The sleep-aid shelf can make very different products look like close relatives. A box of diphenhydramine tablets, a bottle of doxylamine capsules, melatonin gummies, valerian drops: all are sold without a prescription, often under the same soft blue packaging language about rest, nighttime, and waking refreshed. But “over the counter sleep aid” is not one regulatory category. It is a shopping condition.
The first useful question is not whether a product is available at the drugstore. It is whether the product is an OTC drug marketed under FDA rules for nighttime sleep-aid drug products, or a dietary supplement sold under a different law that does not require FDA pre-approval for safety or effectiveness before it reaches the shelf.

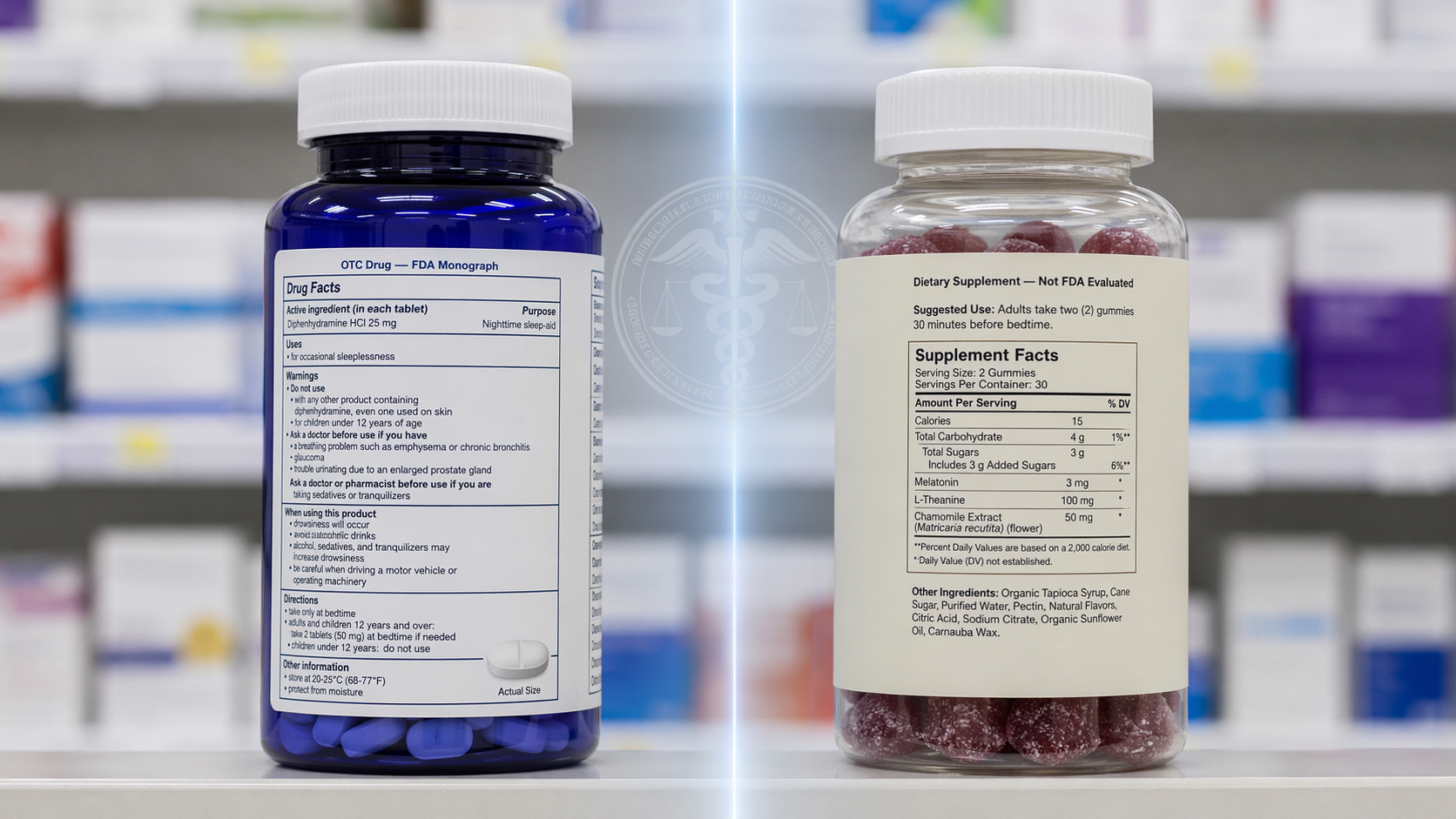
The Shelf Uses One Phrase for Two Regulatory Paths
Diphenhydramine and doxylamine are the familiar antihistamines used in many OTC nighttime sleep-aid drugs. In the Code of Federal Regulations, 21 CFR Part 338 covers “Nighttime Sleep-Aid Drug Products for Over-the-Counter Human Use” and specifies which active ingredients, doses, indications, warnings, and directions can appear for these products when they are marketed under the monograph system.[1]
That does not mean each individual box has gone through the same approval process as a new prescription drug. It means the product must fit within an FDA-established OTC drug framework: recognized active ingredients, standardized labeling, manufacturing expectations, and drug-style adverse-event obligations. If the box says diphenhydramine 25 mg or doxylamine succinate 25 mg, the manufacturer is operating in a drug category where the active ingredient and the label claim are part of a formal rule set.[1]
Melatonin and valerian are different. They are sold as dietary supplements. Under the Dietary Supplement Health and Education Act of 1994, supplements are not pre-approved by the FDA for safety or efficacy before marketing in the way drugs are. The FDA can act when a product is adulterated, misbranded, or linked to a safety problem, but it does not routinely verify that a sleep supplement’s label claim has been proven or that the labeled amount matches the contents before the bottle goes to market.[2]
| If the product is... | What “over the counter” usually means | What a shopper should not assume |
|---|---|---|
| Diphenhydramine or doxylamine sleep aid | An OTC drug marketed under FDA monograph rules for nighttime sleep-aid products | That it is appropriate for nightly or long-term insomnia use |
| Melatonin, valerian, or other sleep supplement | A dietary supplement sold without FDA pre-approval for safety or effectiveness | That the dose, purity, or sleep claim has been independently verified by FDA before sale |
That distinction is dull only until it becomes practical. It affects what the number on the front of the package means, how much confidence to place in the stated dose, and whether the sleep claim has passed through a drug framework or a supplement marketplace.
