Mechanism explainer
CBT-I: A Complete Protocol Guide to Cognitive Behavioral Therapy for Insomnia
A mechanistically grounded walkthrough of the full CBT-I protocol for adults with chronic insomnia — covering all five components, the sleep efficiency titration rules, and a week-by-week breakdown of what to expect and why the treatment feels harder before it improves.

What CBT-I Is and Why It Is the First-Line Treatment
Cognitive Behavioral Therapy for Insomnia (CBT-I) is a structured, multicomponent behavioral protocol that directly targets the psychological and physiological mechanisms sustaining chronic insomnia. It is not a relaxation technique, a sleep hygiene checklist, or a mindfulness program. It is a clinical protocol with a defined structure, specific rules, titration logic, and a documented success rate of 70–80% in adults with primary chronic insomnia.
The American Academy of Sleep Medicine (AASM) issued a strong recommendation for CBT-I in its 2021 clinical practice guideline — the highest evidence level the AASM assigns, meaning clinicians should follow it under most circumstances. The American College of Physicians independently recommends CBT-I as the first-line treatment for all adults with chronic insomnia.
In April 2026, the AASM went further. A new guideline published in the Journal of Clinical Sleep Medicine issued two conditional recommendations on combination therapy. First, it suggests combining CBT-I with medication over using medication alone. Second — and more consequentially for clinical practice — it suggests against combining CBT-I with medication rather than using CBT-I alone, noting that behavioral-psychological treatment by itself typically produces meaningful and durable improvements without the added risks of pharmacotherapy.
"Our analysis suggests that CBT-I by itself is the most efficacious first-line treatment for insomnia." — Dr. Daniel J. Buysse, lead author of the April 2026 AASM combination treatment guideline
The hierarchy the AASM now endorses is unambiguous: CBT-I alone first, combination therapy second, medication alone last. This matters because the most common clinical practice for decades has been to prescribe sleep medication while recommending behavioral changes — a sequence the evidence no longer supports as optimal.
