
The Paradox of Nighttime Anxiety: Why Your Body Feels Alert When It Should Be Resting
You lie down after a long day. Your body is tired. Your eyes are heavy. But instead of drifting off, your mind starts racing. Your heart thumps a little harder. A worry you pushed aside at 3 p.m. now feels urgent and inescapable. If this scenario sounds familiar, you are not alone — and the cause is not simply that you are "too stressed to sleep."
A 2024 survey from the American Academy of Sleep Medicine found that 68% of Americans report losing sleep due to anxiety, and 74% report disrupted sleep due to stress. Those numbers are striking, but they raise a deeper question: why does anxiety specifically spike at night, when the body is biologically programmed to power down?
The answer lies in a circadian conflict — a tug-of-war between two hormones that are supposed to trade places at night. When that handoff fails, the result is not just poor sleep. It is a physiological state that actively generates the symptoms of anxiety, right when you need calm most.
The Healthy Circadian Handoff: How Cortisol and Melatonin Normally Trade Places
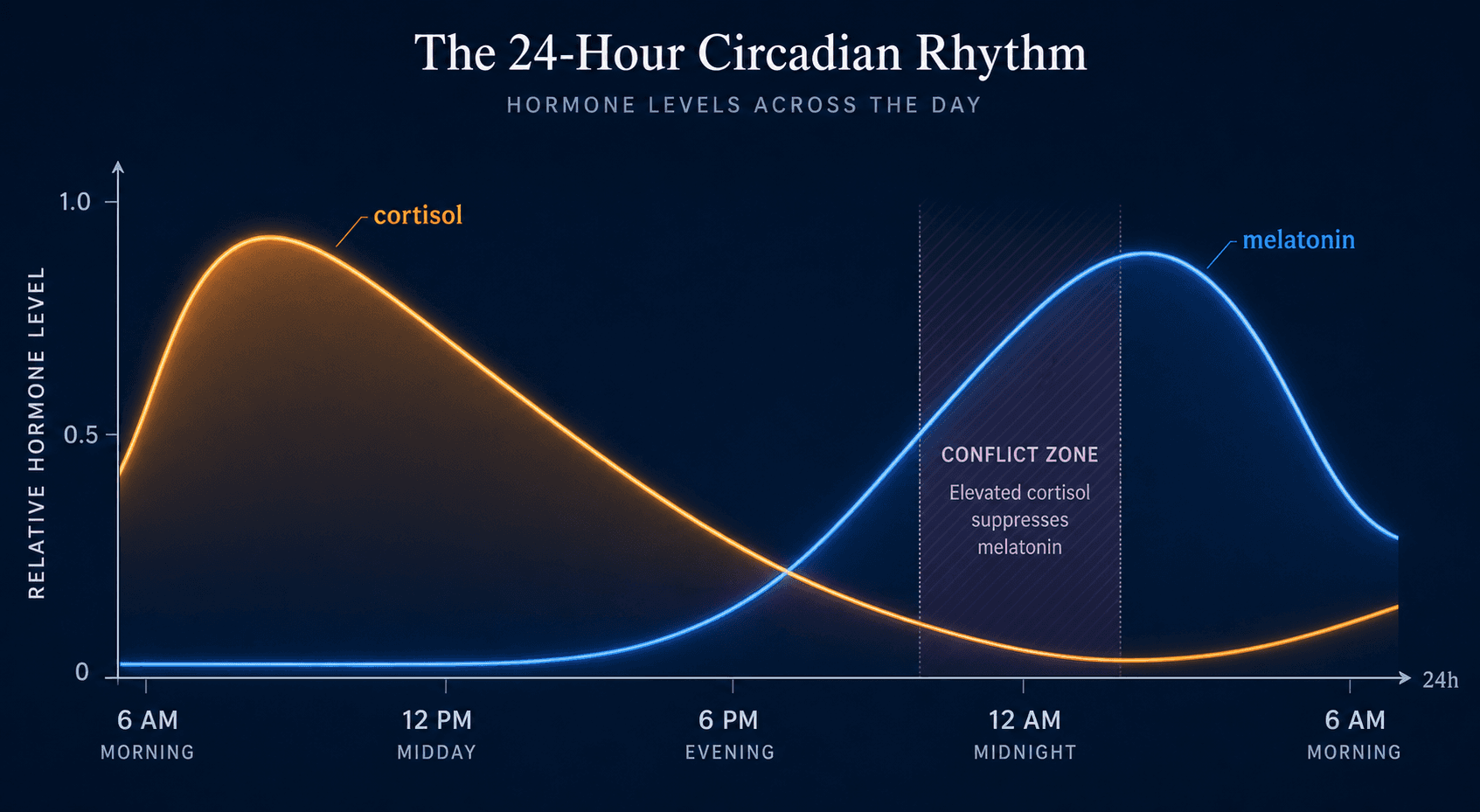
In a well-regulated system, cortisol and melatonin follow opposite schedules. Cortisol — often called the stress hormone, though its role is broader — begins rising in the early morning hours, peaking around 8–9 a.m. to help you wake up. It then declines through the afternoon and reaches its lowest point, or nadir, around midnight.
