Why Morning Back Pain Isn't Random
Low back pain is a near-universal human experience. It affects up to 85% of adults at least once in their lives, and roughly 16 million Americans live with chronic back pain. For many, the pain is most pronounced in the morning — a stiff, achy feeling that fades after getting up and moving around. The common assumption is that this is simply a consequence of aging, a soft mattress, or "sleeping wrong." But the evidence points to a more specific, measurable mechanism: sustained provocative sleep postures cause micro-damage to spinal tissues within minutes, and that damage accumulates over the course of the night.
The idea that a single night of poor posture could produce measurable tissue-level injury is counterintuitive. Most people assume that the body fully recovers during sleep, or that pain upon waking is a sign of an underlying condition flaring up. The research tells a different story. A 2021 cross-sectional study by Cary et al. used infrared video to monitor participants over two nights in their own homes and found that those who woke with cervical symptoms spent more than double the amount of time in provocative postures compared to asymptomatic controls. The difference was not subtle — it was a matter of hours per night.
What Happens to Spinal Tissues During Sustained Postures
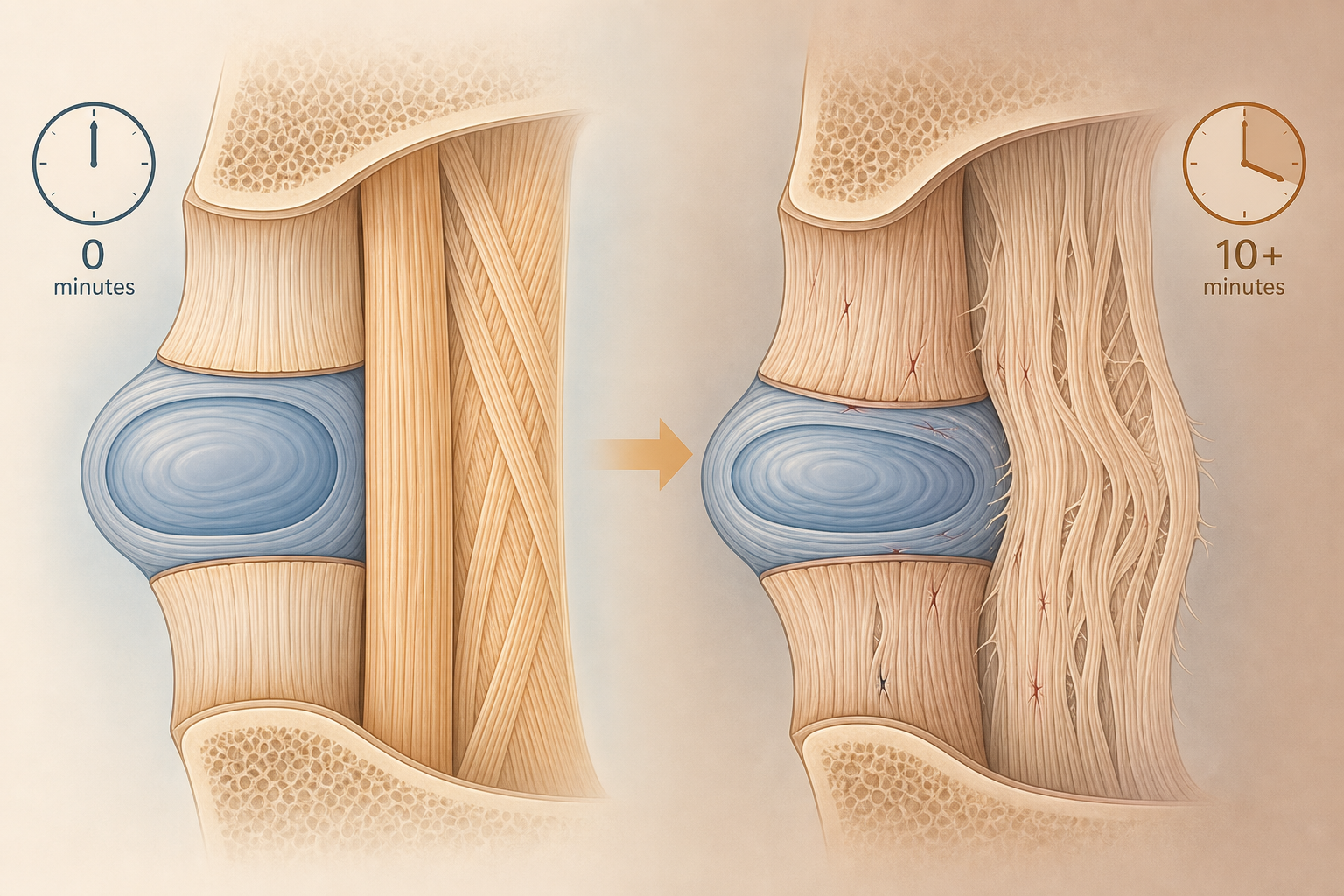
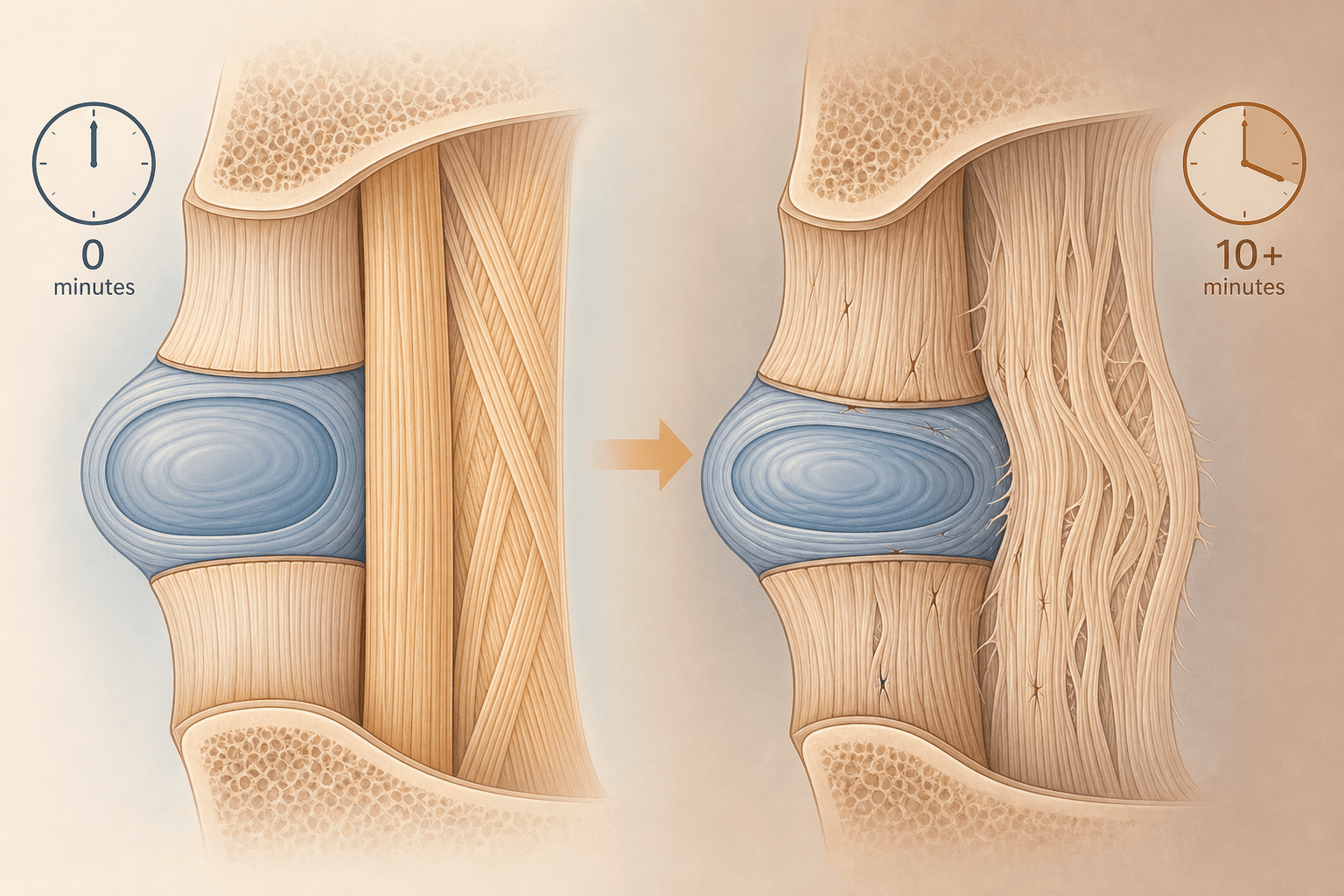
The spine is held together by a complex network of collagenous tissues — ligaments, tendons, intervertebral discs, and facet joint capsules. These tissues are viscoelastic, meaning they deform under sustained load and do not immediately return to their original shape when the load is removed. This property is called creep. When you lie in a position that places a ligament or disc under tension — for example, sleeping on your stomach with your neck rotated to one side — the tissue begins to elongate. After approximately 10 minutes of sustained load, the elongation can exceed 3%, a threshold at which collagen fibers begin to experience micro-damage.
