The sleep-aid question for an older adult usually starts in the medicine cabinet, not in a sleep lab. Someone is awake at 2 a.m., tired of being tired, and the choices look deceptively ordinary: a familiar allergy pill, a “PM” pain reliever, a bottle of melatonin, an old prescription, maybe a newer medication the clinician mentioned. By morning, the same choice can look very different if there is grogginess, a stumble on the way to the bathroom, memory fog at breakfast, or a worried family member trying to sort out which pill was taken.
This is not a rare problem. In 2024, 15.8% of U.S. adults age 65 and older reported using sleep aids regularly, the highest rate among adult age groups in the CDC’s analysis.[1] Among adults 75 and older who used over-the-counter sleep aids, a Gerontological Society of America workgroup reported that 47% used them on 15 or more days per month—well beyond the “occasional use” many product labels imply.[2]
That mismatch matters because aging changes the risk calculation. A medication that merely makes a younger adult sleepy may leave an older adult unsteady, confused, constipated, unable to urinate comfortably, or vulnerable to a prescribing cascade. The 2023 American Geriatrics Society Beers Criteria identifies several common sleep-aid choices—including diphenhydramine, doxylamine, benzodiazepines, and Z-drugs—as potentially inappropriate for many older adults because of safety concerns.[3]

A practical safety hierarchy for sleep aids for elderly adults
The safest way to think about sleep aids for elderly adults is not “natural versus prescription” or “weak versus strong.” A better question is: which option is most likely to improve sleep without worsening cognition, balance, urination, constipation, breathing, or next-day function?
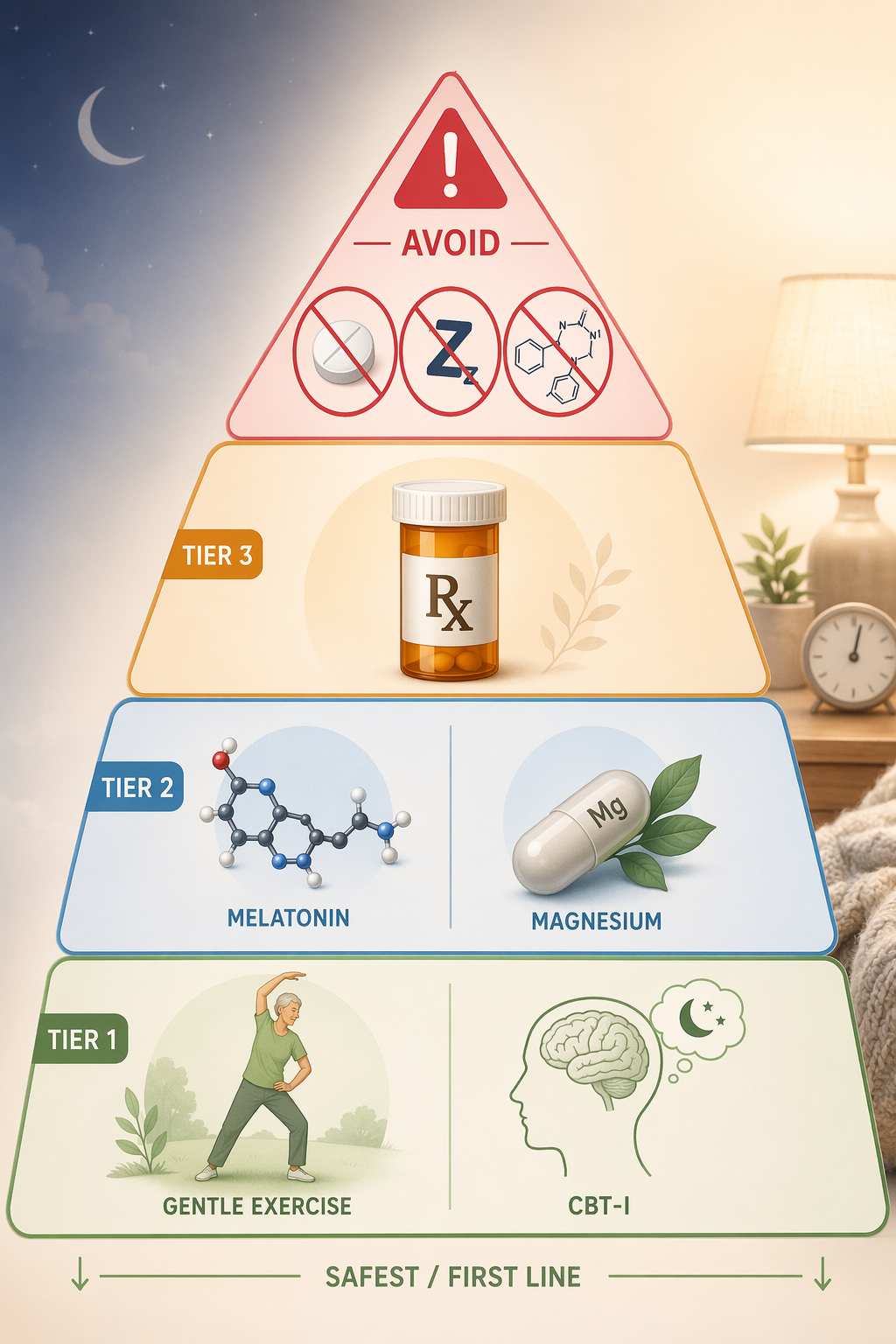
| Safety tier | What belongs here | How to think about it |
|---|---|---|
| Tier 1 | CBT-I, structured exercise, Tai Chi, sleep scheduling work | First-line treatment because there is no medication burden and benefits can last beyond the treatment period |
| Tier 2 | Low-dose melatonin, magnesium glycinate, L-theanine in selected people | Possible short-term bridge, not a cure-all; quality, dose, and interactions still matter |
| Tier 3 | Clinician-guided options such as low-dose doxepin, ramelteon, and dual orexin receptor antagonists | Reasonable when insomnia is persistent or severe and safer choices are selected carefully |
| Avoid list | Diphenhydramine, doxylamine, benzodiazepines, Z-drugs unless there is a compelling individualized reason | Higher geriatric safety concerns, especially next-day impairment, falls, cognition, and dependence |
This hierarchy is not a moral ranking. Severe insomnia can harm health and quality of life, and there are times when medication is appropriate. The point is sequencing: start where the risk is lowest, avoid medications known to cause disproportionate problems in later life, and involve a clinician before a “temporary” solution becomes a nightly routine.
Tier 1: CBT-I and exercise are treatment, not filler