Why does CBT-I outperform medication over time? Sleep medications suppress symptoms while the underlying mechanisms remain intact. CBT-I dismantles those mechanisms. Improvements from CBT-I persist and often increase after treatment ends — a pattern that is the opposite of medication, which produces rebound insomnia on discontinuation.
Why Chronic Insomnia Persists: The Spielman 3P Model
Most people who develop chronic insomnia can identify a triggering event — a stressful period at work, a health scare, a loss. What they cannot explain is why the insomnia continues long after that trigger has resolved. The Spielman 3P model provides the answer, and understanding it is the foundation for understanding why CBT-I works.
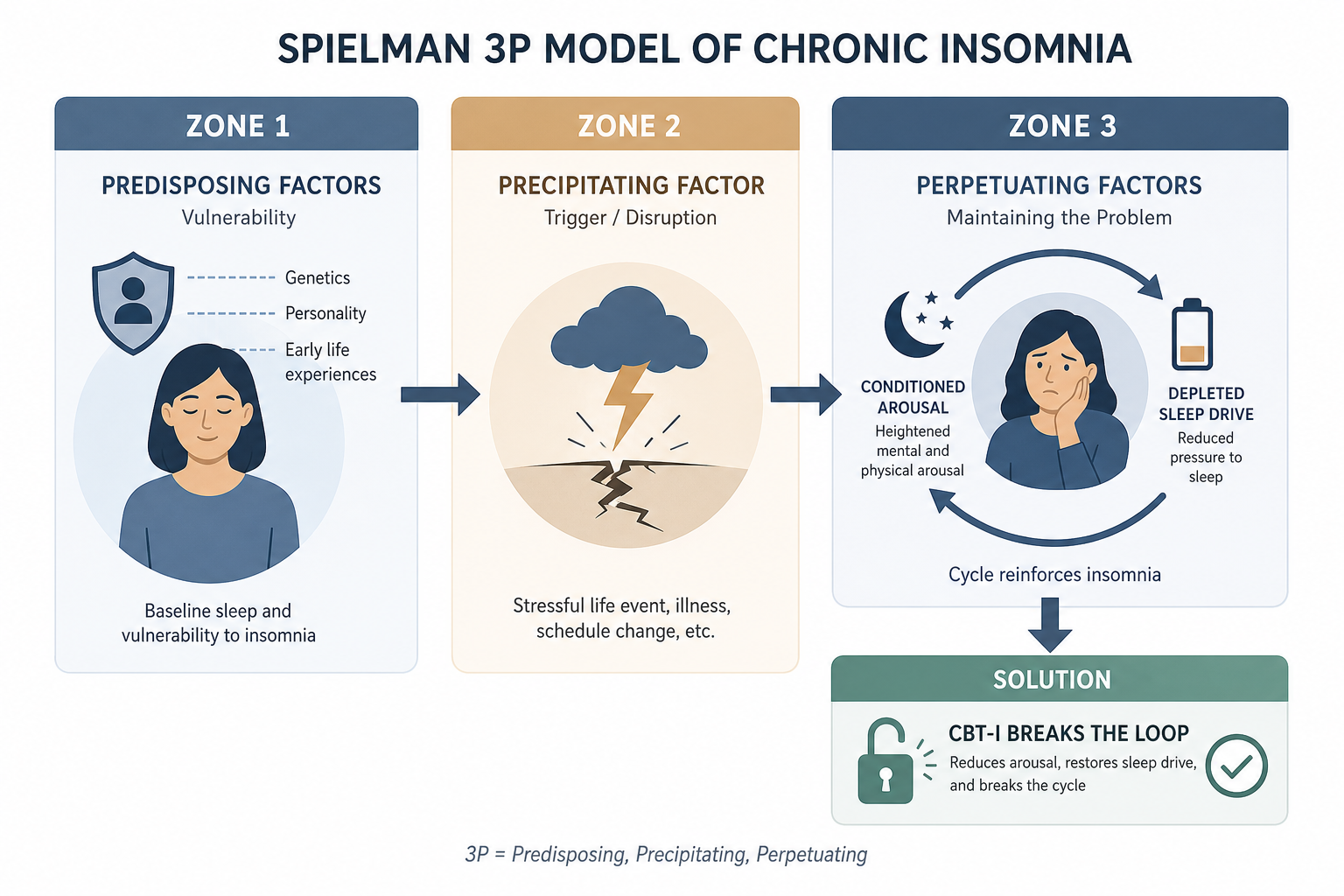
The three Ps are:
- Predisposing factors — Baseline characteristics that increase vulnerability to insomnia: a naturally elevated arousal system, anxiety traits, hyperreactivity to stress. These do not cause insomnia on their own, but they lower the threshold.
- Precipitating factors — The event that pushes sleep over the threshold: a job loss, a medical diagnosis, a relationship breakdown, a new baby. Acute insomnia begins here.
- Perpetuating factors — The behaviors and cognitions that keep insomnia going after the precipitating event has passed: spending more time in bed trying to recover lost sleep, napping, avoiding activities due to fatigue, and developing anxious, hypervigilant attention to sleep. These are what CBT-I targets.
Research by Ellis and colleagues published in 2021 empirically supports this framework. Higher levels of dysfunctional beliefs about sleep and affective sleep preoccupation at baseline significantly predicted whether acute insomnia would persist rather than remit — adding direct evidence that the cognitive and behavioral perpetuating factors are the critical drivers of chronicity, not the original stressor.
This has a direct implication for treatment: there is no point in searching for or treating the original trigger. The work is to dismantle what is maintaining the insomnia now. CBT-I does this through five interlocking components, each targeting a different perpetuating mechanism.
The Sleep Diary: Your Baseline and Decision Tool
Before any CBT-I component begins, you need one to two weeks of sleep diary data. The diary is not a journaling exercise — it is the quantitative input that drives every titration decision in the protocol. Without it, sleep restriction cannot be calibrated correctly.