Melatonin follows the reverse arc. Production ramps up in the evening as light fades, peaks in the middle of the night, and drops off before morning. This is not a coincidence — the two hormones are mutually inhibitory. Cortisol suppresses melatonin release, and melatonin, in turn, helps dampen cortisol production.
This coordinated handoff is orchestrated by the suprachiasmatic nucleus (SCN) — the brain's master clock — and the hypothalamic-pituitary-adrenal (HPA) axis. When functioning correctly, the system ensures that by the time you are ready for bed, cortisol is low, melatonin is high, and your body is in a physiological state permissive to sleep.
For a deeper look at how the body clock regulates this process, see our guide on circadian rhythm mechanisms.
When the Handoff Fails: HPA Axis Dysregulation and Elevated Nighttime Cortisol
Chronic stress and hyperarousal change the HPA axis. Instead of following its natural decline, cortisol stays elevated into the evening. This is not a subtle shift — studies consistently show that people with anxiety disorders have higher nighttime cortisol levels compared to controls, and they also exhibit higher sleep reactivity, meaning their sleep is more easily disrupted by stress.
The consequence is direct: elevated cortisol in the evening suppresses melatonin production. With less melatonin available, the signal to transition into sleep is weakened. The body remains in a state of low-grade physiological alertness — heart rate slightly elevated, blood pressure not fully dipping, sympathetic nervous system activity persisting into the night.
This is the core mechanism that differentiates nighttime anxiety from general anxiety. It is not that your worries suddenly become more valid at 11 p.m. It is that the biological system that should be powering down is still running in daytime mode, and your brain interprets that physiological activation as a threat signal.
Why the Quiet Bedroom Amplifies Internal Threat Signals
The physiological disruption alone would be enough to disturb sleep, but there is a second layer: the psychological amplification that happens when the brain loses daytime distractions.
During the day, your attention is pulled outward — work tasks, conversations, traffic, screens. These external inputs occupy working memory and leave less capacity for internal worry. At night, in a quiet, dark bedroom, those external inputs disappear. The brain, now free from distraction, turns its attention inward.
The Sleep Foundation describes this as a state of mental hyperarousal, identified as a key factor behind insomnia. When you are already physiologically alert due to elevated cortisol, and you have no external stimuli to occupy your attention, the brain fixates on internal sensations: the racing heart, the shallow breathing, the worry that loops without resolution.
Research supports this: people with higher anxiety levels spend less time in both REM sleep and slow-wave (deep) sleep. These are the stages most critical for emotional processing and physical restoration. When you lose them, you do not just feel tired the next day — you also lose the overnight emotional regulation that REM sleep normally provides, making you more reactive to stress the following evening.
The Physiological Cascade: From Elevated Cortisol to Fragmented Sleep to Next-Day Anxiety
The relationship between nighttime anxiety and sleep disruption is not a simple correlation — it is a bidirectional cascade with a clear physiological engine.
