Introduction: When Your Sleep Aid Stops Working
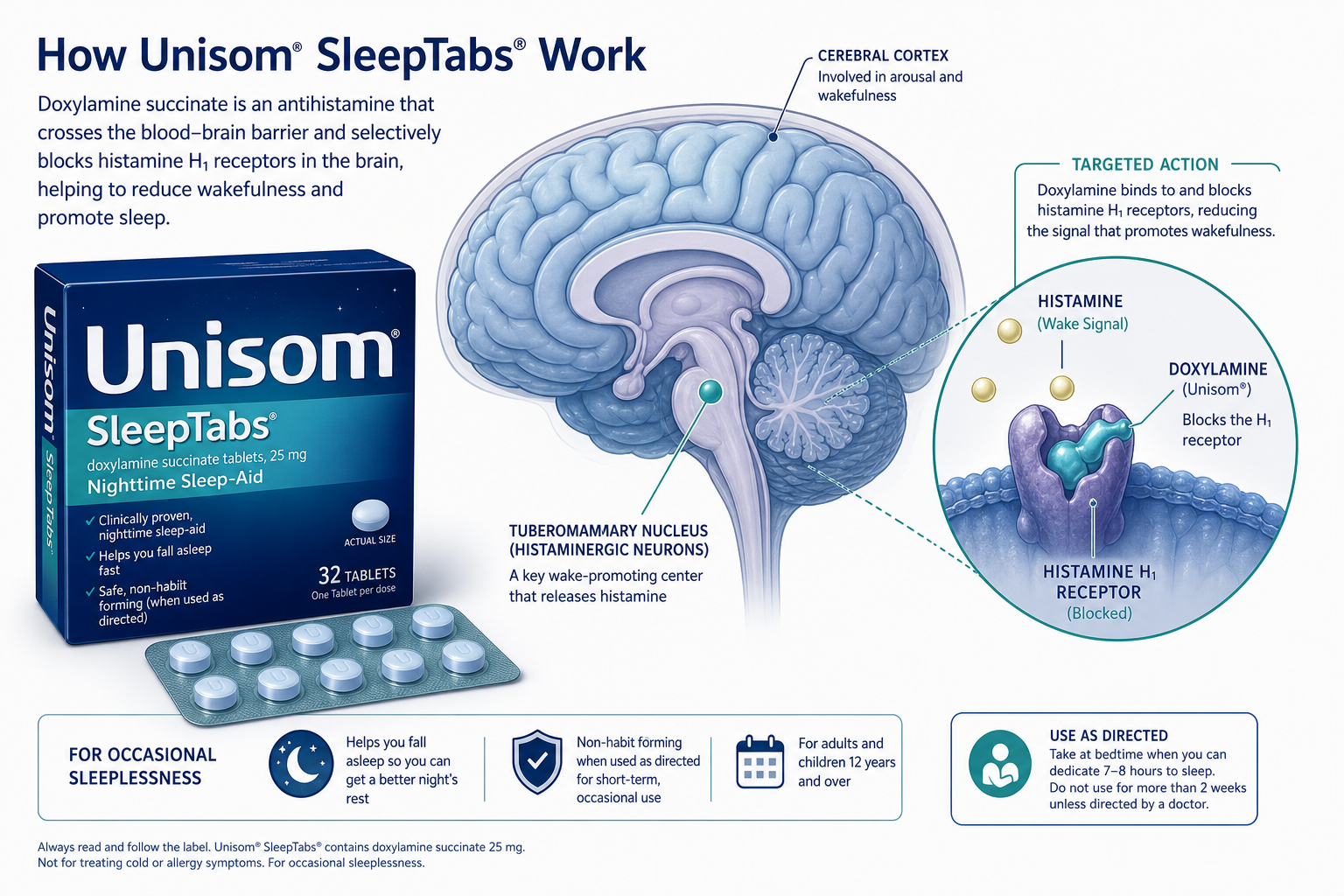
If you started taking Unisom SleepTabs and they worked well for a week or two, only to leave you staring at the ceiling again a few nights later, you are not imagining things. This is a well-documented pattern, not a sign that you are somehow immune to the medication. The active ingredient, doxylamine succinate 25 mg, is a first-generation antihistamine that induces sleepiness by blocking histamine receptors in the brain. But that mechanism has a built-in expiration date for many users.