Each morning, within 30 minutes of waking, record the following from the previous night:
| Diary Field | What It Captures | Why It Matters |
|---|---|---|
| Time to bed (TIB start) | When you got into bed with the intention to sleep | Determines total time in bed |
| Sleep onset latency (SOL) | How long it took to fall asleep after lights out | Key insomnia symptom; drives efficiency calculation |
| Number of awakenings | How many times you woke during the night | Tracks sleep consolidation over weeks |
| Wake after sleep onset (WASO) | Total minutes awake during the night (excluding SOL) | Second major driver of efficiency |
| Final wake time | When you woke for the last time | Establishes the fixed morning anchor |
| Total sleep time (TST) | Estimated total minutes actually asleep | The numerator in the efficiency formula |
| Time out of bed (TIB end) | When you got out of bed for the day | Determines total time in bed denominator |
From these fields, you calculate sleep efficiency (SE) using a single formula:
A note on wearables: fitness trackers and sleep rings do not replace the diary. Consumer devices estimate sleep stages using movement and heart rate algorithms, and their accuracy against polysomnography varies considerably across devices and individuals. More importantly, subjective sleep perception has independent clinical significance — how rested you feel, not just how long a sensor says you slept, is a valid clinical outcome. The diary captures what matters for CBT-I titration.
Component 1: Sleep Restriction Therapy
Sleep restriction therapy is the most powerful and most counterintuitive component of CBT-I. It is also the one most likely to be abandoned prematurely — which is why understanding the mechanism is not optional.
The Mechanism: Adenosine and Homeostatic Sleep Drive
Sleep pressure is regulated by adenosine, a metabolic byproduct that accumulates in the brain during wakefulness and is cleared during sleep. The longer you are awake, the more adenosine builds, and the stronger the drive to sleep becomes. This is the homeostatic sleep system.
People with chronic insomnia typically spend far more time in bed than they are actually sleeping — often 8, 9, or 10 hours in bed for 5 or 6 hours of fragmented sleep. This dissipates adenosine through light dozing, dilutes sleep pressure across too many hours, and produces shallow, fragmented sleep rather than deep consolidated sleep. To understand how sleep architecture is affected, the NREM and REM sleep stages explainer covers why sleep quality — particularly slow-wave depth — improves before total duration does.
Sleep restriction deliberately limits time in bed to match actual sleep time, forcing adenosine to accumulate to a high level before the sleep window opens. The result: when you do get into bed, you fall asleep faster, stay asleep longer, and sleep more deeply. Once this consolidation is established, the window is gradually expanded.
Setting the Initial Sleep Window
Using your diary average from the baseline week, calculate your mean total sleep time. This becomes your initial prescribed time in bed — with a minimum floor of 5.5 hours regardless of how little you report sleeping. Going below this floor risks excessive daytime impairment.
The sleep window is anchored by a fixed morning wake time that does not change, regardless of how the night went. This is the non-negotiable circadian anchor. The bedtime is calculated backward from the wake time. If your average TST is 5.5 hours and your fixed wake time is 6:30 AM, your prescribed bedtime is 1:00 AM.
The Titration Rules: When to Expand, Hold, or Contract
After the first week on the restricted window, you calculate your sleep efficiency from the diary. The result determines what happens next:
| Sleep Efficiency | Action | Window Change |
|---|---|---|
| ≥ 85% | Expand the sleep window | Add 15–30 minutes to bedtime (go to bed earlier) |
| 80–84% | Hold the current window | No change this week |
| < 80% | Contract the sleep window | Reduce time in bed by 15–30 minutes |
This is not a one-time decision. You apply these rules weekly throughout the protocol. Sleep efficiency is the compass. When efficiency is high, the window earns expansion. When efficiency drops, the window contracts to rebuild pressure. The goal is a sleep window that produces consistently efficient, consolidated sleep — then gradual expansion toward a duration that leaves you rested.
