Mechanism explainer
Sleep Debt and Recovery Science: Can You Actually Catch Up on Lost Sleep?
A mechanistically grounded, research-anchored examination of how sleep debt accumulates, why recovery is domain-specific and asymmetric, and what the evidence actually says about weekend catch-up sleep, recovery timelines, and sleep banking — for adults who want more than a simple yes-or-no answer.
Why 'I'll Catch Up on the Weekend' Is More Complicated Than It Sounds
Most adults who regularly cut their sleep short hold a quiet assumption: the deficit is temporary, and a long Saturday morning will balance the ledger. It is an intuitive model — sleep less during the week, sleep more on the weekend, net result zero. The problem is that the brain does not account for sleep the way a bank accounts for money.
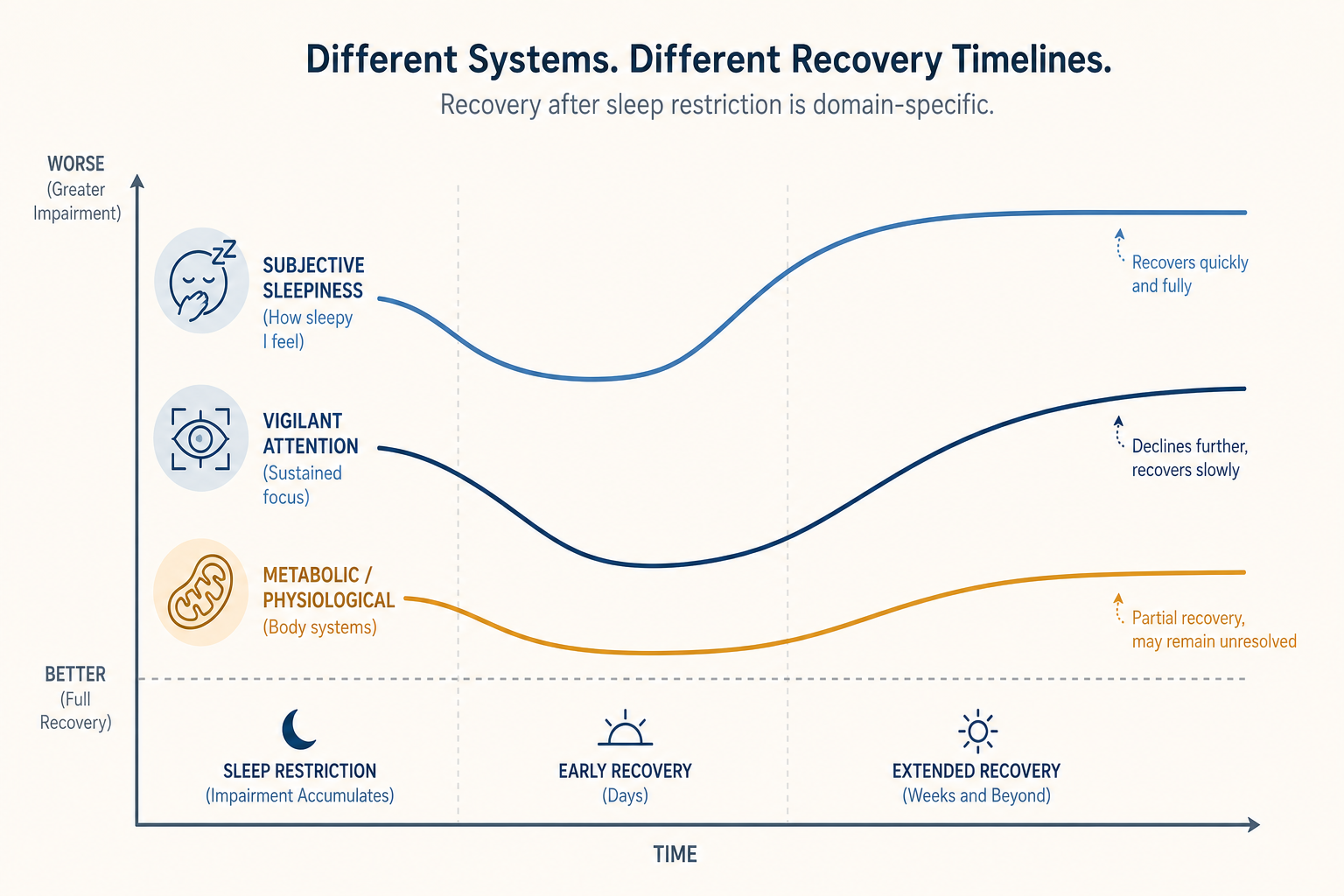
What the research shows is considerably more complicated. Recovery from sleep restriction is not a single event — it is a domain-specific process that unfolds at different rates across different systems. Subjective sleepiness often normalizes within a few days of adequate sleep. Sustained attention, mood stability, and metabolic regulation take much longer. Some measures, in controlled studies, have not returned to baseline even after a full week of unrestricted recovery sleep.
