
Why the 'Non-Habit-Forming' Label Exists
Walk into any pharmacy and you will see the phrase 'non-habit-forming' printed prominently on boxes of diphenhydramine (Benadryl, ZzzQuil), doxylamine (Unisom), and their store-brand equivalents. The term sounds reassuring, but its origin has less to do with modern safety science and more to do with a regulatory distinction made decades ago.
During the 1970s and 1980s, the U.S. Food and Drug Administration (FDA) established the OTC monograph system to classify ingredients that are generally recognized as safe and effective for nonprescription use. At the time, the primary concern was distinguishing first-generation antihistamines from the prescription sedatives that were known to cause physical addiction — namely benzodiazepines (Valium, Xanax) and barbiturates. Unlike those drugs, antihistamines do not activate the brain's dopamine reward pathway in a way that produces compulsive drug-seeking behavior. The FDA therefore permitted manufacturers to label them 'non-habit-forming' to signal that they were not physically addictive in the same sense.
The label was never intended to guarantee that a person could use these products indefinitely without consequences. It was a narrow regulatory carve-out designed to help consumers distinguish between two very different classes of sedatives. Over time, that nuance has been lost.
Physical Dependence vs. Psychological Reliance vs. Tolerance
To understand what the label actually means — and what it conceals — it helps to separate three distinct phenomena that are often lumped together under the word 'habit-forming.'
Physical dependence (addiction) involves changes in brain chemistry that drive compulsive use despite harm. Antihistamines do not produce this effect. You will not experience the intense cravings or withdrawal syndromes associated with opioids or benzodiazepines. On this point, the label is accurate.
Tolerance is a different story. According to the Mayo Clinic (January 2026), tolerance to the sedative effects of antihistamines develops quickly — the longer you take them, the less likely they are to make you sleepy. Many users find that a dose that worked well on night one produces little effect by night five or six. This leads to a common but dangerous response: taking more.
Psychological reliance is the third piece. Even when a substance does not cause physical addiction, a person can come to believe they cannot fall asleep without it. As Ubie Health (March 2026) puts it: 'If you feel like you cannot sleep at all without something, that's a sign to reassess.' This is not addiction in the clinical sense, but it is a real barrier to healthy sleep.
| Concept | Definition | Does it occur with OTC antihistamines? | Key sign |
|---|---|---|---|
| Physical dependence (addiction) | Brain chemistry changes drive compulsive use; withdrawal syndrome on cessation | No — antihistamines do not activate dopamine reward pathways | Cravings, loss of control over use |
| Tolerance | Diminished response to the same dose over time | Yes — develops rapidly, often within days to weeks | Needing a higher dose to achieve the same sedation |
| Psychological reliance | Belief that sleep is impossible without the aid | Yes — common with regular use, even short-term | Anxiety about sleeping without the product |
| Rebound insomnia | Sleep temporarily worsens after discontinuation | Yes — can trap users in a cycle of continued use | Worse sleep on停药 nights than before starting |
Rebound Insomnia: What Happens When You Stop
One of the most insidious effects of regular antihistamine use is rebound insomnia — a temporary worsening of sleep that occurs when you stop taking the drug. This is not withdrawal in the addiction sense, but it feels similar: you lie awake longer than you did before you ever took the first pill.
Dr. Richard Castriotta, a pulmonologist and sleep specialist at UTHealth, explained the dynamic in a Consumer Reports survey covered by ABC13: when users stop, their insomnia often worsens, and 'it takes a while to come back.' The brain has adapted to the presence of the sedating antihistamine, and it needs time to recalibrate its natural sleep-wake signaling.
This rebound effect is a major reason people end up using OTC sleep aids far longer than recommended. The same Consumer Reports national survey found that 20% of adults had taken an OTC sleep medication within the past year, and of those, 41% had used them for a year or longer — well beyond the FDA's two-week short-term window. The cycle is predictable: you stop, sleep gets worse, you assume you 'need' the aid, and you start again.
What the Label Doesn't Tell You: Anticholinergic Risks and Dementia
The 'non-habit-forming' label is silent on a set of risks that have nothing to do with dependence but everything to do with long-term safety. First-generation antihistamines like diphenhydramine and doxylamine are potent anticholinergic agents — they block the neurotransmitter acetylcholine, which plays a critical role in memory, learning, and muscle function.