This is not theoretical. The Cary et al. study explicitly references the 10-minute threshold and the 3% elongation figure, drawing on animal-model research showing that loads exceeding this level are associated with increased expression of pro-inflammatory cytokines. In plain terms: when you hold a provocative posture long enough, you are not just uncomfortable — you are triggering a low-grade inflammatory response in the spinal tissues. That inflammation is what you feel as stiffness, achiness, or sharp pain when you wake up.
The clinical significance of this mechanism is that it decouples sleep posture from sleep duration. You can sleep for eight hours and still wake up in pain if a significant portion of that time was spent in a provocative position. Conversely, a shorter night of sleep with better posture may produce less morning pain. This reframes the problem: it is not about how long you sleep, but about how you are positioned during the vulnerable periods of sustained immobility.
Evidence from Video-Monitored Sleep: The Cary et al. 2021 Study
The strongest direct evidence linking sustained sleep postures to waking spinal symptoms comes from the Cary et al. study, published in 2021. The study enrolled 53 participants and used infrared video cameras to record sleep posture over two nights in the participants' own bedrooms — a naturalistic setting that avoids the artificial constraints of a sleep lab. The researchers then correlated the video data with morning symptom reports.
| Metric | Cervical Symptom Group | Control Group |
|---|---|---|
| Time in provocative postures (median) | 185.1 minutes | 83.8 minutes |
| Frequency of posture changes (mean) | 23.6 | 18.3 |
| Long immobility periods in provocative postures (median) | 2.0 | 0.5 |
| PSQI sleep quality score | 7.4 | 3.2 |
The cervical symptom group spent a median of 185.1 minutes per night in provocative postures — more than double the 83.8 minutes observed in the control group. They also changed positions more frequently (23.6 vs. 18.3 changes per night) and had more extended periods of immobility in provocative postures (median 2.0 vs. 0.5). The sleep quality scores tell a parallel story: the cervical group had a mean PSQI score of 7.4, well above the clinical threshold for poor sleep, compared to 3.2 in controls.
Despite this limitation, the study provides a critical insight: the relationship between sleep posture and morning pain is not about a single bad position. It is about cumulative exposure. The cervical group did not simply adopt one terrible posture and hold it all night. They spent long stretches in provocative positions, moved more often (suggesting discomfort-driven shifting), and had more prolonged immobility in those positions. This pattern — not a single posture, but a night-long accumulation of micro-damage — is the mechanism that explains why morning pain feels diffuse and positional rather than localized to a single movement.
