Mechanism explainer
Why You Can't Sleep: A Mechanistic Guide to the Two-System Sleep Problem
If you feel tired but can't fall asleep, the problem is likely a mismatch between your sleep drive and circadian rhythm. This guide explains how both systems work, helps you identify which one is off, and shows you targeted fixes that go beyond generic sleep tips.

The Tired-but-Wired Paradox: Why You Feel Exhausted but Can't Sleep
You know the feeling. Your body is heavy, your eyes are burning, and you can barely keep them open on the couch. But the moment your head hits the pillow, your brain lights up like a control panel. Thoughts race. You check the clock. You calculate how many hours of sleep you'll get if you fall asleep right now. You don't.
This is not a failure of willpower. It is a biological mismatch between two distinct systems that regulate your sleep. According to data from the CDC's National Health Interview Survey, 14.5% of adults had trouble falling asleep most days or every day in 2020. A 2024 survey commissioned by the American Academy of Sleep Medicine found that 12% of Americans have been diagnosed with chronic insomnia. And among roughly 160,000 Sleep Foundation user profiles, more than 80% reported difficulty falling asleep at least some of the time.
The tired-but-wired paradox is so common because it has multiple root causes, and most generic sleep advice treats them all the same. This guide will help you identify which of your two sleep systems is out of balance — and what to do about it.
System 1: Your Sleep Drive — How Adenosine Builds Pressure to Sleep
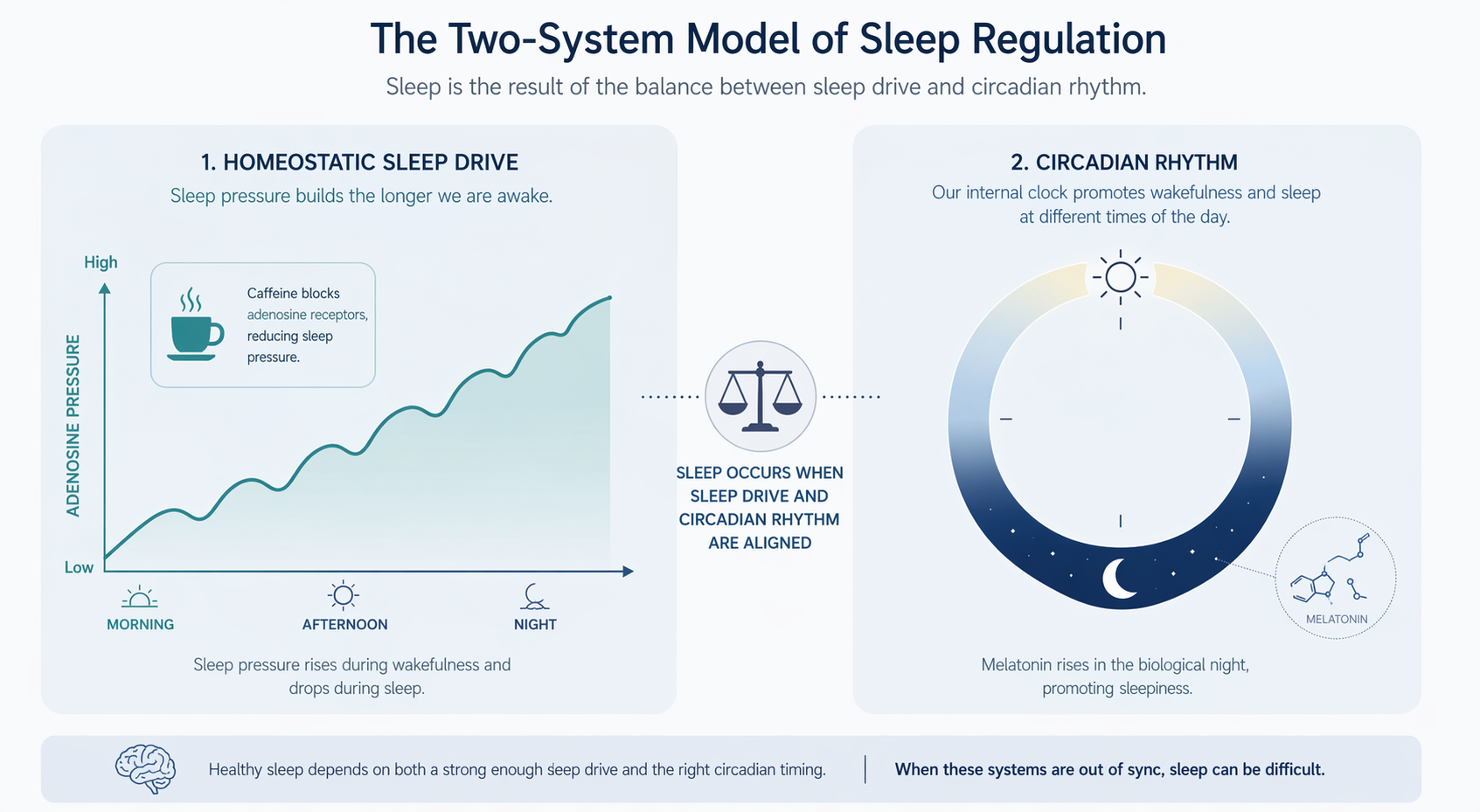
Your sleep drive is the biological pressure to sleep that builds the longer you stay awake. It is driven primarily by a neurotransmitter called adenosine. As your brain uses energy throughout the day, adenosine accumulates in the extracellular space. This accumulation limits activity in the brain areas that promote wakefulness, and the pressure to sleep grows.
Think of adenosine like a biological hourglass that starts emptying the moment you wake up. The longer you are awake, the more sand (adenosine) accumulates. By bedtime, the pressure should be high enough to ease you into sleep. While you sleep, your brain converts adenosine back into ATP, effectively resetting the hourglass for the next day.