The immediate side effects of anticholinergic activity are well documented. The Mayo Clinic lists daytime drowsiness, dry mouth, constipation, and urinary retention as common effects. For most younger adults, these are manageable annoyances. For older adults, the consequences can be far more serious.
- Falls and confusion: The anticholinergic burden of these drugs is linked to cognitive impairment, confusion, and an increased risk of falls in people over 65.
- Beers Criteria listing: Both diphenhydramine and doxylamine are included on the American Geriatrics Society Beers Criteria for Potentially Inappropriate Medication Use in Older Adults, meaning they should generally be avoided in this population.
- Dementia risk: A landmark 2015 study published in JAMA Internal Medicine found that frequent, long-term use of anticholinergic medications, including OTC sleep aids, was associated with an increased risk of dementia. The mechanism is thought to involve cumulative anticholinergic burden over years of use.
- Contraindicated conditions: The Mayo Clinic specifically advises against using these drugs in people with closed-angle glaucoma, peptic ulcer disease, or urinary retention, as anticholinergic effects can worsen these conditions.
None of this information appears on the box. The 'non-habit-forming' label addresses one narrow question — 'Will this make me addicted?' — and leaves the broader safety picture unexamined.
Which Sleep Aids Are Truly Low-Risk for Dependence?
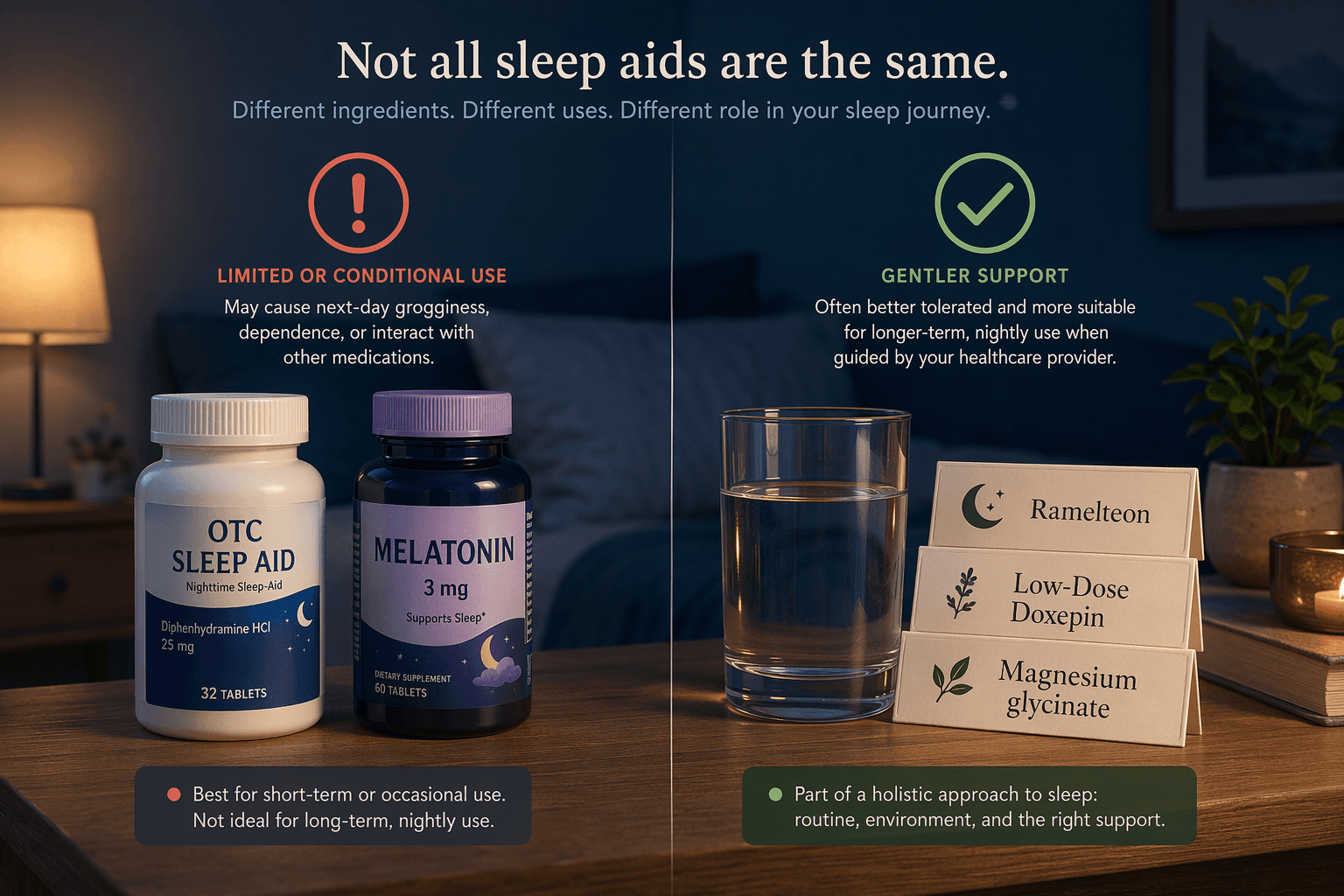
If first-generation antihistamines carry hidden risks, what are the alternatives? The answer depends on whether you are dealing with short-term situational insomnia or a chronic sleep problem, but several options stand out for their more favorable dependence and safety profiles.