Position-by-Position Mechanical Analysis
Each sleep position imposes a different mechanical load profile on the spine. Understanding these profiles — not just memorizing which position is "best" — is what allows you to make informed adjustments. The following analysis focuses on how each position affects tissue loading and micro-damage risk.
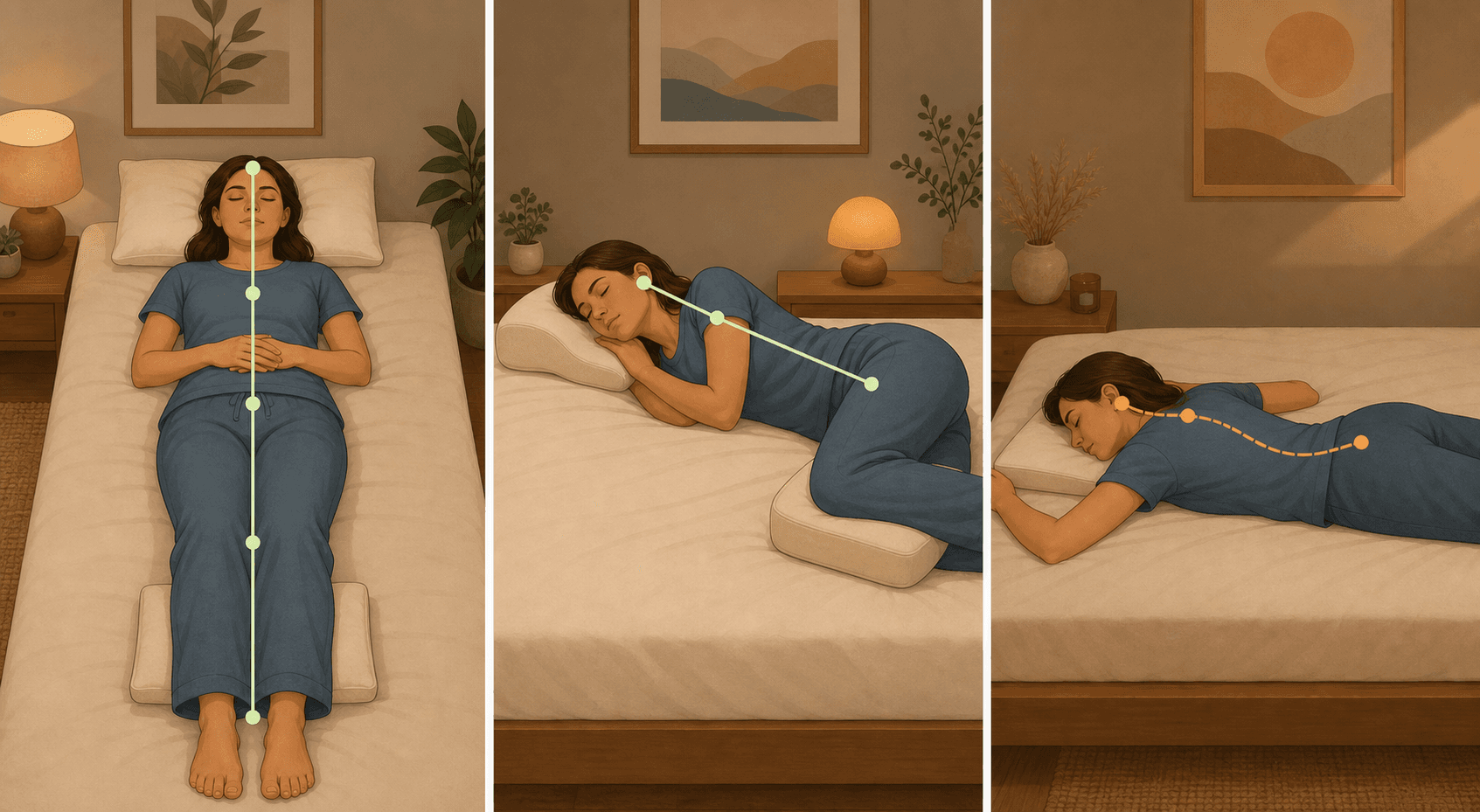
Supine (Back Sleeping)
According to the American Chiropractic Association, sleeping on your back places approximately 50 pounds of pressure on the spine. This is not inherently problematic — the spine is designed to bear load — but the distribution of that load matters. In a neutral supine position with a pillow under the knees, the lumbar curve is supported and the weight is distributed evenly across the posterior chain. Without knee support, the lower back may arch excessively, increasing disc pressure and straining the facet joints.
For most people, back sleeping with a pillow under the knees is the mechanically optimal position. It allows the spine to maintain its natural S-curve, minimizes disc pressure, and avoids the neck rotation required by side or stomach sleeping. However, it is not suitable for everyone. Individuals with obstructive sleep apnea or GERD may find that back sleeping worsens their symptoms. For those readers, a decision framework for back sleeping is available to weigh the trade-offs.
Side Lying
Side sleeping is the most common adult sleep position, and it can be mechanically sound — but only with the right support. The key variable is the width of the shoulder. When you lie on your side, the distance from your ear to the mattress surface is determined by your shoulder width. If your pillow is too low, your neck drops into lateral flexion, stretching the tissues on the upper side and compressing them on the lower side. If your pillow is too high, your neck is pushed into lateral flexion in the opposite direction.
The National Spine Health Foundation reports that placing a pillow between the knees can reduce spinal pressure by nearly half. This works by preventing the top leg from dropping forward, which would otherwise rotate the pelvis and create torque through the lumbar spine. A contoured pillow designed for side sleepers — one that matches the shoulder-to-ear distance — is the recommended choice for maintaining neutral cervical alignment.
Prone (Stomach Sleeping)
Stomach sleeping is consistently described by medical institutions — including Mayo Clinic, Keck Medicine of USC, and Henry Ford Health — as the least back-friendly position. The mechanical problem is twofold. First, lying prone flattens the natural lumbar curve, placing the lower back in extension and increasing pressure on the facet joints. Second, because you cannot breathe face-down, you must rotate your neck to one side, holding the cervical spine in sustained rotation for hours at a time.