Contraindications for Sleep Restriction
Component 2: Stimulus Control Therapy
If sleep restriction targets the homeostatic (adenosine) side of insomnia, stimulus control targets the conditioned arousal side. Together, they address the two core perpetuating mechanisms that the Spielman model identifies.
The Conditioned Arousal Problem
Through repeated pairing of the bed environment with wakefulness, anxiety, and frustrated sleep effort, the bedroom becomes a conditioned stimulus for arousal rather than sleep. This is a Pavlovian association — the same mechanism by which Pavlov's dogs salivated at a bell. For someone with chronic insomnia, getting into bed reliably triggers the opposite of what is needed: a spike in alertness, racing thoughts, and physiological activation.
Stimulus control systematically extinguishes this association by eliminating all wakefulness-paired behaviors from the bed and bedroom, and by enforcing a strict behavioral boundary between the bed and sleep.
The Six Core Stimulus Control Rules
- Use the bed only for sleep and sex. No reading, no screens, no eating, no working, no lying awake watching television. Every non-sleep activity in bed strengthens the arousal association.
- Get out of bed if you cannot fall asleep within approximately 15–20 minutes. Do not watch the clock to time this precisely — use a rough subjective sense. Go to another room and do something quiet and unstimulating until you feel genuinely sleepy, then return to bed. This is the most counterintuitive rule and the most important one.
- Wake at the same time every morning, seven days a week. Including weekends. Sleeping in on weekends shifts the circadian phase and undermines the adenosine pressure built during the week. Consistency is the mechanism.
- Do not nap. Naps dissipate adenosine during the day, reducing the sleep pressure available at bedtime. They are not counted in TST for titration purposes. Even brief naps blunt the homeostatic drive that makes the restricted sleep window work.
- Do not go to bed until you are sleepy. Drowsiness — not tiredness or fatigue — is the signal. Going to bed before your prescribed time because you feel exhausted re-exposes the bed to wakefulness and undermines both components simultaneously.
- Remove or cover clocks in the bedroom. Clock-watching during the night is a hypervigilance behavior that maintains arousal and catastrophizing. Not knowing the exact time reduces the cognitive fuel for anxious sleep calculation.
Component 3: Cognitive Restructuring
The behavioral components of CBT-I address what you do. Cognitive restructuring addresses what you think — specifically, the dysfunctional beliefs about sleep that maintain anxiety, hypervigilance, and sleep effort.
The Four Categories of Dysfunctional Sleep Beliefs
| Belief Category | Example Thought | Clinical Reality |
|---|---|---|
| Catastrophizing about consequences | "If I don't sleep tonight, I'll be completely useless tomorrow and could lose my job." | Acute sleep loss impairs performance, but the body compensates considerably; most catastrophic predictions are exaggerated. |
| Unrealistic sleep quantity requirements | "I need exactly 8 hours or I'm not healthy." | Sleep need varies individually; 7–9 hours is a population range, not a personal prescription. |
| The sleep effort paradox | "I have to try harder to fall asleep." | Sleep is an involuntary process — effortful attention to falling asleep activates arousal systems and prevents it. |
| Hypervigilance and misattribution | "I can always tell when I'm about to have a bad night." | Selective attention to sleep-related cues amplifies perceived severity; chronic insomnia patients often underestimate their actual sleep time. |
On the question of sleep requirements: most adults function well within a 7–9 hour range, and individual need varies considerably. The belief that 8 hours is a universal requirement is a population average misapplied as a personal standard. The FAQ on how many hours of sleep adults need addresses this directly.
How Cognitive Restructuring Works
Cognitive restructuring does not ask you to replace negative thoughts with positive ones. It asks you to examine the accuracy of your beliefs using the same logical standards you would apply to any other claim. The primary tools are:
- Thought records — Written documentation of the triggering situation, the automatic thought, the emotion it produces, the evidence for and against the thought, and a more balanced alternative.