For Supplements, the Dose on the Label May Be the Weak Link
Melatonin is often described casually, almost as if it were closer to a vitamin than a sleep aid. That framing can make a gummy seem lower-stakes than a tablet in a drug box. The problem is not that every melatonin product is dangerous. The problem is that the supplement category gives the shopper less built-in assurance that the labeled dose is the dose being swallowed.
Sleep Foundation reports that an analysis of 32 melatonin gummy brands found actual melatonin content ranging from 0.8 mg to 23.9 mg per serving, a roughly 30-fold spread across products.[2] The same source reports that more than 70% of melatonin supplements have significant discrepancies between labeled and actual melatonin content.[2] Those figures are not a reason to panic over every bottle; they are a reason to stop treating the front-label milligram number as if it were automatically drug-grade dosing information.

The consumer consequence is easy to miss. A person may think they are making a careful choice by starting with one gummy, staying below a higher dose, or comparing “5 mg” products across brands. If one brand contains much less than expected and another contains much more, the usual self-management logic begins to wobble. The person who feels groggy the next morning may blame their own sensitivity. The person who feels nothing may keep escalating. In both cases, the label may not be giving the clean information they think it is.
There is also a difference between a sleep claim that is plausible and a sleep claim that is well supported for the problem at hand. Consumer Reports summarized evidence suggesting melatonin helps people fall asleep about 7 minutes faster on average, with the best evidence for circadian rhythm problems such as jet lag or delayed sleep phase rather than chronic insomnia.[3] That is a narrower benefit than the broad “sleep support” aura on many bottles suggests.
Valerian and other botanical sleep supplements fit the same regulatory pattern even when their evidence questions differ. They may be marketed next to OTC drugs, but they do not enter the market through the same pre-sale drug review gate. Contaminants and undisclosed ingredients have also been raised as supplement concerns by medical and consumer health sources, though that should not be stretched into a claim that all sleep supplements are contaminated.[3][4]
The American Academy of Sleep Medicine’s 2017 clinical practice guideline is a useful check on both sides of the aisle: it recommends against using melatonin, valerian, or diphenhydramine for chronic insomnia because the evidence for benefit and safety is not strong enough.[10] Different regulatory paths do not make either category a reliable long-term insomnia treatment.
FDA-Monographed Does Not Mean Good for Nightly Use
The opposite mistake is to look at the drug box and relax too much. Diphenhydramine and doxylamine have a clearer regulatory status as OTC nighttime sleep-aid drugs, but that status is not a blessing for open-ended use. The monograph tells you what the product is allowed to contain and say. It does not mean the product is a good answer to months of insomnia.
These drugs are sedating antihistamines with anticholinergic effects. For an occasional bad night, some adults may experience the sedation they were looking for. The same properties can also produce next-day drowsiness, dry mouth, constipation, urinary retention, blurred vision, confusion, and falls, especially in older adults or in people taking other medicines with similar effects.[4]
This is where the phrase “non-habit-forming” can be too soothing. It may distinguish these products from some prescription sedatives, but it does not address the practical pattern that develops when a person starts using an antihistamine every night because it works well enough to keep them from dealing with the insomnia itself. Tolerance to the sedating effect can develop, side effects can accumulate, and the original sleep problem can remain untreated.
