

Why Flat Tip Lists Fail Most Readers
If you have searched for "ways to sleep better" before, you have likely encountered the same pattern: a list of 10 to 15 tips, each given roughly equal weight. Keep a consistent schedule. Avoid caffeine. Exercise. Try melatonin. Keep your room cool. The problem with this format is not that the tips are wrong — many are correct — but that it collapses interventions of vastly different evidence strength into a single, undifferentiated column. Stimulus control therapy, which is supported by decades of randomized controlled trials, sits next to a suggestion to buy blackout curtains, which is supported by observational data. Melatonin, which a 2023 analysis found to be inaccurately labeled in 88% of products, sits next to a recommendation to reduce screen time, which has strong mechanistic backing. This flat presentation leaves readers without a way to prioritize. It also creates the false impression that if none of the 15 tips worked, nothing will.
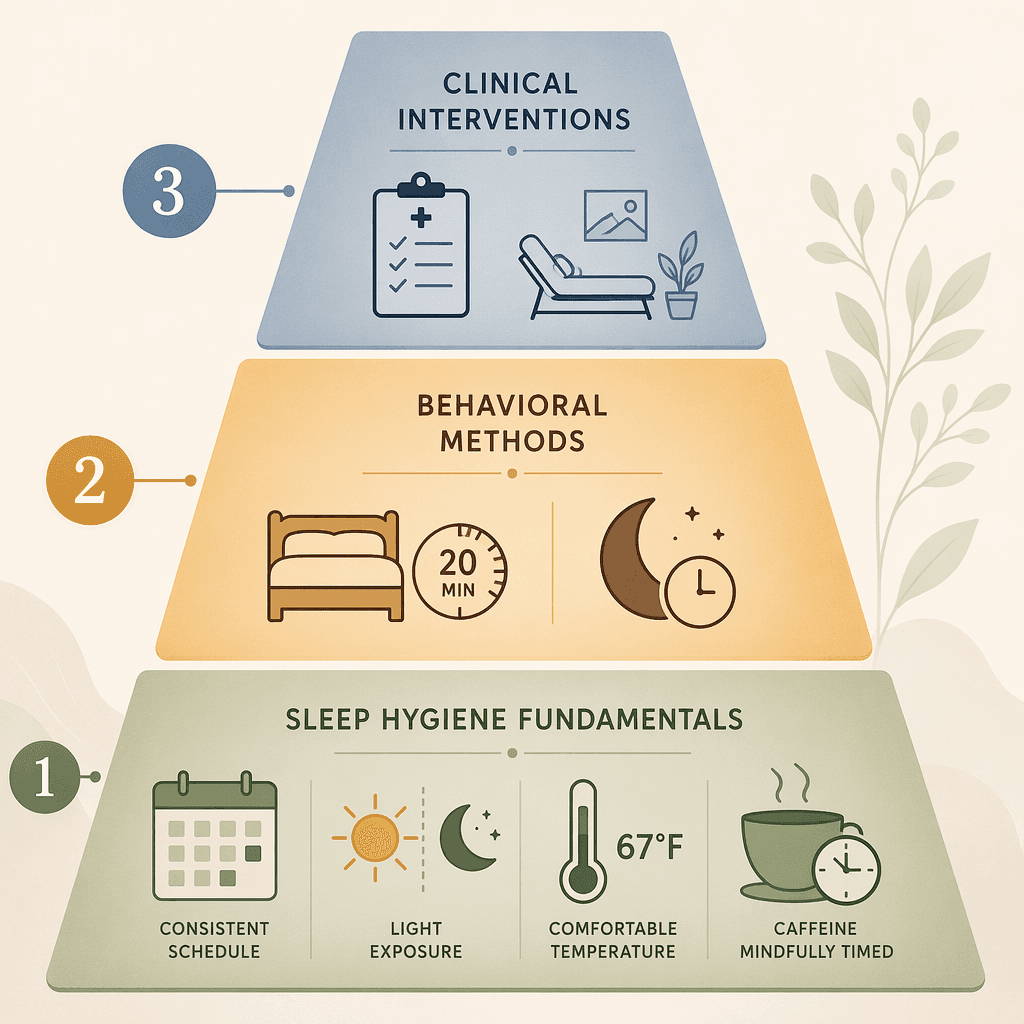
The reality is different. Sleep improvement follows a hierarchy of evidence. Some interventions have broad, consistent support across large populations and should be tried first. Others are more specific, require more consistency, or target particular mechanisms and should be tried second. A third group involves clinical assessment and should be pursued only when the first two tiers have been given a fair trial. This article organizes that hierarchy into three tiers so you can match your effort to the strength of the evidence and know when it is time to escalate.
