-onset difficulty. It is not a treatment for chronic insomnia.
If you are experiencing difficulty falling asleep three or more times per week for three or more months — and the difficulty is causing daytime impairment — that meets the clinical threshold for chronic insomnia disorder. At that level, behavioral hygiene improvements are supportive but insufficient on their own. The evidence-based first-line treatment endorsed by the American Academy of Sleep Medicine (AASM) and the American College of Physicians (ACP) is Cognitive Behavioral Therapy for Insomnia (CBT-I), which includes sleep restriction, stimulus control, and cognitive restructuring components specifically designed for conditioned arousal and sleep-related worry.
- Chronic insomnia (3+ nights/week, 3+ months, with daytime impairment): CBT-I is the appropriate first step, not an optimized wind-down routine.
- Rotating shift schedules: standard wind-down protocols address the pre-sleep window but not the underlying circadian disruption that shift work produces. The Shift Work Disorder article covers the additional management approaches relevant to that situation.
- Readers who also want to explore supplements alongside a behavioral routine may find the articles on L-theanine for sleep and valerian root for sleep useful as reference — though supplements are adjuncts to behavioral practice, not substitutes for it.
Supports these guides
Spot an error or have clinical feedback?
Because this article covers clinical, medication, or safety information, we use a moderated correction channel instead of open public comments. Let us know if something about “Evening Wind-Down Routine for Better Sleep: Evidence-Based Steps and Timing” needs a closer look.
Send feedback on this article