- Socratic questioning — A series of guided questions designed to reveal the logical structure (and often the weaknesses) of a belief: What is the evidence? Has this prediction come true before? What would you tell a friend who said this?
- Decatastrophizing — Specifically examining worst-case sleep predictions against actual outcomes to demonstrate that the catastrophe rarely materializes at the predicted severity.
One technique that bridges cognitive and behavioral work is paradoxical intention (also called passive wakefulness): instead of trying to fall asleep, you try to stay passively awake while lying in bed with eyes closed. This directly addresses the sleep effort paradox — the act of trying to sleep activates the arousal system that prevents sleep. Removing the effort removes the activation.
Component 4: Sleep Hygiene Within CBT-I
Within CBT-I, sleep hygiene functions as the environmental and physiological substrate that makes the behavioral components more effective. The key behaviors are:
- Light exposure — Bright light in the morning anchors the circadian phase and reinforces the fixed wake time. Dim light in the two hours before the prescribed bedtime supports melatonin onset.
- Caffeine timing — Caffeine blocks adenosine receptors. With a half-life of approximately 5–7 hours, afternoon caffeine directly blunts the sleep pressure that sleep restriction is trying to build.
- Alcohol — Alcohol accelerates sleep onset but fragments the second half of the night through rebound arousal and REM suppression. It is not a CBT-I adjunct.
- Bedroom temperature — Core body temperature drops during sleep onset; a cool sleeping environment (roughly 65–68°F / 18–20°C) facilitates this.
- Exercise timing — Regular aerobic exercise improves sleep quality, but vigorous exercise within 2–3 hours of the prescribed bedtime can delay sleep onset in some individuals.
For a full treatment of these practices and the mechanisms behind them, the Sleep Hygiene Fundamentals guide covers the complete evidence-based bedtime routine framework. In the context of CBT-I, these practices matter most when they are undermining the protocol — caffeine blunting adenosine, alcohol fragmenting sleep, irregular wake times destabilizing the circadian anchor.
Component 5: Relaxation Training
Sleep restriction addresses the drive side of insomnia. Relaxation training addresses the arousal side. Both are necessary because chronic insomnia involves two distinct problems: insufficient sleep pressure and excessive pre-sleep physiological and cognitive activation. Relaxation techniques reduce the arousal component directly.
The five techniques used in CBT-I are:
- Progressive muscle relaxation (PMR) — Sequential tensing and releasing of muscle groups from feet to face. The contrast between tension and release trains the body to recognize and produce a lower baseline level of somatic arousal. Practiced daily, typically before the prescribed bedtime.
- Diaphragmatic breathing — Slow, deep breathing that activates the parasympathetic nervous system (the "rest and digest" branch) and lowers heart rate. Inhale through the nose for 4 counts, allowing the abdomen to rise; exhale slowly for 6–8 counts.
- Autogenic training — A self-directed technique involving focused attention on sensations of warmth and heaviness in the limbs, which induces a state of parasympathetic calm. Requires more practice than PMR before producing reliable relaxation.
- Biofeedback — Real-time physiological feedback (typically muscle tension or skin temperature) that helps individuals learn to recognize and control arousal states. More resource-intensive than the other techniques; typically used in clinical settings.
- Paradoxical intention (passive wakefulness) — Described in the cognitive restructuring section above. The instruction to try to stay passively awake removes the sleep effort that activates the arousal system. It is both a cognitive and a relaxation technique.
Relaxation training is practiced during the day as well as before bed — not only at the moment of sleep difficulty. Regular daytime practice builds the skill so that it is available and effective when needed at night, rather than being attempted for the first time under the pressure of insomnia.