Cognitive behavioral therapy for insomnia, or CBT-I, is often described too casually, as if it were a pamphlet of sleep hygiene reminders. It is more structured than that. CBT-I typically works on the habits and learned associations that keep insomnia going: irregular time in bed, clock watching, conditioned alertness in the bedroom, worry about not sleeping, and long naps that make the next night harder.
The evidence is not perfect, and it should not be oversold. A 2025 umbrella review of 160 randomized controlled trials found that CBT-I reduced sleep-onset latency by about 9 minutes and wake-after-sleep-onset by about 22 minutes in older adults, while exercise therapy—especially Tai Chi—improved Pittsburgh Sleep Quality Index scores by about 1.14 points. Most of the evidence in that review was rated low or very low certainty, which means the exact size of benefit should be treated cautiously.[4]
Even with that caveat, CBT-I belongs at the top of the hierarchy because its benefits do not depend on sedating the brain. A Cleveland Clinic Journal of Medicine review reported that CBT-I has comparable short-term efficacy to pharmacotherapy, with an effect size of 0.96 versus 0.87, and longer-lasting effects.[3] For an older adult, durability matters. A modest improvement that does not add morning confusion or unsteadiness can be more valuable than a stronger sedative effect that creates a problem at 7 a.m.
Structured exercise belongs in the same first-line tier for similar reasons. It is not an instant sleeping pill. It may take time, and it has to fit the person’s mobility, pain level, cardiac status, and fall risk. But when it is chosen sensibly—walking, supervised balance work, gentle strength training, Tai Chi, or another realistic routine—it can support sleep while also helping the very systems that sedating medications often endanger: gait, balance, mood, and daytime function.
For families, this is the part that often needs reframing. CBT-I and exercise are not what you try after the “real” sleep aids fail. They are the place to start precisely because older adults are more likely to pay for sedation with falls, delirium, memory complaints, and medication complications.
What this looks like in ordinary life
A practical first-line plan might involve setting a consistent wake time, reducing long daytime naps, getting morning light, using the bed only for sleep and intimacy, leaving the bed briefly when unable to sleep, and adding safe daytime activity. Those steps sound plain, but plain is not the same as weak. They target the rhythm and conditioning problems that keep insomnia alive without adding another drug to a medication list.
The hard part is that behavioral treatment asks for patience at the exact moment people want immediate relief. That is where a clinician, CBT-I program, sleep psychologist, or well-designed digital CBT-I program can help. The goal is not to lecture someone into better sleep. It is to reduce the need to gamble with medications that may solve midnight and create morning.