This article is not a general safety guide — that territory is covered in our detailed doxylamine safety explainer. Instead, this is written for the person who has already tried Unisom SleepTabs, experienced diminishing returns, and needs to understand why it happened and what to do next. We will walk through the pharmacology of tolerance, the mismatch between what doxylamine treats and what causes chronic insomnia, the risks of pushing past the FDA's two-week limit, and a clinical stepwise approach for finding a solution that actually works long-term.

Why Unisom SleepTabs Lose Their Effect: The Tolerance Problem
The primary reason Unisom SleepTabs stop working is pharmacological tolerance. When you take doxylamine nightly, your brain adapts to the presence of the drug. The histamine H1 receptors that the medication blocks begin to upregulate — meaning the brain produces more of them or makes them more sensitive — to overcome the blockade. At the same time, the central nervous system may downregulate its own sedative response. The net effect is that the same 25 mg dose that once produced reliable drowsiness now barely registers.
This is not a subtle or rare phenomenon. The Mayo Clinic states plainly: "Tolerance to the effects of antihistamines can develop quickly. The longer you take them, the less likely they are to make you sleepy." Harvard Health sleep expert Dr. Lawrence Epstein puts it even more directly: "You tend to become tolerant of the effect relatively quickly, so they stop working for you." The clinical literature from StatPearls confirms that tolerance to the sedative effects of first-generation antihistamines can emerge within days to weeks of regular use.
User review data reinforces just how common this experience is. On Drugs.com, Unisom SleepTabs hold an average rating of 5.7 out of 10 across 82 reviews, with 39% of users reporting a negative experience. Many of those negative reviews describe the same trajectory: initial success followed by progressive loss of effect. On WebMD, the overall rating is 4.0 out of 5 from 288 reviews, but the written accounts frequently cite tolerance and diminishing returns as primary frustrations. Some users report taking the medication for years — far beyond the label's two-week limit — and describe a slow erosion of effectiveness that led them to seek alternatives.

The Root Cause Mismatch: Why Doxylamine Can't Fix Chronic Insomnia
Even if tolerance were not an issue, doxylamine would still be a poor match for chronic insomnia because it only addresses one narrow pathway: histamine-mediated wakefulness. Doxylamine is an H1 receptor antagonist. It blocks the action of histamine, a neurotransmitter that promotes alertness and wakefulness. That is all it does. It does not address the systems that actually drive chronic insomnia.
Chronic insomnia is rarely caused by an overactive histamine system. The primary drivers, as outlined in clinical frameworks from sources like Ubie Health, include:
- Cognitive and physiological hyperarousal: A state where the brain's arousal systems are stuck in an overactive mode, often driven by anxiety, stress, or conditioned worry about sleep itself. A sedating antihistamine cannot override this level of activation.
- Circadian rhythm disruption: Misalignment between the internal body clock and the desired sleep-wake schedule. Doxylamine does not reset circadian timing.
- Sleep-disordered breathing: Conditions like obstructive sleep apnea cause repeated awakenings throughout the night. A sedative may mask the symptoms but does not treat the airway obstruction.
- Restless legs syndrome (RLS): An urge to move the legs that disrupts sleep onset and maintenance. Antihistamines can actually worsen RLS symptoms in some people.
- Hormonal changes: Perimenopause, pregnancy, and thyroid disorders can all disrupt sleep architecture through mechanisms that have nothing to do with histamine.
- Depression and anxiety disorders: These conditions produce insomnia through complex neurochemical pathways involving serotonin, norepinephrine, and cortisol — none of which are addressed by H1 blockade.
This is the fundamental mismatch: doxylamine treats a symptom (inability to fall asleep) by inducing sedation through a single neurotransmitter system, but chronic insomnia is maintained by multiple, interconnected physiological and psychological systems. When the underlying driver is hyperarousal, anxiety, or a sleep disorder, the antihistamine is fighting the wrong battle.