Tier One: Sleep Hygiene Fundamentals — Broadest Evidence, First-Line for Everyone
Tier One contains the interventions with the widest research support and the lowest cost or risk. These are the changes that should be in place for every adult before considering anything else. They address the basic physiological and environmental conditions that the human sleep system requires to function properly.
Consistent Sleep-Wake Schedule
The single most impactful sleep hygiene practice is going to bed and waking up at roughly the same time every day, including weekends. This stabilizes the circadian rhythm, which is the internal biological clock that regulates the timing of sleep and wakefulness. When the schedule shifts by more than an hour on weekends — a pattern sometimes called "social jet lag" — the circadian system loses its anchor, and sleep onset and morning alertness both suffer. The target is at least seven hours in bed for adults, though individual needs vary.
For a deeper understanding of the biological mechanisms behind this recommendation, see our guide on circadian rhythm mechanisms.
Light-Dark Cycle Management
Light is the primary external cue that sets the circadian clock. Morning sunlight exposure — ideally within 30 to 60 minutes of waking — signals the brain to suppress melatonin production and shift into daytime mode. Evening exposure to artificial light, particularly the short-wavelength blue light emitted by screens, delays melatonin onset and makes it harder to fall asleep. The practical recommendation is to seek bright light early in the day and dim lights in the hour before bed. Research cited in the Global Wellness Institute's 2026 trends report (Gooley et al., 2011) confirms that room light at night suppresses melatonin onset, which directly affects sleep timing.
Thermal Environment: 65–68°F
The body's core temperature naturally drops by about one to two degrees Fahrenheit to initiate and maintain sleep. A bedroom that is too warm interferes with this thermoregulatory process. The Sleep Foundation, Harvard Health, and the Global Wellness Institute (citing Basner et al., 2023) all converge on a recommended bedroom temperature range of 65 to 68°F (18.3 to 20°C). This is not a comfort preference — it is a physiological requirement for efficient sleep onset and maintenance.
Caffeine Cutoff: 8+ Hours Before Bed
Caffeine is a competitive antagonist of adenosine receptors — it blocks the chemical that builds sleep pressure throughout the day. The half-life of caffeine in most adults is roughly five to six hours, meaning that a 2:00 PM coffee still leaves a quarter of its active dose in your system at 10:00 PM. A 2023 review cited by Healthline found that consuming caffeine as early as eight hours before bedtime reduced total sleep time by an average of 45 minutes and sleep efficiency by 7%. For most people, this means a caffeine cutoff around 1:00 or 2:00 PM, depending on individual sensitivity and metabolism.
The 3-2-1 Rule as a Practical Timing Framework
Several consumer-facing sources, including the Sleep Foundation and Healthline, describe a 3-2-1 rule as a memory aid for evening timing: stop alcohol three hours before bed, stop food two hours before, and stop liquids one hour before. Alcohol is particularly problematic because, although it can hasten sleep onset, it fragments sleep in the second half of the night and reduces REM sleep duration. This rule is a practical guideline, not a rigorously tested clinical protocol, but it aligns well with the physiological timing of digestion and metabolism.
For a complete walkthrough of building these fundamentals into a structured routine, see our evidence-based bedtime routine guide.