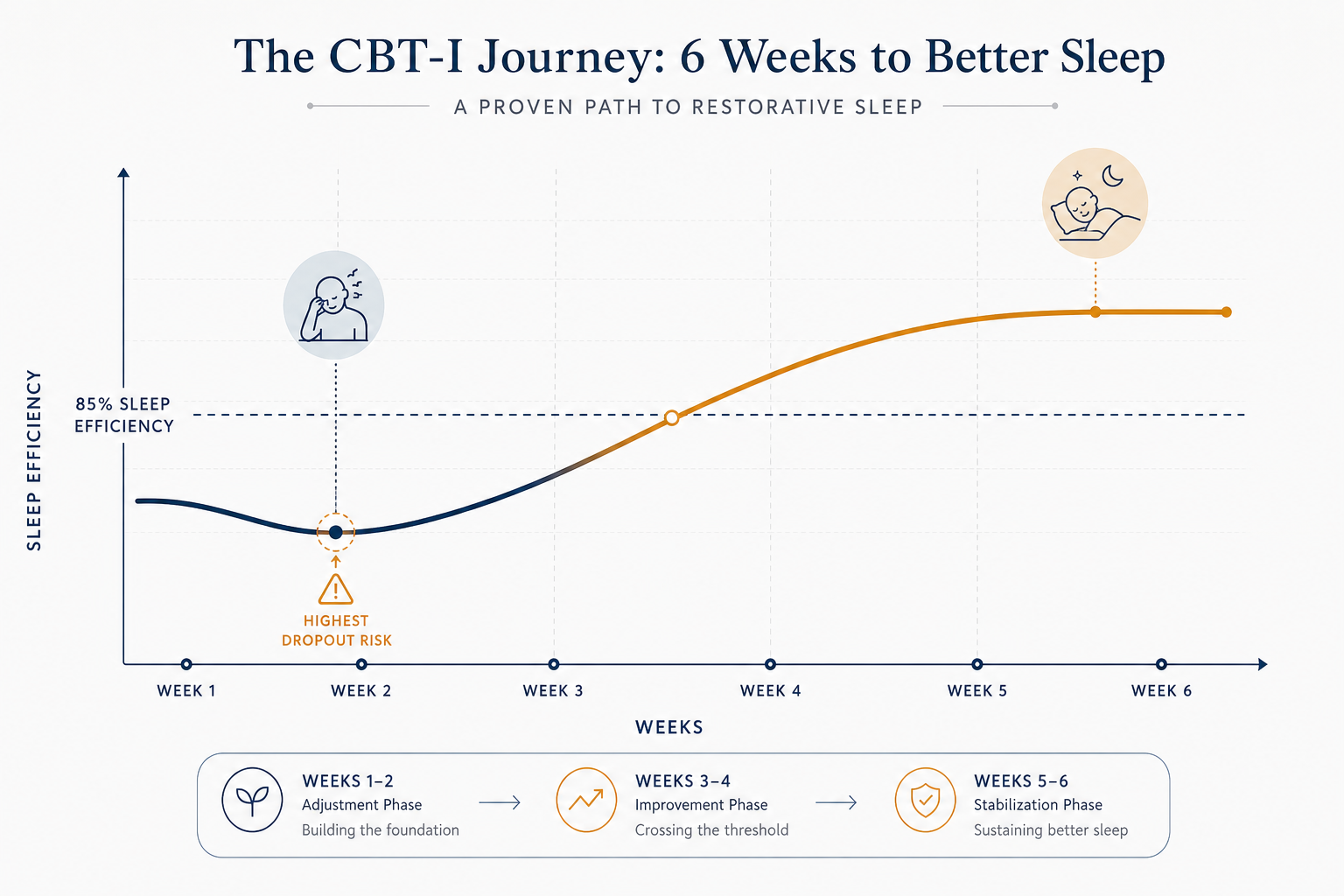
Week by Week: What to Expect Across the 6–8 Week Protocol
The most important thing to understand about the CBT-I arc is that it feels harder before it feels better — and the timing of that difficulty is not random. It maps directly onto the biological mechanisms at work.