Older adults deserve special caution. The American Geriatrics Society Beers Criteria classify diphenhydramine and doxylamine as potentially inappropriate for adults 65 and older because of their anticholinergic burden and risk profile.[4] A 2021 systematic review of OTC medications for primary insomnia in older people also found limited support for these products in that population, which matters because older adults are often the very people most vulnerable to residual sedation and confusion.[5]
The dementia discussion needs care. Harvard Health summarizes research from Gray and colleagues in JAMA Internal Medicine that followed about 3,500 adults age 65 and older over 7 years; 800 developed dementia, and those with 3 or more years of cumulative use of strong anticholinergic drugs had a 54% higher dementia risk than those with shorter or lower exposure.[6] That is an observational association, not proof that diphenhydramine or doxylamine caused dementia. People in early, undiagnosed cognitive decline may also use more medications for sleep, mood, or other symptoms. Still, the association is enough to make casual long-term use a poor bargain in older adults.
The Real-World Problem Is Usually Repetition
Most people do not buy an over the counter sleep aid because they are trying to build a medication regimen. They buy it because three bad nights have made work, parenting, caregiving, or basic patience feel harder. The short-term relief is real enough to respect. A product that helps someone get through a travel week, a temporary stressor, or a disrupted schedule can feel like a rescue.
But repetition changes the safety question. One or two nights of an OTC antihistamine is a different decision from taking it nightly for months. Trying melatonin for jet lag is a different decision from using escalating gummy doses to manage chronic insomnia. A supplement with a loose dose range and a drug with a predictable dose can both become the wrong tool when they are used to postpone a proper evaluation.
Pharmacists and clinicians often see the cleanup version of this problem. Someone may be taking diphenhydramine for sleep while also using an allergy medicine, a cold product, or another medication with anticholinergic effects. Someone else may be switching between melatonin brands and assuming that “5 mg” means the same exposure each time. In a study of OTC medications containing diphenhydramine or doxylamine used by older adults, researchers found that these products were being used in a population where medication review and counseling matter, not as harmless background items.[7]
What to Check Before You Put It in the Cart
The label can usually tell you which regulatory world you are in. On an OTC drug, look for a Drug Facts panel and an active ingredient such as diphenhydramine or doxylamine. On a supplement, look for a Supplement Facts panel and ingredients such as melatonin, valerian, magnesium, L-theanine, or herbal blends. The panels are not decoration; they are the fastest clue to what kind of oversight sits behind the product.
- If it has a Drug Facts panel: treat the dose as more standardized, but read the warnings as seriously as the sleep claim.
- If it has a Supplement Facts panel: do not assume FDA has verified the dose, purity, or effectiveness before sale.
- If you are 65 or older: avoid making diphenhydramine or doxylamine a routine sleep solution without medical advice.
- If you are pregnant, breastfeeding, managing a chronic condition, or taking other sedating or anticholinergic medicines: ask a clinician or pharmacist before using either category.
- If insomnia is lasting weeks or becoming nightly: stop treating the shelf as the treatment plan.
Mayo Clinic and Cleveland Clinic both frame OTC sleep aids as products that require caution, especially for people with medical conditions, older adults, pregnant people, and those taking other medications.[8][9] That advice can sound generic until a real person is standing in the aisle with four hours of sleep behind them. The point is not that every purchase requires an appointment. The point is that certain flags should move the decision from self-experimentation to a quick medication check.
A Better Standard Than “Can I Buy It Without a Prescription?”
A useful standard starts with the category. Is this an OTC drug with diphenhydramine or doxylamine, marketed under the FDA’s nighttime sleep-aid monograph? Or is this a dietary supplement, where the label may make a sleep-support claim without FDA pre-approval for safety or effectiveness?
Then the judgment splits. For supplements, be cautious about dose precision and broad claims, especially with melatonin gummies and other products where label-content discrepancies have been documented. For antihistamine sleep aids, be cautious about repeated use, next-day impairment, duplicate ingredients, and anticholinergic risk. Neither category is a good substitute for evaluating chronic insomnia, and neither becomes harmless because it is sold beside toothpaste.
The most protective move is often small: turn the bottle around. Drug Facts or Supplement Facts tells you which assumptions to drop before you take the first dose.
References
- 21 CFR Part 338 Nighttime Sleep-Aid Drug Products, eCFR.
- Compare Sleep Aids: Understanding the Differences, Sleep Foundation.
- The Truth About Popular Sleep Supplements, Consumer Reports, 2023.
- Drugstore sleep aids may bring more risks than benefits, Harvard Health.
- Systematic review of OTC medications for primary insomnia in older people, PubMed, 2021.
- Common anticholinergic drugs like Benadryl linked to increased dementia risk, Harvard Health, updated 2025.
- OTC medications containing diphenhydramine/doxylamine used by older adults, International Journal of Clinical Pharmacy, 2017.
- Sleep aids: Understand options sold without a prescription, Mayo Clinic.
- What to Know About Over-the-Counter Sleep Aids, Cleveland Clinic.
- Clinical Practice Guideline for the Pharmacologic Treatment of Chronic Insomnia in Adults, American Academy of Sleep Medicine, 2017.


Comments
Join the discussion with an anonymous comment.