Tier Two: Behavioral Methods When Fundamentals Aren't Enough
For many people, consistent application of Tier One changes produces noticeable improvement within two to four weeks. If it does not — or if improvement plateaus — the next step is behavioral methods with strong randomized controlled trial support. These methods target the conditioned associations and behavioral patterns that maintain poor sleep, even after the original triggers have resolved.
Stimulus Control Therapy
Stimulus control is one of the core components of Cognitive Behavioral Therapy for Insomnia (CBT-I) and has strong independent evidence. The logic is straightforward: the bed and bedroom should become a strong cue for sleep, not for wakefulness. When you spend extended time in bed awake — worrying, scrolling, or simply lying there frustrated — your brain learns to associate the bed with arousal rather than rest. Stimulus control breaks this association through a set of rules:
- Go to bed only when you are sleepy.
- If you are unable to fall asleep within approximately 20 minutes, get out of bed. Return to bed only when you feel sleepy again.
- Use the bed only for sleep and sex. No reading, watching TV, working, or scrolling.
- Get out of bed at the same time every morning, regardless of how much sleep you got the night before.
- No napping during the day.
The 20-minute rule is the most frequently misunderstood part of stimulus control. It is not a strict timer. The instruction is to leave the bedroom when you recognize that you are not falling asleep and are beginning to feel frustrated or alert. Lying in bed awake for an hour while watching the clock defeats the purpose. For a full explanation of the conditioning logic behind each rule, see our stimulus control therapy guide.
Sleep Restriction Therapy
Sleep restriction therapy addresses a different problem: spending too much time in bed relative to actual sleep time, which fragments sleep and reduces its depth. The intervention is counterintuitive — it initially limits the time spent in bed to match the average total sleep time, creating mild sleep deprivation that consolidates sleep and increases sleep drive. Over several weeks, the time in bed is gradually expanded as sleep efficiency (the percentage of time in bed spent asleep) improves above 85–90%.
This method produces measurable improvement in sleep continuity within two to four weeks, but it requires careful tracking and adherence. It is not appropriate for individuals with a history of mania, seizure disorders, or certain medical conditions. If you try sleep restriction and encounter stalls or difficulties, our sleep restriction troubleshooting guide covers the most common obstacles and how to adjust.
| Method | Core Mechanism | Typical Time to Effect | Best Suited For |
|---|---|---|---|
| Stimulus control | Re-associates bed with sleep, not wakefulness | 2–4 weeks | Difficulty falling asleep; conditioned arousal |
| Sleep restriction | Consolidates sleep window to improve efficiency | 2–4 weeks | Fragmented sleep; spending too long in bed awake |
| Relaxation techniques | Reduces physiological arousal before bed | 1–2 weeks | Anxiety-driven sleep onset delay; racing thoughts |
Tier Three: Clinical Interventions for Persistent Sleep Problems
If you have applied Tier One and Tier Two methods consistently for four to six weeks and still experience significant sleep disruption — difficulty falling asleep most nights, waking frequently and unable to return to sleep, or waking unrefreshed despite adequate time in bed — it is appropriate to consider clinical evaluation. This tier involves interventions that require professional guidance or diagnostic assessment.
CBT-I: The Gold Standard for Chronic Insomnia
Cognitive Behavioral Therapy for Insomnia (CBT-I) is the first-line treatment recommended by the American Academy of Sleep Medicine (AASM) for chronic insomnia. It is a multi-component intervention that combines stimulus control, sleep restriction, cognitive restructuring (addressing unhelpful beliefs about sleep), and sometimes relaxation training. Unlike sleep medications, CBT-I targets the underlying behavioral and cognitive mechanisms that maintain insomnia.
The evidence base is substantial. A 2021 meta-analysis by Scott et al. published in Sleep Medicine Reviews analyzed 65 randomized controlled trials with 8,608 participants and found that improving sleep quality produced medium-sized effects on depression (g+ = −0.63), anxiety (g+ = −0.51), and stress (g+ = −0.42). The most common intervention across these trials was CBT-I, used in 74% of studies. Importantly, the review found a dose-response relationship: greater improvements in sleep led to greater improvements in mental health, and the effect was significant regardless of whether participants had physical or mental health comorbidities.