| Week | What Is Happening Mechanistically | What You Are Likely to Experience | Titration Decision |
|---|---|---|---|
| Week 1 | Adenosine begins accumulating under restriction. Conditioned arousal is still strong. Sleep pressure is building but has not yet overcome the arousal threshold consistently. | Significant daytime fatigue, difficulty staying awake until prescribed bedtime, frustration. Sleep may feel no better — possibly worse. | Calculate baseline SE from pre-treatment diary. Set initial sleep window. No expansion yet. |
| Week 2 | Adenosine pressure is now substantial. Sleep efficiency is beginning to improve even if total sleep time has not. Conditioned arousal is starting to extinguish through repeated out-of-bed protocols. | Fatigue peaks. Some nights show clear improvement; others do not. This inconsistency is normal — extinction is not linear. Highest dropout risk point. | Calculate SE from week 1 diary. If SE ≥ 85%, expand window 15–30 min. If 80–84%, hold. If < 80%, contract. |
| Week 3 | Sleep efficiency typically crosses 85%. Slow-wave sleep (N3) depth has increased — the brain is using the restricted window to prioritize restorative sleep. Conditioned arousal is meaningfully reduced. | First clear improvement: falling asleep faster, fewer awakenings, waking feeling more rested. The out-of-bed protocol becomes easier to follow. | SE likely ≥ 85%. Expand window. Cognitive restructuring work deepens as catastrophizing reduces with evidence of improvement. |
| Week 4 | Sleep consolidation is stable. The circadian rhythm has been reinforced by the consistent wake time. Sleep efficiency remains high as the window expands. | Nights are more consistent. The anxiety about sleep begins to diminish. Catastrophizing is replaced by evidence-based confidence. | Continue weekly titration. Window expanding gradually toward individual sleep need. |
| Weeks 5–6 | Sleep is stable and self-reinforcing. The conditioned arousal association has been substantially extinguished. Sleep drive is well-regulated. Maintenance strategies are introduced. | Sleep is less fragile. The protocol feels less effortful. Maintenance habits replace the acute restrictions. | Titrate toward final sleep window. Introduce maintenance guidelines for sustaining gains after treatment ends. |
After CBT-I ends, sleep typically continues to improve. The neural patterns established during treatment do not reverse when sessions stop. Many patients report their best sleep in years at the three-to-six-month mark after completing the protocol — a trajectory that is the opposite of sleep medication, which produces tolerance and rebound.
Who CBT-I Is and Is Not Suitable For
CBT-I is appropriate for most adults with chronic insomnia, including those with comorbid anxiety, depression, chronic pain, and other medical conditions. The evidence supports its effectiveness across these comorbid presentations — in many cases, improving sleep through CBT-I also improves the comorbid condition.
Contraindications and Modifications
- Bipolar disorder — Sleep restriction can precipitate manic or hypomanic episodes. CBT-I for bipolar disorder requires specialist supervision and significant protocol modification.
- Seizure disorders / epilepsy — Sleep deprivation lowers the seizure threshold. Sleep restriction is contraindicated without neurological oversight.
- Excessive sleepiness disorders — Narcolepsy and idiopathic hypersomnia involve different pathophysiology; sleep restriction exacerbates rather than treats these conditions.
- Untreated parasomnias — Sleep restriction can worsen sleepwalking, REM sleep behavior disorder, and other parasomnias by increasing sleep pressure and slow-wave sleep.
- High fall risk — Older adults and individuals on medications that increase fall risk require careful assessment before sleep restriction; the daytime fatigue of early CBT-I creates additional hazard.
- Safety-critical occupations — Commercial pilots, surgeons, and others whose work involves acute safety consequences of impaired alertness should not begin sleep restriction without professional coordination.
For older adults who are not in the contraindicated categories, sleep compression is the preferred modification. Rather than immediately restricting time in bed to match TST, sleep compression gradually reduces the window over several weeks. The mechanism is the same — building sleep pressure — but the pace is gentler, reducing fall risk and tolerability concerns.