Caffeine's Role: The Adenosine Blocker
Caffeine works by fitting into adenosine receptors in your brain, blocking adenosine from docking there. You still have plenty of adenosine circulating — your brain just cannot detect it. This is why caffeine makes you feel alert even when you are physiologically tired.
The problem is that caffeine does not clear quickly. It has an average half-life of about 5 hours. This means that if you consume 200 mg of caffeine at 2:00 PM (roughly a 16-ounce cup of brewed coffee), about 100 mg is still active in your system at 7:00 PM, and about 50 mg at midnight. Research cited by Healthline indicates that 200 mg of caffeine consumed 16 hours before bed can still measurably impact sleep. Consuming 400 mg of caffeine within 6 hours of bedtime may significantly reduce sleep quality.
Other factors can also reduce your sleep drive:
- Long or late naps: Napping for more than 20–30 minutes, or napping late in the day, releases some of your accumulated sleep pressure, making it harder to fall asleep at night.
- Insufficient wake time: If you spend too many hours in bed (sleeping in on weekends, lying in bed awake), you reduce the total time available for adenosine to build.
- Regular caffeine consumption: Your brain adapts by upregulating adenosine receptors, which means you may need more caffeine to feel the same effect, and your baseline sleep drive may be blunted.
System 2: Your Circadian Rhythm — The Body Clock That Times Your Sleep
While your sleep drive builds pressure to sleep, your circadian rhythm determines when that pressure is released. This internal body clock is controlled by the suprachiasmatic nucleus (SCN), a cluster of about 20,000 neurons in the hypothalamus. The SCN responds primarily to light signals received through your eyes.
In the morning, light exposure triggers the SCN to suppress melatonin and release cortisol, promoting alertness. As evening approaches, the SCN signals the pineal gland to begin melatonin production, preparing your body for sleep. This timing mechanism is remarkably precise — but it is also easily disrupted.
What Throws Your Circadian Rhythm Off
- Evening light exposure: Blue light from phones, tablets, and computers suppresses melatonin production. Your brain interprets the light as a signal that it is still daytime.