For readers interested in self-directed CBT-I techniques before or alongside seeking professional help, our self-directed CBT-I guide provides a structured overview of the core components and how to implement them.
When to Consider Sleep Apnea Testing
Not all persistent sleep problems are insomnia. Loud snoring, witnessed pauses in breathing during sleep, gasping or choking at night, excessive daytime sleepiness despite adequate sleep time, and morning headaches are all potential indicators of obstructive sleep apnea. The home sleep apnea testing market is projected to grow to $966.1 million by 2035, according to the Global Wellness Institute's 2026 trends report, reflecting a shift toward accessible diagnostic tools. If you have any of these symptoms, a clinical evaluation — not self-directed behavioral methods — is the appropriate next step.
How to Self-Triage: A Decision Framework for Choosing Your Next Step
The following table maps common sleep complaints to the most appropriate starting tier and specific intervention. Use it to identify where to begin, but remember that the tiers are sequential: start with Tier One, give it two to four weeks of consistent application, and escalate only if improvement is insufficient.
| Your Primary Complaint | Start With | Specific Intervention | How Long to Try Before Escalating |
|---|---|---|---|
| Difficulty falling asleep | Tier One | Consistent schedule, caffeine cutoff, evening wind-down routine | 2–4 weeks |
| Difficulty falling asleep (persistent) | Tier Two | Stimulus control (20-minute rule, bed for sleep only) | 4–6 weeks |
| Waking frequently during the night | Tier One | Thermal environment (65–68°F), alcohol avoidance, light management | 2–4 weeks |
| Waking frequently (persistent) | Tier Two | Sleep restriction therapy to consolidate sleep window | 4–6 weeks |
| Waking too early and unable to return to sleep | Tier One | Morning light exposure to advance circadian timing | 2–4 weeks |
| Waking too early (persistent) | Tier Two | Stimulus control + sleep restriction combination | 4–6 weeks |
| Feeling unrefreshed despite adequate time in bed | Tier One | Schedule consistency, sleep duration check (7+ hours) | 2–4 weeks |
| Feeling unrefreshed (persistent) + snoring or gasping | Tier Three | Clinical evaluation for sleep apnea; home sleep apnea testing | Seek evaluation promptly |
| Anxiety or racing thoughts at bedtime | Tier One + Tier Two | Relaxation techniques, stimulus control, cognitive restructuring | 4–6 weeks |
| Shift work or jet lag | Tier One | Timed light exposure, strategic napping, consistent anchor schedule | 1–2 weeks per shift change |
The Resmed 2026 Global Sleep Survey, which surveyed 30,000 individuals across 13 markets, found that 66% of respondents said they would seek professional help for sleep issues, but only 23% had actually done so. The gap between intention and action is large. If you have been struggling for more than three months and have not seen improvement after consistent application of Tier One and Tier Two methods, the appropriate next step is to follow through on that intention and schedule a clinical evaluation.
Summary: The Evidence Gradient in Practice
The difference between this framework and a generic list of 15 sleep tips is the gradient. Tier One interventions — consistent schedule, light management, thermal environment, caffeine timing — have the broadest evidence base and the lowest barrier to entry. They should be in place for everyone. Tier Two methods — stimulus control and sleep restriction — require more consistency and may feel uncomfortable at first, but they target the specific behavioral mechanisms that maintain poor sleep and have strong RCT support. Tier Three — CBT-I and clinical evaluation — are for persistent problems that have not responded to the first two tiers.
The most common mistake readers make is skipping tiers. Jumping from a flat list of tips directly to a supplement or a device without first establishing the fundamentals is like trying to fix a leaky roof by rearranging the furniture. Start at the bottom of the pyramid. Give each tier a fair trial — two to four weeks for Tier One, four to six weeks for Tier Two. Only then, if improvement is still insufficient, escalate to Tier Three. The evidence supports this sequence, and your sleep will too.
Comments
Join the discussion with an anonymous comment.