Paradoxical Reactions: When a Sleep Aid Keeps You Awake
A less common but clinically important reason Unisom SleepTabs may appear to "stop working" is that they produce the opposite of the intended effect. Paradoxical reactions to antihistamines — restlessness, agitation, confusion, racing heart, and even increased alertness — are documented in the medical literature. StatPearls notes that doxylamine's anticholinergic properties — its action on muscarinic acetylcholine receptors — are responsible for many of its off-target effects, including central nervous system excitation in susceptible individuals.
Older adults are particularly vulnerable to paradoxical reactions. The Cleveland Clinic advises that people 65 and older may have a stronger reaction to doxylamine and may need a smaller dose. The Harvard Health article on OTC sleep aids specifically warns about confusion and falls in older adults. WebMD user reviews include accounts of paradoxical reactions such as a racing heart and restlessness after taking doxylamine, which users described as making sleep worse rather than better.
Tolerance vs. Therapeutic Failure: How to Tell the Difference
Not every situation where Unisom SleepTabs stop working is the same. Understanding which pattern you are experiencing can guide your next step. The table below outlines three distinct scenarios.
| Pattern | What It Looks Like | Likely Cause | Next Step |
|---|---|---|---|
| Tolerance | The drug worked well for the first 1–2 weeks, then gradually became less effective. You need more to get the same effect. | Receptor upregulation and CNS adaptation to the antihistamine. This is the expected pharmacological response to regular use. | Stop nightly use. Do not increase the dose. Transition to non-pharmacologic approaches like sleep hygiene or CBT-I. |
| Primary failure | The drug never worked well for you, even from the first dose. You experienced minimal sedation or unpleasant side effects. | Individual variation in drug metabolism, receptor sensitivity, or paradoxical reaction. Some people simply do not respond to antihistamines. | Discontinue. This medication is not a good fit for your neurochemistry. Explore other options with a clinician. |
| Therapeutic failure due to worsening root cause | The drug worked initially, but your insomnia has progressively worsened despite continued use. You are sleeping less than when you started. | The underlying driver of your insomnia (anxiety, sleep apnea, depression, hormonal change) has intensified. The antihistamine cannot keep up. | Stop use and see a doctor. This pattern suggests a clinical condition that requires proper diagnosis and targeted treatment. |
If you are unsure whether your sleep difficulties qualify as clinical insomnia or are still in the occasional-sleeplessness category, our triage framework for distinguishing occasional sleep problems from clinical insomnia can help you clarify where you fall on that spectrum.
Long-Term Risks of Continued Use: Beyond Diminishing Returns
Continuing to take Unisom SleepTabs beyond the FDA's two-week limit carries risks that go far beyond the frustration of diminishing effectiveness. These risks accumulate with duration of use and are particularly relevant for anyone who has been taking the medication nightly for months or years.
- Anticholinergic burden: Doxylamine has significant anticholinergic activity — it blocks the neurotransmitter acetylcholine in addition to histamine. Chronic anticholinergic exposure is associated with cognitive decline, memory impairment, and an increased risk of dementia. A 2021 review of 14 cohort studies cited by Healthline found that higher cumulative anticholinergic exposure was linked to increased dementia risk. StatPearls also notes this association signal from observational data.
- Next-day grogginess (hangover effect): Doxylamine has a half-life of approximately 10 hours in healthy adults, extending to 12–15 hours in older adults. This means a significant concentration of the drug remains in your system the next morning, impairing vigilance, coordination, and cognitive performance. The Mayo Clinic specifically warns about this "hangover effect."
- Fall risk in older adults: The combination of sedation, dizziness, and impaired coordination makes doxylamine particularly hazardous for adults 65 and older. The Harvard Health article on OTC sleep aids explicitly flags this risk.
- Urinary retention and constipation: The anticholinergic effects of doxylamine can cause urinary retention (difficulty emptying the bladder) and constipation, which are particularly problematic for older adults and men with prostate enlargement.
For a deeper discussion of why the "non-habit-forming" label on OTC sleep aids can be misleading, see our article on what 'non-habit-forming' actually means — and what it doesn't.
What to Do Next: A Clinical Stepwise Approach
If Unisom SleepTabs have stopped working, the answer is not to increase the dose or switch to another OTC antihistamine. Tolerance will catch up with any drug in this class. Instead, follow this clinical stepwise approach, which aligns with the treatment hierarchy recommended by the American Academy of Sleep Medicine (AASM).