Digital CBT-I: Apps, Programs, and Self-Guided Options
The primary barrier to CBT-I has never been the evidence — it has been access. Trained CBT-I providers are scarce relative to the prevalence of chronic insomnia. Most primary care physicians are not equipped to deliver the protocol. Waitlists for behavioral sleep medicine specialists can extend months.
Digital CBT-I addresses this access problem directly. A 2025 meta-analysis of 49 randomized controlled trials involving more than 20,000 participants found that fully automated digital CBT-I significantly reduced insomnia severity compared to control conditions, with a weighted mean difference of –3.42 points on the Insomnia Severity Index (ISI). Critically, this effect held for fully automated programs without therapist involvement — expanding access to geographically isolated or lower-resource populations.
Current Digital CBT-I Options
- Somryst — An FDA-authorized prescription digital therapeutic for chronic insomnia in adults. As of Q2 2026, it is categorized by CMS as an evidence-based, reimbursable digital mental health treatment. Requires a prescription. Verify current coverage with your insurer.
- SleepioRx — Also FDA-cleared and CMS-categorized as of Q2 2026. Delivers a structured digital CBT-I program. Prescription and coverage requirements vary; check current access.
- CBT-I Coach — A free app developed by the VA and DoD. Not a standalone treatment program but a structured support tool for patients working through CBT-I with a provider or self-guided. Widely used, freely available, and evidence-informed.
Finding a CBT-I Provider and When to Seek Professional Supervision
For most adults with uncomplicated chronic insomnia, self-guided digital CBT-I produces meaningful results. Professional supervision becomes important — and in some cases necessary — in the following situations:
- Any of the contraindicated conditions listed above (bipolar disorder, seizure disorders, parasomnias, excessive sleepiness disorders, high fall risk)
- Significant comorbid psychiatric conditions — moderate-to-severe depression, PTSD, panic disorder — where CBT-I requires integration with psychiatric care
- No meaningful improvement after a full 6–8 week self-guided protocol
- Suspected comorbid sleep disorder (e.g., sleep apnea, restless legs syndrome) that has not been evaluated and may be contributing to insomnia
- Significant difficulty implementing sleep restriction or the out-of-bed protocol without guidance — the behavioral components are harder to sustain without accountability
How to Locate a Trained CBT-I Provider
- The AASM member directory lists accredited sleep centers and behavioral sleep medicine specialists by location. Search for providers with behavioral sleep medicine training or a CBSM (Certified Behavioral Sleep Medicine) credential.
- Clinical psychologists with sleep specialization often deliver CBT-I in outpatient settings, sometimes without the wait times of dedicated sleep centers.
- Some primary care practices and integrated behavioral health programs have added CBT-I to their service offerings as the evidence base and training infrastructure have expanded.
- Telehealth has substantially expanded access to trained CBT-I providers — location is no longer the barrier it once was for many patients.
One important framing note: CBT-I is not a passive treatment delivered to you. You are the active agent. The protocol gives you the tools, the titration rules, and the mechanistic understanding — but the work of staying out of bed at 3 AM, keeping the sleep diary, and examining your catastrophic sleep beliefs is yours. That active agency is also why the improvements last.
For readers considering OTC sleep aids or supplements alongside or instead of CBT-I, the melatonin evidence and safety guide covers the evidence, dosage, and population-specific safety considerations for the most commonly used sleep supplement — and the April 2026 AASM guideline's positioning of CBT-I above combination therapy applies equally to the question of whether adding a supplement is likely to improve on CBT-I alone.
Supports these guides
Spot an error or have clinical feedback?
Because this article covers clinical, medication, or safety information, we use a moderated correction channel instead of open public comments. Let us know if something about “CBT-I: A Complete Protocol Guide to Cognitive Behavioral Therapy for Insomnia” needs a closer look.
Send feedback on this article