Why Generic Sleep Lists Fail (and What Works Instead)
If you have searched for "things to help you sleep," you have likely seen the same ten tips repeated across every article: dim the lights, avoid screens, keep your room cool, skip caffeine after noon. These are not wrong, but they are also not enough — because they treat every sleep problem as if it were the same problem.
A person who takes 90 minutes to fall asleep needs a different first-line intervention than someone who falls asleep easily but wakes at 3 a.m. and cannot get back to sleep. Someone whose mind races the moment the lights go out needs a different approach than someone who sleeps seven hours but wakes feeling like they have not rested at all. A one-size-fits-all list cannot serve all four of these people, yet that is what most articles deliver.
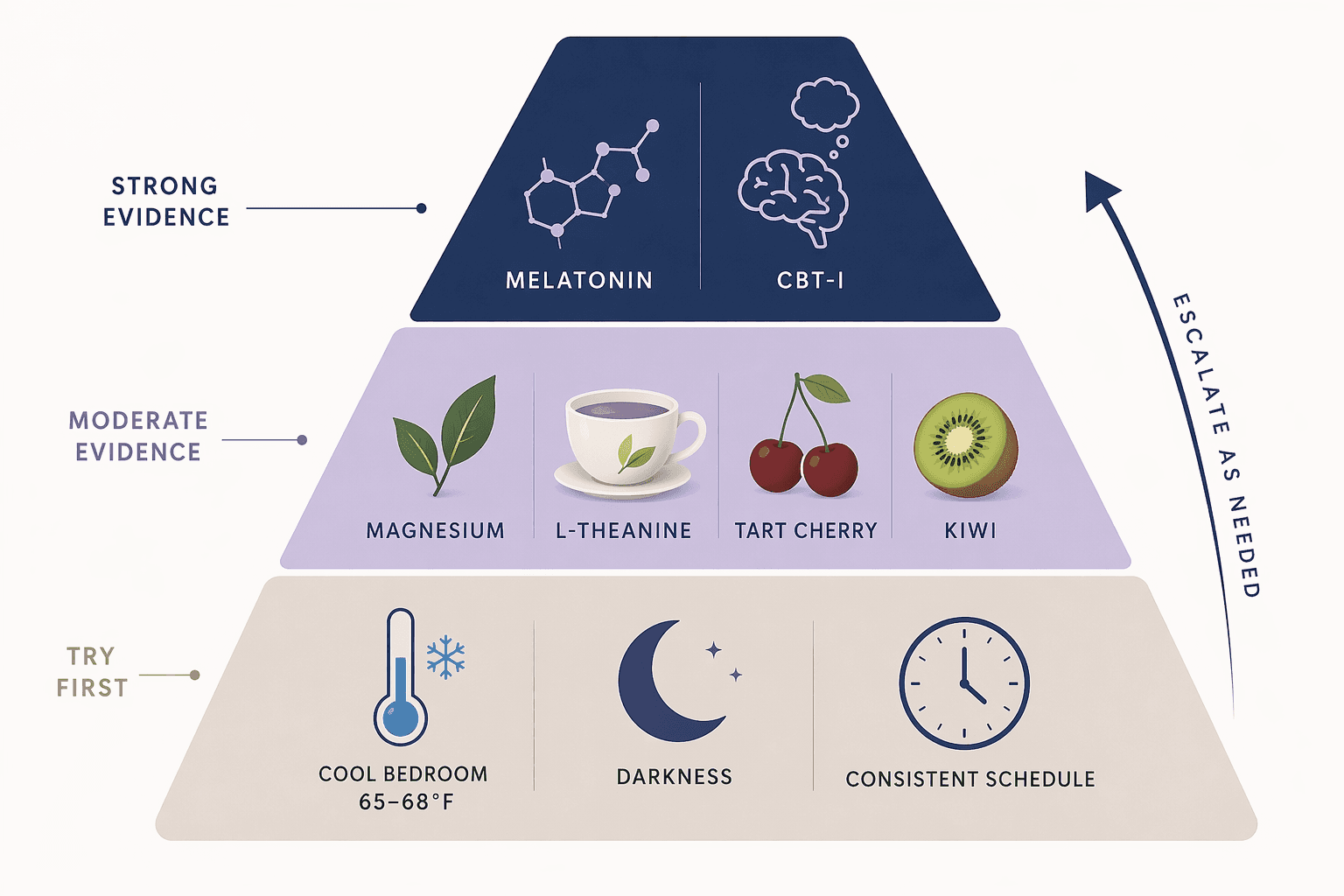
Research suggests that at least 10% of adults have chronic insomnia and another 20% experience it occasionally, according to a 2020 research review. That is a large and diverse group of people, and they do not all share the same root cause. The framework below replaces the generic list with a decision-first approach: identify your dominant sleep problem pattern, then try the interventions that match it.