Step 1: Conduct a Sleep Hygiene Audit
Before moving to more intensive interventions, rule out basic environmental and behavioral factors that may be undermining your sleep. This is not a comprehensive solution for chronic insomnia, but it is a necessary foundation.
- Keep a consistent wake time seven days per week, even after a poor night's sleep.
- Avoid caffeine after 2:00 PM and alcohol within three hours of bedtime.
- Ensure your bedroom is dark, quiet, and cool (65–68°F / 18–20°C).
- Stop using screens 60–90 minutes before bed, or use blue-light blocking settings.
- Get at least 15 minutes of natural light exposure within an hour of waking.
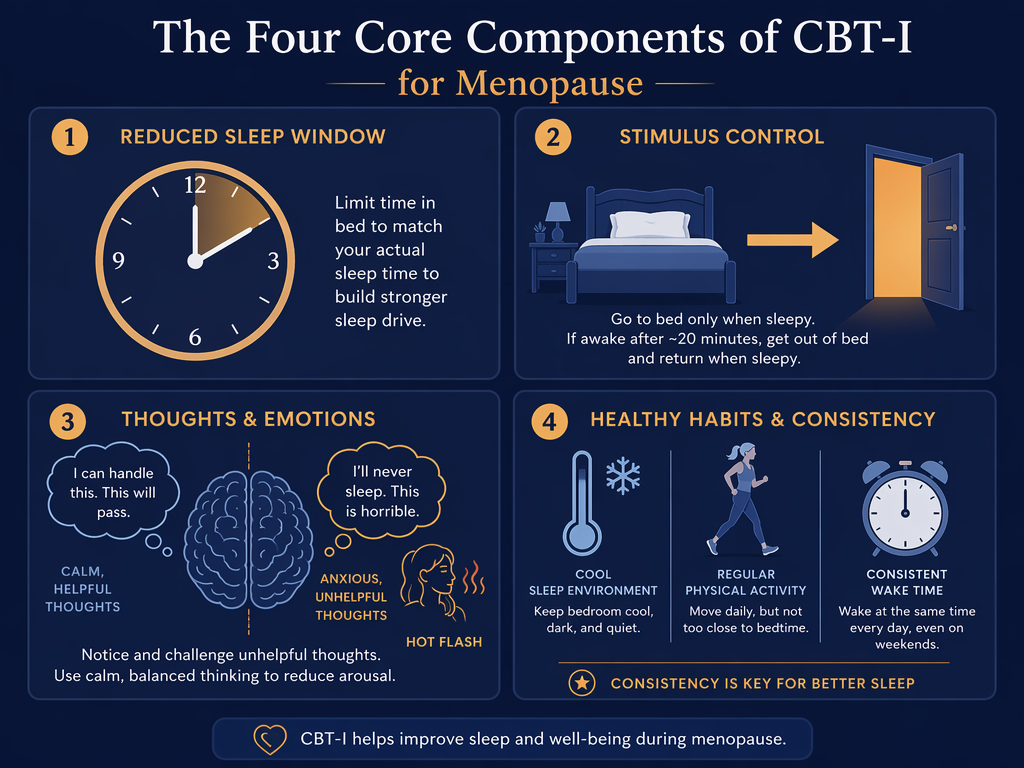
Step 2: Consider CBT-I as First-Line Treatment
Cognitive Behavioral Therapy for Insomnia (CBT-I) is the AASM-recommended first-line treatment for chronic insomnia. Unlike OTC sleep aids, CBT-I addresses the underlying mechanisms that maintain insomnia: conditioned arousal, maladaptive sleep behaviors, and dysfunctional beliefs about sleep. Multiple randomized controlled trials have shown that CBT-I produces durable improvements in sleep latency, sleep efficiency, and total sleep time — outcomes that persist long after treatment ends, which no sleep medication can claim.
For a detailed explanation of how CBT-I works and who it helps, see our CBT-I FAQ. For the latest guideline-based comparison of CBT-I versus medication versus combination therapy, see our 2026 AASM guideline comparison article.