This combination — lumbar extension plus cervical rotation — is a direct recipe for the tissue creep mechanism described earlier. The neck rotation alone can exceed the 3% elongation threshold within minutes, and the lumbar extension adds a second site of potential micro-damage. If you are a committed stomach sleeper, the best mitigation is to place a thin pillow under the lower abdomen or hips to reduce the lumbar arch, and use a very flat pillow (or no pillow) under the head to minimize neck rotation.
Practical Application: Pillow Mapping, Mattress Firmness, and the Log-Roll Technique
Understanding the tissue creep mechanism is only useful if it translates into actionable changes. The following recommendations are drawn from the mechanical analysis above and are consistent across multiple medical institutions.
Pillow Mapping by Position
- Back sleepers: Use a flatter, contoured pillow that supports the natural curve of the cervical spine without pushing the head too far forward. Place a second pillow under the knees to maintain the lumbar curve.
- Side sleepers: Use a taller, contoured pillow that fills the gap between the ear and the mattress (matching your shoulder width). Place a pillow between the knees to keep the pelvis and spine aligned.
- Stomach sleepers: Use a very thin pillow or no pillow under the head. Place a small, flat pillow under the lower abdomen or hips to prevent the lower back from sagging into extension.
Mattress Firmness
Multiple sources — including the National Spine Health Foundation, Hospital for Special Surgery, and Henry Ford Health — recommend a medium-firm mattress for back pain. The reasoning is mechanical: a mattress that is too soft allows the hips and shoulders to sink, creating a hammock effect that misaligns the spine. A mattress that is too firm creates pressure points and does not accommodate the natural curves. A medium-firm mattress provides enough support to maintain alignment while allowing enough give to distribute pressure.
A simple test: lie on your back on the mattress. If your lower back sinks below the level of your shoulders and feet, the mattress is too soft. If you feel excessive pressure on your hips and shoulders, it is too firm. The National Spine Health Foundation also recommends replacing mattresses every 7–10 years, as foam and spring support degrade over time.
The Log-Roll Technique
Getting in and out of bed is a moment of high spinal torsion risk, especially for people with existing back pain. The log-roll technique minimizes this risk by keeping the spine in a neutral, aligned position throughout the movement. The National Spine Health Foundation and the Advanced Spine Center both describe the same sequence: roll onto your side as a single unit (keeping your shoulders and hips aligned), then use your arms to push your upper body upright while simultaneously swinging your legs off the bed. Reverse the sequence when lying down.
The Bidirectional Relationship Between Sleep Quality and Back Pain
The relationship between sleep and back pain is not one-directional. Poor sleep lowers pain thresholds, making the same mechanical load feel more painful. And provocative sleep postures degrade sleep quality — the Cary et al. study found that participants with morning symptoms had significantly worse PSQI scores (7.4 vs. 3.2), indicating clinically meaningful sleep disruption. This creates a feedback loop: pain disrupts sleep, poor sleep amplifies pain sensitivity, and the provocative postures that caused the pain in the first place continue night after night.
The National Spine Health Foundation notes that chronic sleep deprivation is associated with increased sensitivity to pain, and that long-term poor sleep quality contributes to a substantially increased risk of chronic and disabling back pain. This means that posture retraining is not just about protecting your spine — it is also about protecting your sleep. When you reduce the time spent in provocative postures, you reduce both the mechanical micro-damage and the sleep disruption that amplifies pain perception.
For a broader exploration of how sleep position affects overall sleep quality — including airway patency, GERD, and glymphatic clearance — see our companion article: How Sleep Position Affects Sleep Quality and Health.
Key Takeaways
- Morning back pain is not random. Sustained provocative sleep postures cause measurable collagenous tissue micro-damage within 10 minutes, and this damage accumulates over the night.
- The Cary et al. 2021 study provides direct evidence: participants with morning cervical symptoms spent 185 minutes per night in provocative postures vs. 84 minutes in controls, and had more frequent posture changes and longer immobility periods.
- Back sleeping with a pillow under the knees is mechanically optimal for most people. Side sleeping requires a contoured pillow matching shoulder width and a pillow between the knees. Stomach sleeping should be avoided or mitigated with a thin hip pillow.
- A medium-firm mattress provides the best balance of support and pressure distribution. Replace mattresses every 7–10 years.
- The log-roll technique for getting in and out of bed prevents spinal torsion and is especially important for those with acute back pain.
- Sleep quality and back pain are bidirectional. Improving sleep posture can interrupt the cycle of pain-disrupted sleep and sleep-amplified pain.
Comments
Join the discussion with an anonymous comment.