During a smoke event, sleep can fall apart even when bedtime has not changed. The bedroom is the same, the alarm is the same, and the usual sleep advice may technically still apply. But the day around sleep has changed: the air irritates the throat, windows stay shut, outdoor walks disappear, children or older relatives are kept inside, and the phone becomes an air-quality monitor before it becomes an alarm clock.
That mismatch matters because wildfire smoke and sleep problems are no longer a fringe concern for a few unlucky weeks. Climate modeling projects that wildfire-related PM2.5 pollution could rise by 55% under an RCP 4.5 scenario and by 190% under an RCP 8.5 scenario by the end of the century, compared with modeled baseline conditions.[1] Those projections do not tell any one household how many bad nights are coming this summer. They do explain why smoke-season sleep deserves more than a generic reminder to relax before bed.
Survey data also suggest that sleep disruption is a visible part of the smoke burden. In one Frontiers in Public Health study, more than 37% of smoke-exposed residents reported disrupted or poor sleep, with women and adults ages 25 to 54 disproportionately affected.[2] The caveat is important: the study had a 6.4% response rate to mailed invitations, so the figure should not be treated as a clean national prevalence estimate.[2] It is better read as a signal that sleep disruption is common enough to ask about directly, not as a private failure of bedtime discipline.
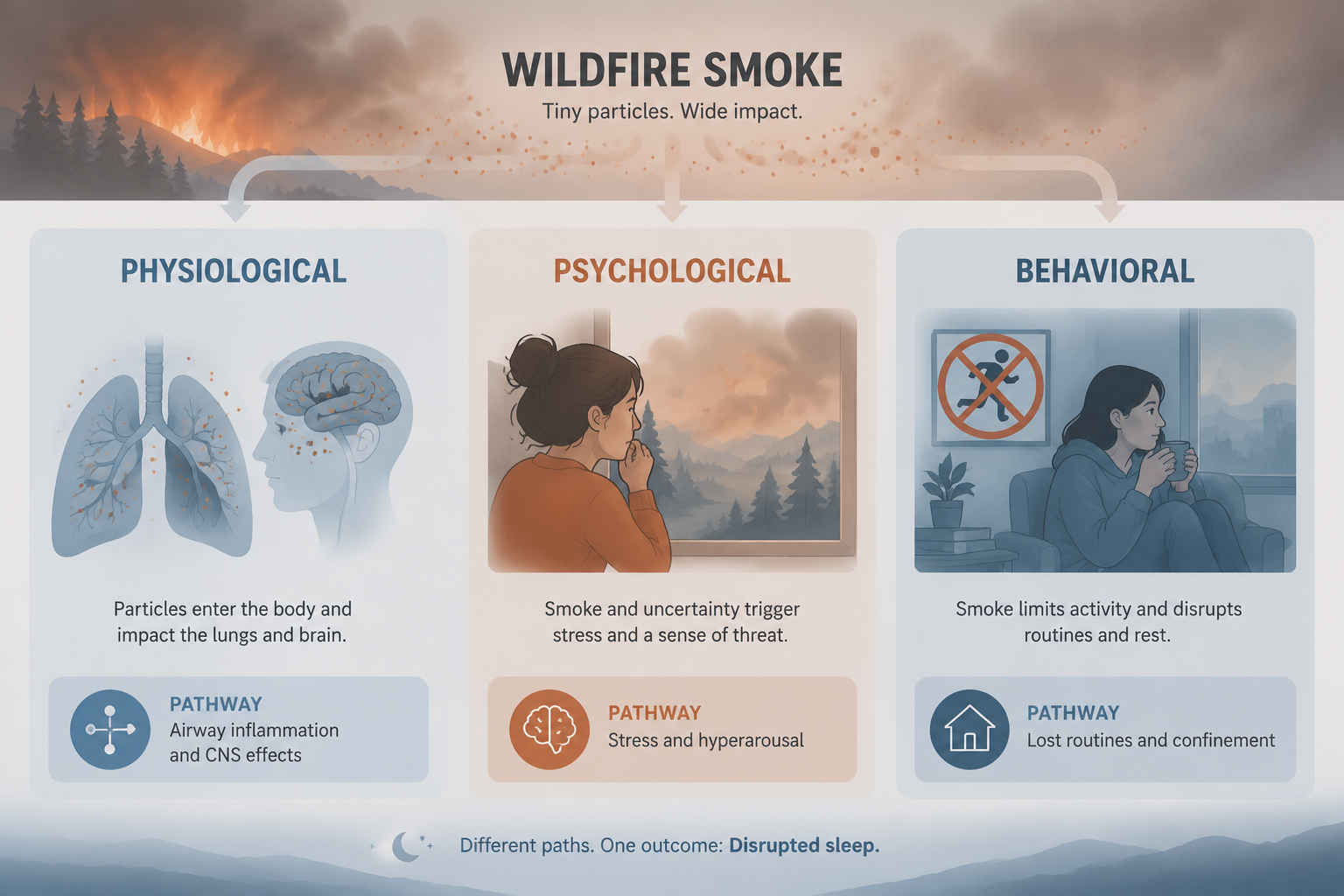
The useful way to think about smoke-season sleep is not as one problem with one fix. Wildfire smoke can disturb sleep through at least three interacting pathways: a physiological pathway involving airway irritation, inflammation, breathing discomfort, and possible central nervous system effects; a psychological pathway involving perceived threat and hyperarousal; and a behavioral pathway involving the loss of movement, daylight, and ordinary routines. Eisenman and Galway’s scoping review of wildfire smoke and health describes wildfire smoke effects as operating through multiple levels rather than through exposure alone, which fits what many households experience during prolonged smoke events: the particles matter, but so do the warnings, restrictions, and disrupted days around them.[3]
The Physiological Route: Irritated Airways, Inflammation, and Uneasy Breathing