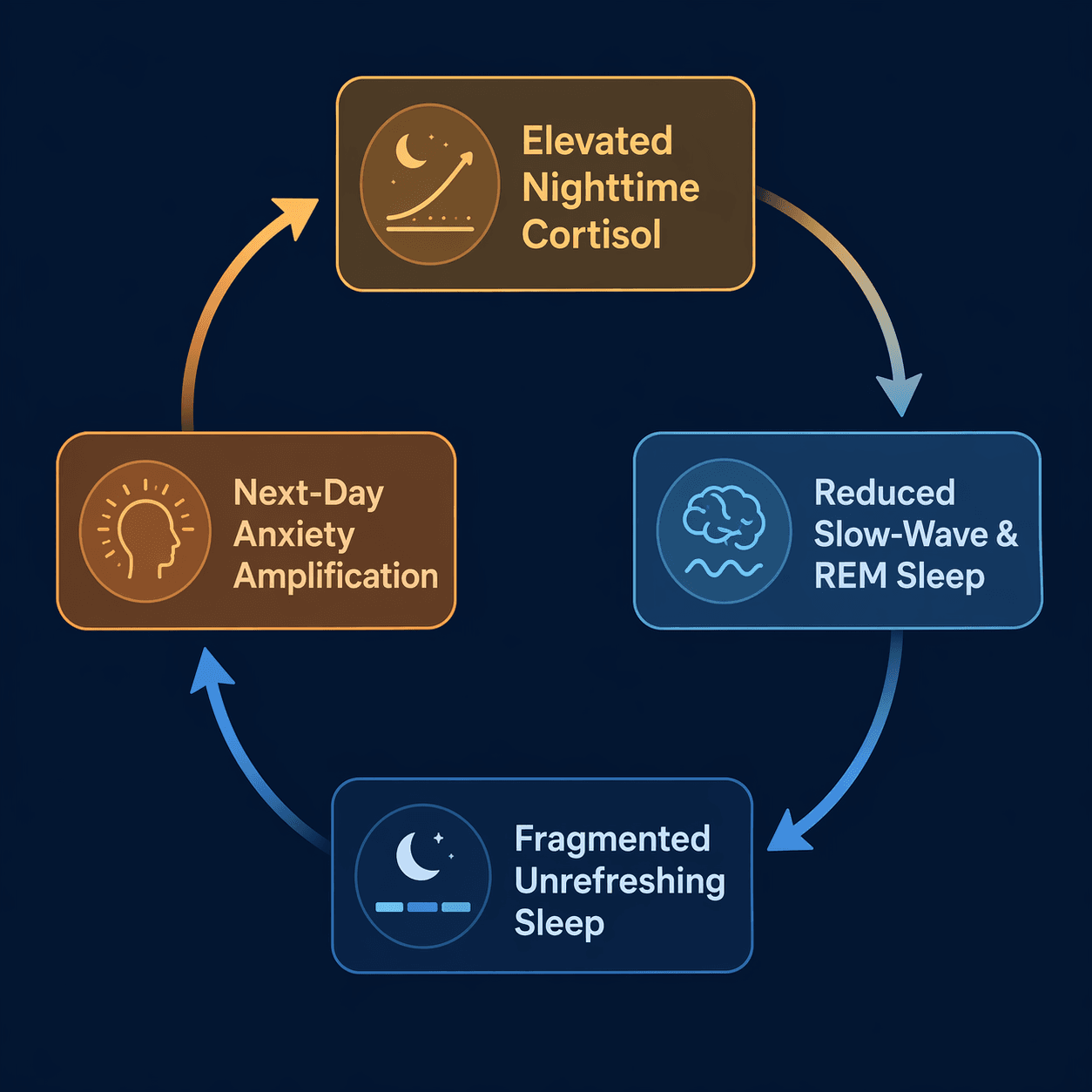
Here is how the cascade unfolds:
- Elevated nighttime cortisol suppresses melatonin and keeps the sympathetic nervous system active.
- This reduces time spent in slow-wave sleep (deep sleep) and REM sleep — the two most restorative stages.
- Shallow, fragmented sleep leads to more frequent nighttime awakenings, often accompanied by a racing heart or sense of dread.
- Unrefreshing sleep leaves the next day's emotional regulation systems compromised. The amygdala becomes more reactive; the prefrontal cortex has less capacity to dampen fear responses.
- Heightened daytime anxiety further dysregulates the HPA axis, ensuring that cortisol stays elevated again the following evening.
This loop is the reason why "just relax" advice so often fails. The system is locked in a self-reinforcing cycle where the cause (elevated cortisol) and the consequence (poor sleep) feed each other. Breaking the loop requires targeting the mechanism, not just the symptoms.
Is It General Nighttime Anxiety, Nocturnal Panic, or Something Else?
Not all nighttime anxiety episodes are the same. Differentiating between common nighttime anxiety, nocturnal panic attacks, and sleep apnea-related awakenings matters because the treatment paths are different.