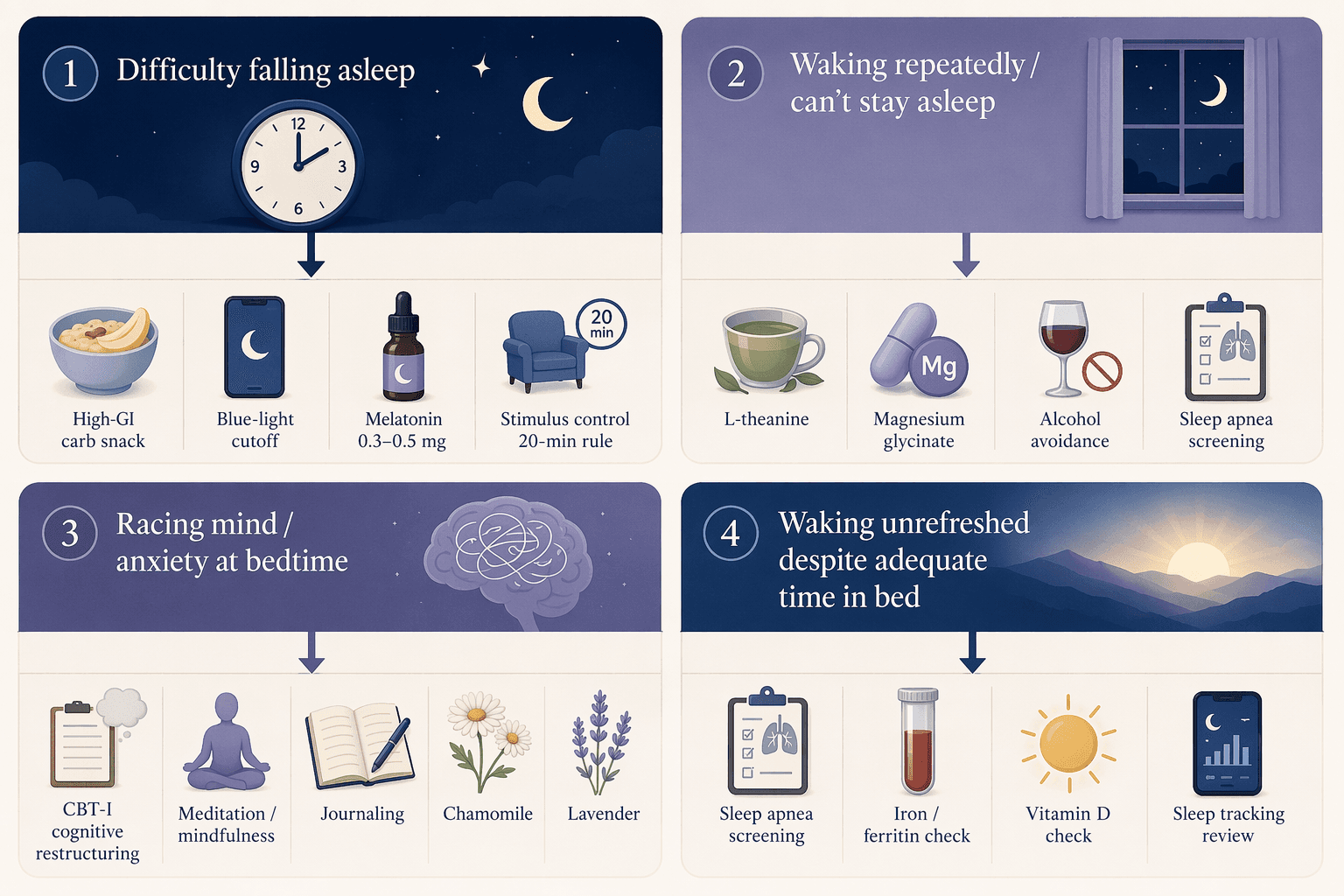
Problem Pattern 1: Difficulty Falling Asleep (Sleep-Onset Insomnia)
If you regularly lie in bed for more than 30 minutes before falling asleep, your brain has likely formed a conditioned association between your bed and wakefulness. The goal is to break that cycle and give your sleep drive the best possible chance to take over. Here is a prioritized ladder of interventions to try, starting with the least invasive.