Step 3: Seek Medical Evaluation for Underlying Sleep Disorders
If sleep hygiene improvements and CBT-I are not sufficient — or if you suspect an underlying condition — a medical evaluation is the next step. A clinician can screen for sleep apnea, restless legs syndrome, depression, anxiety disorders, thyroid dysfunction, and other conditions that commonly present as insomnia. The Ubie Health framework recommends screening for sleep apnea, thyroid disease, depression, and RLS as part of the step-up from failed OTC therapy.
Step 4: Explore Prescription Alternatives (With a Doctor)
For patients who need pharmacologic support beyond OTC options, several prescription medications have a stronger evidence base and a more favorable risk profile for long-term use than antihistamines. These include:
| Medication Class | Examples | Mechanism | Key Advantage Over Antihistamines |
|---|---|---|---|
| Low-dose doxepin | Silenor (3–6 mg) | Selective histamine H1 antagonist at low doses | Approved for sleep maintenance; minimal anticholinergic effects at low dose; no tolerance in clinical trials up to 12 weeks |
| Orexin receptor antagonists | Darvidrex, Belsomra, Dayvigo, Quviviq | Blocks orexin, the neurotransmitter that promotes wakefulness | Targets the wakefulness system directly; no GABA activity; lower risk of dependence |
| Melatonin receptor agonists | Ramelteon (Rozerem) | Selective MT1/MT2 receptor agonist | No abuse potential; no tolerance; no next-day grogginess in most patients |
| Sedating antidepressants | Trazodone (25–100 mg), mirtazapine (7.5–15 mg) | Serotonin receptor antagonism with sedative properties | Addresses comorbid depression or anxiety while improving sleep; no tolerance to sedative effect |

Tapering Off Unisom SleepTabs: What to Expect
One concern that keeps people on OTC sleep aids longer than they should is the fear of withdrawal. The good news is that doxylamine does not cause physical dependence in the same way that benzodiazepines or Z-drugs do. There is no opioid-like withdrawal syndrome. However, some people experience rebound insomnia — a temporary worsening of sleep difficulty — when they stop taking the medication, particularly if they have been using it nightly for weeks or months.
A simple tapering approach can minimize this rebound effect:
- If you are taking a full 25 mg tablet, reduce to half a tablet (12.5 mg) for 3–5 nights.
- Then take half a tablet every other night for another 3–5 nights.
- Then stop entirely.
When to See a Doctor
The FDA label for Unisom SleepTabs is clear: stop use and ask a doctor if sleeplessness persists continuously for more than two weeks. Beyond that label directive, here are specific situations that warrant a medical evaluation:
- You have been using any OTC sleep aid nightly for more than 2–4 weeks.
- You experience loud snoring, gasping, or choking during sleep, or your bed partner has observed pauses in your breathing.
- You have an irresistible urge to move your legs in the evening, especially if it interferes with falling asleep.
- You experience excessive daytime sleepiness that makes it difficult to stay awake while driving, working, or in conversations.
- You have symptoms of depression or anxiety — persistent low mood, loss of interest, excessive worry — that may be driving your insomnia.
- You are 65 or older and have been using an anticholinergic sleep aid regularly.
- You want to explore prescription alternatives or a structured CBT-I program.
If you are unsure whether your situation warrants a doctor's visit, our triage framework for distinguishing occasional sleep problems from clinical insomnia can help you make that decision.
Bottom Line: A Framework for Your Next Step
If Unisom SleepTabs have stopped working for you, here is the framework to guide your next move:
- Do not increase the dose. Tolerance will continue to escalate, and higher doses increase the risk of anticholinergic side effects without producing sustainable sleep improvement.
- Respect the two-week boundary. The FDA label's two-week limit is not a suggestion — it is a clinical safety boundary based on the known timeline for tolerance development and the recognition that persistent insomnia requires investigation.
- CBT-I is the first-line treatment. For chronic insomnia, cognitive behavioral therapy has superior long-term outcomes compared to any pharmacologic approach, including prescription medications. It addresses the root causes rather than masking symptoms.
- See a doctor if you have been using OTC sleep aids nightly for more than 2–4 weeks. Persistent insomnia is a medical condition that deserves proper diagnosis and evidence-based treatment, not an escalating cycle of OTC medication use.

Comments
Join the discussion with an anonymous comment.