The most direct pathway starts with PM2.5, the fine particulate matter in wildfire smoke. These particles are small enough to be inhaled deep into the lungs, where they can irritate airways and contribute to inflammation. At night, that does not have to become a dramatic asthma attack to matter. A scratchy throat, mild cough, chest tightness, nasal irritation, or the sense that breathing takes a little more effort can fragment sleep and make it harder to settle back down after normal awakenings.
This is one reason smoke-season insomnia can feel unfairly resistant to standard advice. A person may have dimmed the lights and avoided late caffeine, yet still be lying awake because the body is receiving irritation signals from the airway. If smoke has triggered coughing or congestion, the usual sleep-onset problem becomes a maintenance problem: sleep starts, breaks, restarts, and breaks again.
There is also mechanistic interest in whether smoke particles can affect brain systems involved in sleep and arousal. The Sleep Foundation summarizes evidence that wildfire smoke PM2.5 can infiltrate brain regions that regulate sleep, including the frontal cortex and cerebellum.[4] That does not prove that every smoky night directly disrupts human sleep through the brain. It does make the physiological pathway more plausible than a simple “the air smells bad, so people worry” explanation.
Animal research adds another cautious piece. In a 2023 Frontiers in Environmental Health study, rats were exposed to eucalyptus wood smoke at approximately 964 μg/m³, a very high concentration, and the researchers examined biological effects relevant to neuroinflammation and exposure response.[5] The study should stay in its lane: rats are not people, eucalyptus smoke under experimental conditions is not an ordinary bedroom, and direct translation to human sleep disruption would be too strong. Still, it supports a biologically plausible concern that smoke exposure can affect more than the nose and lungs.
For countermeasures, this pathway points first to exposure reduction, not willpower. Keep windows closed when outdoor air is poor, use appropriate filtration when available, run HVAC systems on recirculation if that is the safer setup for the home, and avoid bringing smoke indoors through evening activities that can wait. People with asthma, COPD, heart disease, pregnancy, or symptoms such as wheezing, chest pain, severe shortness of breath, or oxygen concerns should treat the situation as medical, not merely behavioral.