First-Line Interventions for Sleep-Onset Insomnia
- Check your bedroom temperature. The ideal range is 65 to 68 degrees Fahrenheit, according to the Sleep Foundation. Johns Hopkins Medicine similarly recommends a thermostat setting between 65 and 72 degrees. A room that is too warm delays the core body temperature drop that signals your brain to initiate sleep.
- Apply the 20-minute stimulus control rule. If you have spent roughly 20 minutes in bed unable to sleep, get out of bed and do something relaxing in low light. Return to bed only when you feel sleepy again. This is a core component of CBT-I protocols and is recommended by the Sleep Foundation, the Mayo Clinic, and the National Council on Aging.
- Eliminate blue light exposure for at least 60 minutes before bed. Light from phones, laptops, and TVs prevents the natural release of melatonin, which the brain begins producing roughly four hours before natural sleepiness sets in, according to Johns Hopkins.
- Consider a high-glycemic-index carbohydrate snack four hours before bed. A 2007 study by Afaghi et al., summarized in a 2016 review by St-Onge et al., found that a high-GI meal reduced sleep-onset latency from 17.5 minutes to 9.0 minutes compared to a low-GI meal. This is not a large meal — a small bowl of white rice or a banana can suffice.
- Try low-dose melatonin (0.3 to 0.5 mg) taken two hours before your target bedtime. Melatonin supplements are available in doses ranging from 0.1 mg to 10 mg, but higher doses are not necessarily more effective and may cause next-day grogginess. Because melatonin is classified as a dietary supplement and is not FDA-regulated, Johns Hopkins advises sticking with a single trusted brand and avoiding unknown online sources.
Problem Pattern 2: Waking Up Repeatedly (Sleep-Maintenance Insomnia)
Falling asleep is not the issue — staying asleep is. You wake up multiple times during the night, or you wake up too early and cannot get back to sleep. Sleep-maintenance insomnia often has different root causes than sleep-onset insomnia, and the interventions reflect that.
First-Line Interventions for Sleep-Maintenance Insomnia
- Consider L-theanine 200 mg. Unlike melatonin, L-theanine does not appear to help people fall asleep, but it may enhance sleep quality by reducing the number of nighttime awakenings, making it suitable specifically for sleep-maintenance insomnia. Consuming up to 200 mg per day appears safe for most people, according to the Sleep Foundation.
- Try magnesium glycinate, particularly if you are over 65. Limited research suggests older adults with insomnia may benefit from magnesium supplements. A clinical trial cited by the Sleep Foundation found that a combination of melatonin, magnesium, and zinc helped older adults with insomnia sleep longer and more deeply.
- Eliminate alcohol within three hours of bedtime. Alcohol is a sedative that can help you fall asleep, but it disrupts sleep architecture during the second half of the night, leading to more frequent awakenings and less restorative sleep. Harvard Health notes that alcohol acts as a stimulant that disrupts sleep during the night.
- Conduct a noise and temperature audit. Even small environmental disruptions — a neighbor's dog, a partner's snoring, a room that warms up overnight — can cause micro-arousals that you do not consciously remember but that fragment your sleep. The ideal bedroom temperature remains 65 to 68 degrees throughout the night.
- Consider a sleep apnea screening if you snore loudly, have been told you stop breathing during sleep, or wake up gasping for air. Sleep apnea is a common underlying cause of sleep-maintenance insomnia and is often undiagnosed.
Problem Pattern 3: Racing Mind or Anxiety at Bedtime
Your body is tired, but your brain will not cooperate. Worries about work, relationships, or health loop on repeat the moment you lie down. This pattern is driven by a cortisol-melatonin conflict: stress activates fight-or-flight hormones that directly oppose the neurochemical signals needed for sleep onset.
First-Line Interventions for Racing Mind at Bedtime
- Use cognitive restructuring techniques from CBT-I. While stimulus control addresses conditioned arousal, cognitive restructuring targets the anxious thoughts themselves. This involves identifying catastrophic thinking about sleep ("If I do not fall asleep right now, tomorrow will be ruined") and replacing it with more balanced thoughts. CBT-I is the recommended first-line treatment for chronic insomnia per AASM guidelines, according to the Sleep Foundation.