Nocturnal panic attacks are a distinct phenomenon. A 2013 study by Nakamura et al. published in the Journal of Clinical Sleep Medicine compared 101 untreated panic disorder patients and found that those with primary nocturnal panic (attacks occurring mainly during sleep) had a distinct profile: 80% reported attacks in the first tertile of the night, during delta (slow-wave) sleep, and the hallmark symptom was a choking sensation. The study suggests primary nocturnal panic may be a relatively mild subcategory that responds well to treatment.
| Feature | General Nighttime Anxiety | Nocturnal Panic Attack | Sleep Apnea Awakening |
|---|---|---|---|
| Timing | Evening, while trying to fall asleep | First tertile of sleep (first 2–3 hours) | Throughout the night, often in REM |
| Onset | Gradual, builds as distractions fade | Abrupt, wakes you from sleep | Gradual or abrupt, often with gasping |
| Key sensation | Worry, racing thoughts, muscle tension | Intense fear, choking sensation, sense of doom | Gasping, choking, chest pressure, snoring history |
| Heart rate | Elevated but not extreme | Rapid, pounding | May spike upon awakening |
| Duration | Minutes to hours (keeps you awake) | 3–10 minutes, then returns to sleep | Brief, may happen multiple times per night |
| Prevalence | Very common in anxiety disorders | Up to 71% of people with panic disorder experience at least one; 18–45% have recurring episodes | Varies by population; more common in men and older adults |
The Nakamura et al. study was conducted at a sleep center in Japan and may have referral bias (e.g., more males with sleep-related concerns). Replication in broader populations is needed. However, the clinical distinction between nocturnal panic and sleep apnea is well-established across multiple studies and is not dependent on a single source.
Evidence-Based Interventions That Target the Mechanism
Because the root cause is circadian and physiological, the most effective interventions are those that directly address the HPA axis dysregulation and the conditioned arousal around the bed. Generic sleep hygiene — avoid caffeine, keep the room cool — is not enough for this presentation.
The following interventions are supported by clinical evidence and target the mechanism rather than just the symptoms:
- CBT-I (Cognitive Behavioral Therapy for Insomnia): This is the first-line treatment for chronic insomnia, including insomnia driven by anxiety. When used as a multicomponent protocol — combining stimulus control, sleep restriction, cognitive restructuring, and relaxation training — CBT-I improves insomnia symptoms in 70% to 80% of patients with primary insomnia, according to the Sleep Foundation. The American College of Physicians recommends all adult patients receive CBT-I as a first-line approach. For the comorbid anxiety-insomnia presentation, see our guide on CBT-I for comorbid insomnia.
- Stimulus Control Therapy: This is the component of CBT-I that directly targets the conditioned arousal between the bed and alertness. The goal is to break the association your brain has formed between the bedroom and wakefulness. For a detailed breakdown of each rule and the conditioning logic behind it, see our stimulus control therapy guide.
- Breath Retraining and Vagal Activation: Slow, extended exhalation (e.g., 4-7-8 breathing or box breathing) activates the vagus nerve, which triggers the parasympathetic nervous system and lowers cortisol. This is not a relaxation gimmick — it directly counteracts the sympathetic dominance caused by elevated nighttime cortisol.
- Timed Light Exposure for Circadian Reset: Morning bright light exposure (within 30–60 minutes of waking) helps reset the SCN and strengthen the cortisol-melatonin rhythm. Evening light avoidance (dimming lights, using blue-light filters 1–2 hours before bed) prevents melatonin suppression. For readers interested in melatonin supplementation as part of a circadian reset strategy, see our melatonin dosage guide.
- SSRI or SNRI as an Adjunct: For patients whose nighttime anxiety is part of a broader anxiety disorder, selective serotonin reuptake inhibitors (SSRIs) can reduce the underlying hyperarousal. The 2026 AASM guideline update provides specific recommendations on when medication is appropriate as an adjunct to CBT-I. See our FAQ on CBT-I vs. medication vs. combination therapy for the latest guidance.
Breaking the Cycle: How Restoring Sleep Disrupts Anxiety Escalation
The bidirectional loop between nighttime anxiety and poor sleep can feel inescapable, but the mechanism itself points toward a hopeful conclusion: because the cycle is driven by a measurable physiological conflict — elevated cortisol suppressing melatonin and fragmenting sleep — interventions that restore sleep architecture also reduce anxiety.
When CBT-I or stimulus control therapy successfully reduces sleep latency and consolidates sleep, the next-day effects are not just about feeling less tired. Restored REM sleep improves emotional regulation. Restored slow-wave sleep lowers baseline sympathetic activity. The HPA axis begins to re-regulate, and cortisol starts following its natural rhythm again.
This is why the first step is not trying harder to relax. The first step is understanding that the conflict is circadian and physiological — and that the right interventions target the mechanism, not the symptom. For a broader overview of the anxiety-insomnia relationship and treatment pathways, see our companion article on sleep anxiety and insomnia.
The quiet bedroom does not have to be a place of dread. When the cortisol-melatonin handoff is restored, the same environment that once amplified internal threat signals becomes what it was always meant to be: a space for the body to power down and recover.





Comments
Join the discussion with an anonymous comment.