Ramelteon (brand name Rozerem) is a prescription melatonin-receptor agonist that targets the same receptors as the body's natural sleep hormone. According to Harvard Health (2017), it is 'not thought to be habit-forming' because it does not interact with GABA receptors — the mechanism behind the dependence risk of benzodiazepines and Z-drugs. The Sleep Foundation notes that ramelteon is generally well tolerated, though daytime drowsiness is possible, and it is not recommended for sleep-maintenance insomnia (waking up in the middle of the night).
Low-dose doxepin (3–6 mg) is a prescription tricyclic antidepressant that, at these very low doses, acts primarily as a histamine receptor blocker — but without the strong anticholinergic effects of diphenhydramine. A 2025 review in the Cleveland Clinic Journal of Medicine confirms that at 3–6 mg, doxepin improves sleep maintenance with no memory problems or anticholinergic effects at studied doses in a 12-week RCT. It is considered a safer option for older adults compared to first-generation antihistamines.
For those seeking nonprescription options, the evidence is more mixed but worth examining. A 2024 review in The American Journal of Lifestyle Medicine (Esquivel) identified seven RCTs on melatonin, five of which showed statistically significant improvements in sleep quality compared to placebo, though doses ranged from 3 to 10 mg. The American Academy of Sleep Medicine (AASM) does not recommend melatonin for insomnia, but it remains a widely used option with a low dependence risk. L-theanine at 200 mg/day significantly improved PSQI scores in healthy adults in a 2019 study (Hidese et al., Nutrients). For magnesium, two RCTs showed no benefit except in individuals with low baseline serum magnesium, so its utility depends on your individual status.
| Option | Type | Mechanism | Dependence risk | Evidence quality | Best for |
|---|---|---|---|---|---|
| Ramelteon (Rozerem) | Prescription | Melatonin-receptor agonist | Very low (not thought to be habit-forming per Harvard Health) | RCT-supported for sleep onset | Sleep-onset insomnia; older adults |
| Low-dose doxepin (3–6 mg) | Prescription | Histamine receptor blockade (low anticholinergic) | Low | RCT-supported for sleep maintenance | Sleep-maintenance insomnia; older adults |
| Melatonin (0.5–3 mg) | Dietary supplement | Melatonin-receptor activation | Very low | Mixed — 5 of 7 RCTs showed improvement (Esquivel 2024) | Circadian disruption, jet lag, mild sleep-onset difficulty |
| L-theanine (200 mg/day) | Dietary supplement | Increases GABA, serotonin, dopamine levels | Very low | Single RCT showed PSQI improvement (Hidese 2019) | Mild anxiety-related sleep difficulty |
| Magnesium glycinate | Dietary supplement | NMDA receptor antagonism, GABA support | Very low | Limited — benefit only in low-baseline-magnesium individuals | Individuals with confirmed magnesium deficiency |
| Diphenhydramine / Doxylamine | OTC drug | First-generation antihistamine (anticholinergic) | Low for physical addiction; high for tolerance and psychological reliance | AASM does not recommend for insomnia | Short-term use only (≤2 weeks); not for older adults |
Practical Takeaways for Readers
The 'non-habit-forming' label is not a lie, but it is incomplete. It tells you one true thing — that antihistamines are not physically addictive like benzodiazepines — and leaves you to discover the rest on your own. Here is what the evidence actually supports.