Tier 2: cautious OTC bridges, with melatonin handled carefully
If behavioral steps are underway and sleep is still poor, some over-the-counter options may be reasonable as short-term bridges. “Over the counter” does not automatically mean safe, and “natural” does not automatically mean effective. The better OTC candidates are the ones least likely to impair balance, cognition, or breathing when used at conservative doses.
Melatonin: lower dose, clearer expectations
Melatonin is often the first supplement people reach for, and it is usually a safer discussion than diphenhydramine or doxylamine. The best evidence in older adults is not for high-dose U.S. gummy products. A 2021 American Family Physician review reported that 2 mg prolonged-release melatonin reduced sleep-onset latency by 14 to 16 minutes in older adults, with adverse event rates comparable to placebo.[5]
That finding should be kept in its lane. Much of the stronger evidence involves prolonged-release formulations, while many U.S. OTC melatonin products are immediate-release and may vary in potency. A practical low-dose range often used for older adults is 0.5 to 3 mg, especially when the main problem is falling asleep or a shifted sleep schedule. More is not necessarily better; higher doses may increase next-day grogginess, vivid dreams, or confusion in sensitive people.
Melatonin also needs a medication-list check. People taking anticoagulants, diabetes medications, immunosuppressants, seizure medications, or multiple sedating drugs should ask a clinician or pharmacist before adding it. The question is not whether melatonin is “gentle” in the abstract. The question is whether it is gentle for this person, with this medication list, this fall risk, and this morning routine.
Magnesium glycinate and L-theanine: possible, not proven cures
Magnesium glycinate and L-theanine are sometimes reasonable to discuss when the goal is a low-risk bridge, particularly for people who want to avoid sedating antihistamines. They should not be presented as proven insomnia cures. Magnesium can cause diarrhea, may be unsafe in significant kidney disease, and can interfere with absorption of some medications if taken too close together. L-theanine may be calming for some people, but the evidence base for treating insomnia in older adults is limited.
For OTC supplements, the safest approach is conservative: one change at a time, the lowest reasonable dose, a clear stop date, and a note in the medication list. If a supplement is used nightly for weeks and the sleep problem is unchanged, continuing it out of habit is not harmless simply because it came from a health-food aisle.
Tier 3: safer prescription options can be appropriate
Prescription medication is not automatically the dangerous category, just as OTC medication is not automatically the safe one. The safer prescription options for older adults are usually those chosen deliberately for the person’s sleep pattern, medical conditions, fall risk, and current medications—not old sedatives refilled indefinitely because they “worked.”
Low-dose doxepin is one example. At antidepressant doses, doxepin can have anticholinergic effects, but at very low insomnia doses it behaves differently. The Cleveland Clinic Journal of Medicine review cited a 12-week trial in which low-dose doxepin, in the 1 to 3 mg range, improved sleep without anticholinergic effects or memory problems.[3] In practice, clinicians often consider low-dose doxepin for sleep-maintenance insomnia—waking during the night or too early—rather than as a general sedative.
Ramelteon is another clinician-guided option, especially when the main issue is falling asleep. It works through melatonin receptors rather than by broadly sedating the central nervous system. It still needs individualized review, but it does not carry the same dependence profile as benzodiazepines.
Dual orexin receptor antagonists, or DORAs, such as lemborexant and daridorexant, are also part of the safer modern prescription conversation. In the same review, lemborexant had a reported number needed to treat of 3, while daridorexant 50 mg had a reported number needed to harm of 78, suggesting a favorable risk-benefit profile in the data reviewed.[3] These drugs are not free of next-day impairment concerns, cost issues, or interaction questions, but they are a different category from older sedatives that simply push the brain toward generalized sedation.
The clinical boundary is important: if insomnia is persistent, severe, associated with depression or anxiety, linked to pain, worsened by nighttime urination, or accompanied by snoring and breathing pauses, the answer is not to keep climbing the OTC shelf. The sleep problem may be a symptom, and the safest “sleep aid” may be treating the condition that is waking the person up.
The avoid list: familiar does not mean safe
The most important safety advice in older-adult insomnia may be what not to take casually. Many people worry about prescription sleeping pills while feeling comfortable with Benadryl, Unisom, “PM” combination products, or an old benzodiazepine in the bathroom drawer. That confidence is misplaced.