The Psychological Route: Smoke as a Threat Cue
Smoke is not just an air-quality measurement. It is also a sensory signal that something nearby, or not-so-nearby, is burning. The orange light, the smell in the hallway, the emergency alerts, and the map refreshes all tell the nervous system to stay watchful. That watchfulness can be useful at 4 p.m. when decisions need to be made. It is less useful at 2 a.m. when the body keeps scanning for updates.
A 2023 Sleep Medicine study of wildfire survivors gives this pathway particular weight: among trauma-related predictors, smoke exposure was reported as the strongest predictor of insomnia, surpassing property loss or evacuation.[6] That finding complicates a common assumption that only the most visibly catastrophic wildfire experiences “count” as trauma. For sleep, a person does not need to have lost a home for smoke to become a cue for danger, uncertainty, and vigilance.
This does not mean smoke exposure inevitably causes insomnia in every exposed person, or that all nighttime anxiety during smoke season is clinically traumatic. It means the threat pathway deserves to be taken seriously. When the air itself becomes the reminder, the bedroom can stop feeling like a sealed-off place and start feeling like another location inside the event.
Related mental-health evidence points in the same direction, though it should not be mistaken for direct sleep-outcome proof. A California study of the severe 2020 wildfire season found that each 10 μg/m³ increase in wildfire-specific PM2.5 was associated with a measurable increase in emergency department visits for depression, anxiety, and mood disorders within 7 days.[7] The study was limited to California from July through December 2020, during the state’s worst wildfire season on record, so it should not be generalized casually to every region or every smoke episode.[7] It does show that smoke exposure can coincide with short-term mental-health strain at a population level.
The practical response here is not to stop checking conditions altogether. Information matters. The goal is to put boundaries around threat monitoring so it does not become the last and first activity of the night. A better pattern is to choose a final evening check, make the necessary household decisions from that information, then stop refreshing unless an emergency alert requires action. If evacuation risk is part of the situation, prepare the essentials earlier in the evening; do not make the bed the place where planning finally begins.
The Behavioral Route: The Day Loses Its Anchors
The quieter pathway is behavioral. Smoke changes the day that sleep depends on. Outdoor exercise gets canceled. Morning light is filtered or avoided. Children stay inside and burn less energy. Adults skip walks, errands, commutes, and ordinary transitions. By evening, the body has had fewer timing cues and fewer chances to discharge restlessness.
Dodd and colleagues captured this in qualitative work on the “lost summer” experience of a record wildfire season, describing how prolonged smoke exposure disrupted outdoor physical activity and sunlight exposure, both of which help regulate circadian timing and sleep onset.[8] The phrase is useful because it names the cumulative pattern. One canceled walk is manageable. Weeks of indoor improvising can flatten the difference between morning, afternoon, and evening.
This pathway also explains why children and adults may be restless at night for different reasons inside the same home. A child may be under-tired from confinement and overstimulated by indoor substitutes. An adult may be both under-moved and over-alert after a day of checking alerts, moving air purifiers, and deciding whether the next day’s plans are safe. The family may call it a bedtime problem, but the bedtime is only where the disrupted day finally shows up.
| Pathway | What changes during smoke events | What the response should target |
|---|---|---|
| Physiological | Airway irritation, inflammation, coughing, congestion, breathing discomfort, and possible CNS effects | Cleaner indoor air, exposure reduction, symptom monitoring, and medical care when respiratory or cardiac symptoms warrant it |
| Psychological | Threat cues, alert checking, uncertainty, and nighttime hyperarousal | Bounded information habits, earlier planning, calming routines, and support when anxiety or trauma symptoms persist |
| Behavioral | Less daylight, less movement, indoor confinement, canceled routines, and blurred daily timing | Indoor movement, bright daytime light when safe, consistent meals, and a protected evening wind-down |
Why Generic Sleep Hygiene Often Feels Too Thin
Basic sleep hygiene still matters during smoke season. A consistent wake time, dimmer evening light, a cooler bedroom when possible, and a predictable wind-down routine are not suddenly irrelevant. If the whole routine has drifted, a fuller reset is better handled through a baseline guide such as Sleep Hygiene Fundamentals and an Evidence-Based Bedtime Routine.