- Irregular sleep schedules: Going to bed and waking up at different times each day confuses the SCN. Your body clock relies on consistency to set its timing.
- Delayed sleep phase: Many people naturally have a circadian period slightly longer than 24 hours. Without strong morning light exposure to reset the clock each day, the rhythm drifts later and later.
- Shift work or jet lag: Abrupt changes to your light-dark schedule force your circadian rhythm out of alignment with your local environment.
For a deeper dive into how the SCN, melatonin, and cortisol interact, see our Circadian Rhythm Mechanisms article. For our purposes here, the key takeaway is this: your circadian rhythm tells your body when to be asleep, and your sleep drive tells it how badly you need to be asleep. When both systems are aligned, falling asleep feels natural. When they conflict, you get the tired-but-wired experience.
The Mismatch: What Happens When Sleep Drive and Circadian Timing Conflict
When your sleep drive and circadian rhythm are in sync, you fall asleep within 10–20 minutes of getting into bed. When they are out of sync, you lie awake despite feeling tired. There are three common mismatch scenarios, and each requires a different fix.
Scenario 1: Low Sleep Drive
You feel tired but not deeply sleepy. You may have napped during the day, consumed caffeine too late, or simply not been awake long enough to build sufficient adenosine pressure. This is common after sleeping in on weekends — you wake up later, so by your usual bedtime, you have only been awake for 14 hours instead of 16 or 17.
Scenario 2: Mistimed Circadian Rhythm
Your body is producing melatonin at the wrong time. This happens when you expose yourself to bright light late in the evening, keep an irregular sleep schedule, or have a naturally delayed circadian phase. You may feel alert at midnight even though you woke up at 7:00 AM — your body clock thinks it is still early evening.
Scenario 3: High Cognitive Arousal Overriding Sleep Drive
This is the classic tired-but-wired scenario. Your sleep drive is high, and your circadian timing is correct, but your brain is in a state of high alert. According to the Cleveland Clinic, when you lie down in a low-distraction environment, stressful thoughts can activate the fight-or-flight system, directly opposing the relaxation state needed for sleep. Over time, the bed itself becomes classically conditioned as a cue for worry.
Self-Triage: Which System Is Failing You?
Before you try any intervention, take five minutes to assess which mismatch type fits your experience. The table below walks through the key diagnostic questions for each scenario.
| Question | Low Sleep Drive | Mistimed Rhythm | Anxiety Activation |
|---|---|---|---|
| Do you feel physically sleepy when you get into bed? | No — you feel tired but not sleepy | Yes — you feel sleepy, but can't fall asleep | Yes — you feel exhausted, but your mind is racing |
| Did you consume caffeine after 2:00 PM? | Often yes | Not necessarily | Not necessarily |
| Did you take a nap longer than 30 minutes today? | Often yes | Not necessarily | Not necessarily |
| Do you use your phone or watch TV in bed? | Not necessarily | Often yes — especially in the hour before bed | Not necessarily — but you may be lying in bed worrying |
| Is your sleep schedule consistent? | Usually consistent | Often inconsistent — different bedtimes on weekends | Usually consistent |
| What happens when you lie down? | You feel alert, not particularly anxious | You feel sleepy but your body doesn't 'switch off' | Your mind immediately starts racing about tomorrow |
If you checked multiple boxes across different columns, you may have a combination of issues. Start with the scenario that feels most dominant — the one that describes your experience most nights.
Targeted Interventions for Each Mismatch Type
The reason generic sleep tips often fail is that they treat all three scenarios the same. A caffeine cutoff recommendation will not help someone whose problem is anxiety-driven arousal. A relaxation technique will not fix a mistimed circadian rhythm. Matching the intervention to the specific system failure is far more effective.
If Your Problem Is Low Sleep Drive
Your goal is to increase the adenosine pressure that builds during the day. The most effective levers are:
- Set a caffeine cutoff: Stop all caffeine by 1:00–2:00 PM. Given the 5-hour half-life, this gives your body enough time to clear most of the caffeine before bedtime. If you are particularly sensitive, consider cutting off at noon.