- OTC antihistamine sleep aids are for short-term use only. The FDA's two-week window is not arbitrary — it reflects the rapid development of tolerance and the risk of rebound insomnia. If you have been using diphenhydramine or doxylamine for more than two weeks, you are already outside the intended use case.
- Tolerance and psychological reliance are real, even if physical addiction is not. If you feel anxious about sleeping without your OTC aid, that is a signal to reassess — not a reason to double the dose.
- Older adults should avoid diphenhydramine and doxylamine entirely. The Beers Criteria, the Mayo Clinic, and the CCJM review all converge on this point: the anticholinergic risks outweigh the benefits for people over 65. Safer prescription options like low-dose doxepin or ramelteon should be discussed with a clinician.
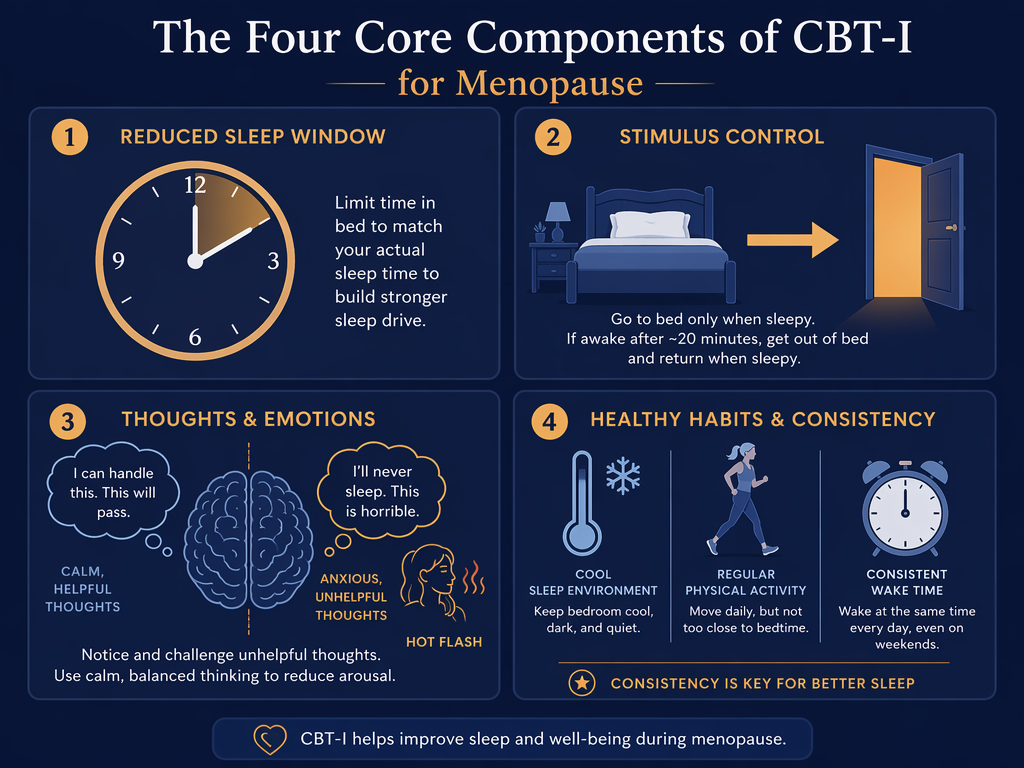
- If insomnia persists beyond a few weeks, an OTC sleep aid is not the solution. The AASM and the CCJM both identify Cognitive Behavioral Therapy for Insomnia (CBT-I) as the gold standard first-line treatment for chronic insomnia. It addresses the underlying causes of poor sleep without any pharmacological dependence risk.
- Supplements like melatonin and L-theanine have lower dependence risk but mixed evidence. They may be reasonable options for situational use, but they are not a substitute for a clinical evaluation if your sleep problem is persistent.

Comments
Join the discussion with an anonymous comment.