- Write down your worries before bed. A brief journaling session — five to ten minutes — can offload circulating thoughts onto paper, reducing their ability to interrupt sleep. This is sometimes called a "brain dump" and is a simple cognitive intervention with low risk and no cost.
- Try chamomile tea. Johns Hopkins Medicine recommends warm milk, chamomile tea, and tart cherry juice for patients with sleep trouble. Chamomile contains apigenin, an antioxidant that binds to benzodiazepine receptors in the brain and may produce a mild sedative effect.
- Consider lavender. Aromatherapy with lavender essential oil has shown modest benefits for sleep quality in several small studies. It is not a standalone treatment, but it may help signal to your brain that it is time to wind down.
- Practice mindfulness or meditation. Even five minutes of focused breathing or body-scan meditation can shift the autonomic nervous system from sympathetic (fight-or-flight) to parasympathetic (rest-and-digest) mode, reducing the cortisol surge that keeps your mind racing.
Problem Pattern 4: Waking Unrefreshed Despite Adequate Sleep Time
You get seven or eight hours of sleep, but you wake up feeling as though you have not slept at all. This pattern is the most likely to have an underlying medical cause, and self-management alone is often insufficient. The priority here shifts from behavioral tweaks to screening for conditions that fragment sleep architecture without causing full awakenings.
First-Line Interventions for Unrefreshing Sleep
- Screen for sleep apnea. A 2023 review suggests that approximately 33.9% of men and 17.4% of women in the US have sleep apnea. The STOP-BANG questionnaire is a validated screening tool you can complete in under two minutes. If you score three or higher, a formal sleep study may be warranted.
- Check your iron and ferritin levels. Restless legs syndrome (RLS) is a common cause of unrefreshing sleep, and low iron stores are a treatable contributor to RLS symptoms. A simple blood test can determine whether supplementation is appropriate.
- Check your vitamin D levels. Vitamin D deficiency has been associated with poor sleep quality in multiple observational studies. While the mechanism is not fully understood, correcting a deficiency is a low-risk intervention that may improve sleep quality.
- Review your sleep tracking data. If you use a wearable device, look for patterns: frequent nighttime movement, low HRV, or a high proportion of light sleep relative to deep sleep. While consumer wearables are not clinical-grade diagnostics, they can provide useful clues about whether your sleep is fragmented in ways you do not consciously perceive.
When to Escalate: Signs You Need a Sleep Specialist
Self-management is appropriate for many sleep problems, but there are clear boundaries. The following criteria indicate that professional evaluation is warranted rather than continued self-experimentation.
- Chronic insomnia: difficulty falling asleep, staying asleep, or waking too early that occurs at least three nights per week for three months or longer, accompanied by daytime impairment such as fatigue, mood disturbance, or cognitive difficulty.
- Suspected sleep apnea: loud snoring, witnessed pauses in breathing during sleep, gasping or choking sounds, excessive daytime sleepiness despite adequate sleep time, or a STOP-BANG score of three or higher.
- Persistent unrefreshing sleep: sleeping seven or more hours per night but waking feeling exhausted, with no obvious environmental cause, for more than one month.
- Restless legs syndrome: an irresistible urge to move the legs, especially in the evening or at night, that interferes with sleep onset or maintenance.
Quick-Reference Decision Table: Match Your Problem to Your First Step
The table below summarizes the four problem patterns and their top two to three prioritized first-line interventions. Use it as a starting point, then refer to the detailed sections above for implementation guidance.
| Problem Pattern | Key Signs | Top 2-3 First-Line Interventions |
|---|---|---|
| Difficulty falling asleep | >30 min to fall asleep; mind may be quiet but sleep does not come | 1. 20-minute stimulus control rule 2. Bedroom temp 65-68°F 3. Low-dose melatonin (0.3-0.5 mg) |
| Waking up repeatedly | Falls asleep easily but wakes 2+ times per night or too early | 1. L-theanine 200 mg 2. Alcohol avoidance 3. Sleep apnea screening if snoring |
| Racing mind / anxiety | Body tired, but anxious thoughts prevent sleep onset | 1. Cognitive restructuring (CBT-I) 2. Journaling before bed 3. Chamomile tea or lavender |
| Waking unrefreshed | 7+ hours of sleep but feels exhausted upon waking | 1. Sleep apnea screening (STOP-BANG) 2. Iron/ferritin check 3. Vitamin D check |
Comments
Join the discussion with an anonymous comment.