- Limit naps to 20 minutes or less: Short naps can be refreshing without releasing significant sleep pressure. Naps longer than 30 minutes, especially after 3:00 PM, can reduce your sleep drive for the night.
- Avoid sleeping in on weekends: If you wake up 2–3 hours later on Saturday and Sunday, you reduce your total wake time before your usual bedtime, making it harder to fall asleep Sunday night.
- Consider sleep restriction: If you spend 9 hours in bed but only sleep 6, you are diluting your sleep drive. Temporarily limiting your time in bed to your actual sleep time can rebuild sleep pressure. This is a core component of CBT-I and should be done with guidance.
If Your Problem Is a Mistimed Circadian Rhythm
Your goal is to anchor your body clock to a consistent light-dark cycle. The most effective interventions are:
- Get morning light exposure: Within 30–60 minutes of waking, expose yourself to natural daylight for at least 15–20 minutes. This signals the SCN that the day has started and sets your circadian timing for the next 24 hours.
- Keep a consistent wake time: Wake up at the same time every day, including weekends. Your circadian rhythm is more sensitive to wake time than to bedtime. A consistent wake time anchors your entire sleep schedule.
- Reduce evening light exposure: Dim your lights 1–2 hours before bed. Avoid screens, or use blue-light blocking settings. Even dim indoor light can suppress melatonin production by 50% or more.
- Create a wind-down routine: A consistent 30–60 minute pre-bed routine signals your body that sleep is approaching. This is covered in detail in our Sleep Hygiene Fundamentals guide.
If Your Problem Is Anxiety Activation
Your goal is to break the conditioned association between your bed and worry. The most effective interventions are:
- Scheduled worry time: Set aside 15 minutes in the early evening to write down everything on your mind. Close the notebook and tell yourself you will not revisit those thoughts until tomorrow's scheduled time. This contains the worry to a specific window.
- The 15–20 minute rule: If you have been in bed for 15–20 minutes without falling asleep, get up and go to another room. Do something calm and boring (reading a physical book, folding laundry) in dim light. Return to bed only when you feel sleepy. This is the core of Stimulus Control Therapy — it breaks the conditioned link between bed and wakefulness.
- Mindfulness or slow breathing: Practices like body scan meditation or 4-7-8 breathing can reduce fight-or-flight arousal. These are not quick fixes, but consistent practice over 2–4 weeks can lower baseline anxiety levels at bedtime.
- Gratitude journaling: Writing down three things you are grateful for each evening has been shown to reduce pre-sleep cognitive arousal in some studies.

When to See a Doctor: Beyond the Two-System Model
The two-system model explains most cases of difficulty falling asleep, but not all. If any of the following apply to you, it is worth seeking a professional evaluation:
- Your sleep difficulty has persisted for more than 3 months, occurring at least 3 nights per week
- You experience significant daytime impairment — fatigue, mood changes, difficulty concentrating — even when you do get some sleep
- You suspect an underlying sleep disorder such as sleep apnea (loud snoring, gasping for air) or restless legs syndrome (uncomfortable leg sensations that improve with movement)
- You have tried the targeted interventions above consistently for 4–6 weeks without improvement
For chronic insomnia, the American Academy of Sleep Medicine recommends cognitive behavioral therapy for insomnia (CBT-I) as the first-line treatment. Research shows that 7 to 8 out of 10 people who complete CBT-I experience significant improvement, typically within 6 to 8 weeks. Our self-directed CBT-I guide explains how to apply the core techniques — stimulus control, sleep restriction, and cognitive restructuring — without a therapist.
Supports these guides
Spot an error or have clinical feedback?
Because this article covers clinical, medication, or safety information, we use a moderated correction channel instead of open public comments. Let us know if something about “Why You Can't Sleep: A Mechanistic Guide to the Two-System Sleep Problem” needs a closer look.
Send feedback on this article