Diphenhydramine and doxylamine
Diphenhydramine and doxylamine are first-generation antihistamines. They are common in OTC sleep products, allergy products, and combination pain relievers labeled for nighttime use. Their problem in older adults is not just sleepiness. They add anticholinergic burden, which can worsen confusion, dry mouth, constipation, urinary retention, blurred vision, and next-day impairment.
Diphenhydramine also lasts longer in older bodies. The Cleveland Clinic Journal of Medicine review cites pharmacokinetic data showing a half-life of about 13.5 hours in elderly adults versus about 9.2 hours in younger adults.[3] A pill taken at 11 p.m. can still be relevant when someone is getting up at 7 a.m., navigating the bathroom, making coffee, or driving to an appointment.
The GSA workgroup also noted an uncomfortable regulatory history: OTC sleep aids such as diphenhydramine and doxylamine were grandfathered before the FDA’s 1972 monograph process and were not required to demonstrate efficacy in modern randomized controlled trials.[2] That does not mean they never make anyone sleepy. It means long familiarity should not be confused with strong modern evidence or geriatric safety.
Benzodiazepines
Benzodiazepines such as temazepam, lorazepam, alprazolam, clonazepam, and diazepam are sometimes inherited from years of “just for sleep” prescribing. In older adults, they are associated with sedation, cognitive impairment, delirium, falls, fractures, motor vehicle crashes, and dependence concerns; the Beers Criteria lists benzodiazepines as potentially inappropriate for older adults.[3]
They also become difficult to unwind. A person may start with occasional use, then use the medication after several bad nights, then feel unable to sleep without it. Stopping suddenly can be unsafe. If a benzodiazepine has become part of a nightly routine, the next step is not a stern lecture or abrupt discontinuation. It is a tapering plan supervised by a clinician.
Z-drugs
Z-drugs, including zolpidem, zaleplon, and eszopiclone, were often marketed as cleaner sleep medications than benzodiazepines. For older adults, that distinction is not reassuring enough. The Beers Criteria also identifies Z-drugs as potentially inappropriate because they can cause problems such as delirium, falls, fractures, emergency visits, motor vehicle crashes, and limited improvement in sleep latency and duration.[3]
The pattern is familiar: the pill helps someone fall asleep, but the household pays attention to the aftermath—unsteadiness, odd nighttime behavior, morning grogginess, or worsening memory complaints. A medication that improves one sleep metric while making the next day less safe is a poor bargain.
Major health organizations continue to warn against routine sleeping-pill use in older adults. Choosing Wisely Canada reports that nearly 1 in 3 older adults in Canada take sleeping pills despite guidelines against routine use.[7] Mayo Clinic similarly cautions that sleep aids can pose particular risks for people over 65, including concerns about falls, confusion, and dementia risk.[6]
When to stop self-treating
Self-treatment should stay brief and modest. An older adult should involve a clinician promptly if insomnia lasts for weeks, causes daytime sleepiness or falls, follows a new medication change, appears with depression or anxiety, or comes with loud snoring, gasping, restless legs, worsening pain, nighttime confusion, or frequent urination. The same is true when someone is already taking several medications, drinks alcohol in the evening, has memory impairment, has kidney or liver disease, or has had recent falls.
A useful medication review asks more than “what sleeping pill do you take?” It should include allergy pills, nausea medicines, bladder medicines, muscle relaxants, pain relievers, cannabis products, alcohol, supplements, and any “PM” product. Many older adults do not think of diphenhydramine as a sleep medication if it is hidden inside a combination product.
The safest sleep aid for an older adult is not the strongest sedative. It is the option that improves sleep without worsening cognition, balance, or next-day function. For many people, that means CBT-I and safe exercise first, cautious low-dose OTC options only if needed, and safer prescription choices only with medical guidance—while keeping first-generation antihistamines, benzodiazepines, and Z-drugs off the casual-use list.
References
- Use of Sleep Aids Among Adults Age 18 and Older: United States, 2024, CDC National Center for Health Statistics, April 2026.
- Sleep Health and Appropriate Use of OTC Sleep Aids in Older Adults, Gerontological Society of America.
- Insomnia in older adults: A review of treatment options, Cleveland Clinic Journal of Medicine, January 2025.
- Non-pharmacological interventions for sleep in older adults: an umbrella review.
- Melatonin for the Treatment of Insomnia in Older Adults, American Family Physician, 2021.
- Sleep aids: Understand options sold without a prescription, Mayo Clinic, January 2026.
- Sleeping pills and older adults, Choosing Wisely Canada.


Comments
Join the discussion with an anonymous comment.