But the usual checklist is incomplete if it ignores why the night changed. A person coughing from smoke does not primarily need a lecture about screens. A person lying awake after watching evacuation zones shift may need fewer late-night alerts and a clearer safety plan. A household that has spent five days indoors may need deliberate movement and daylight substitutes before it needs another lavender product.
For broader context on smoke itself, see Why Does Wildfire Smoke Disrupt Your Sleep?. For seasonal overlap, especially when hot nights and smoke arrive together, Summer Heat and Wildfire Smoke Create a Triple Threat to Sleep is the more specific companion piece.
Matching the Fix to the Pathway
When smoke is the trigger, the first question is not “What is the perfect bedtime rule?” It is “Which pathway is most active tonight?” The answer can change across the same week.
- If the body pathway is loud, prioritize indoor air. Close obvious leakage points when outdoor air is poor, use the best available filtration, avoid indoor particle sources, and treat respiratory or cardiac symptoms as health signals rather than sleep annoyances.
- If the threat pathway is loud, move planning earlier. Check reliable alerts at a set time, decide what would trigger action, prepare essentials if needed, then keep the phone out of the last part of the night unless emergency notifications are necessary.
- If the behavioral pathway is loud, rebuild the day indoors. Use safe indoor movement, bright daytime light where possible, regular meals, and a clear evening transition so the body still receives timing cues.
- If sleep stays disrupted after the smoke clears, treat that as a separate problem. Short-term smoke disruption can turn into conditioned insomnia when the bed becomes associated with wakefulness.
That last point is where ordinary insomnia care re-enters. If the sleep problem persists for weeks, becomes less tied to smoke conditions, or starts changing daytime functioning, CBT-I is the evidence-based treatment to understand. Supplements and home remedies may feel appealing during a bad stretch, but they should not be the first answer to a problem driven by air quality, hyperarousal, and disrupted routines; Which Home Remedies for Insomnia Actually Have Scientific Backing? is a better place to sort that out before adding products on top of an unaddressed exposure problem.
Wildfire smoke disrupts sleep because it changes the body, the threat environment, and the structure of the day at the same time. The most useful response is not to blame the sleeper or keep tightening one bedtime rule. It is to identify the pathway doing the most damage tonight and answer that pathway directly.
References
- Future Fire Impacts on Smoke Concentrations, Visibility, and Health in the Contiguous United States. GeoHealth. 2018. https://agupubs.onlinelibrary.wiley.com/doi/full/10.1029/2018GH000144
- Physical and Mental Health Effects of Bushfire and Smoke in the Australian Capital Territory 2019–20. Frontiers in Public Health. 2021. https://www.frontiersin.org/articles/10.3389/fpubh.2021.682402/full
- The mental health and well-being effects of wildfire smoke: a scoping review. BMC Public Health. 2022. https://pmc.ncbi.nlm.nih.gov/articles/PMC9724257/
- Wildfires and Sleep. Sleep Foundation. https://www.sleepfoundation.org/sleep-news/wildfires-and-sleep
- Wood smoke exposure and neuroinflammation in rats. Frontiers in Environmental Health. 2023. https://www.frontiersin.org/journals/environmental-health/articles/10.3389/fenvh.2023.1151669/full
- Trauma-related predictors of insomnia among wildfire survivors. Sleep Medicine. 2023. https://www.sciencedirect.com/journal/sleep-medicine
- Wildfire Smoke Exposure and Emergency Department Visits for Mental Health Conditions in California. JAMA Network Open. 2025. https://jamanetwork.com/journals/jamanetworkopen/
- Lived experience of a record wildfire season in the Northwest Territories, Canada. Canadian Journal of Public Health. 2018. https://link.springer.com/journal/41997
Comments
Join the discussion with an anonymous comment.