This article works through the evidence systematically: how sleep debt accumulates at a neurochemical level, why mild chronic shortfalls are more dangerous than they appear, what the perception gap means for self-assessment, how long different domains actually take to recover, and what the divided evidence on weekend catch-up and sleep banking actually says.
How the Brain Accounts for Sleep: Adenosine, Process S, and the Two-Process Model
The brain tracks the need for sleep through a mechanism that is, at its core, biochemical. During every waking hour, neurons throughout the brain — particularly in the basal forebrain — release adenosine as a byproduct of metabolic activity. Adenosine accumulates in the extracellular space, binding to receptors that progressively suppress arousal and increase sleep pressure. The longer you are awake, the more adenosine has built up, and the stronger the drive to sleep becomes.
This adenosine-mediated mechanism is the molecular substrate of what sleep researchers call Process S — the homeostatic component of the two-process model of sleep regulation. Process S rises during wakefulness and dissipates during sleep. When sleep is cut short, adenosine clearance is incomplete, and Process S carries a residual elevation into the next waking period. That residual is what constitutes sleep debt at the neurochemical level.
The two-process model pairs Process S with Process C — the circadian drive governed by the suprachiasmatic nucleus and the molecular clock machinery. Process C creates the daily rhythm of alertness and sleep propensity independent of how long you have been awake. The interaction between the two processes determines when you feel sleepy, how deeply you sleep, and how efficiently you recover. For the purposes of understanding sleep debt, Process S is the primary mechanism — it is the accumulating pressure that builds with restriction and that must be discharged through sufficient sleep.
The circadian architecture that governs Process C — the SCN, the CLOCK/BMAL1 feedback loop, and melatonin timing — is covered in detail in the article on circadian rhythm mechanisms. This article focuses on Process S and what happens when adenosine clearance is chronically incomplete.

Acute vs. Chronic Restriction: Why Mild Nightly Shortfalls Are More Insidious
Most discussions of sleep deprivation focus on the dramatic end — a full night without sleep, or military-style total deprivation studies. These are useful for establishing physiological limits, but they do not describe how most adults actually accumulate sleep debt. The more common pattern is chronic partial restriction: getting six hours instead of eight, night after night, week after week.
Research by David Dinges and Hans Van Dongen at the University of Pennsylvania quantified what this looks like in practice. Participants restricted to six hours of sleep per night for 14 consecutive days accumulated cognitive deficits equivalent to those produced by two full nights of total sleep deprivation. The impairment was not trivial and did not plateau at a manageable level — it continued to compound across the two-week period.
The insidious quality of chronic partial restriction is precisely its moderation. A single night of six hours feels manageable. Two nights feels slightly worse. By the end of the second week, the cumulative deficit has reached a level that would be immediately recognizable if it had arrived all at once — but because it arrived incrementally, it does not feel that way.
| Sleep Pattern | Duration | Approximate Cognitive Equivalent |
|---|---|---|
| 8 hours/night | 14 days | Baseline — no significant deficit |
| 6 hours/night | 14 days | Similar to ~48 hours total sleep deprivation |
| 4 hours/night | 5 nights | Severe impairment across vigilance, mood, and sleepiness |
| Total deprivation | 1–2 nights | Acute severe impairment; faster onset than chronic restriction |
The Perception Gap: Feeling Fine While Performing Poorly
The most clinically significant finding in the sleep debt literature may not be how much impairment accumulates — it is the gap between how impaired people are and how impaired they feel. After two to three days of sleep restriction, subjective sleepiness largely stabilizes. People stop feeling progressively worse. They adapt to their new baseline and report feeling only mildly tired, or not particularly tired at all.
Objective performance, measured on tasks like the Psychomotor Vigilance Test (PVT), tells a different story. Reaction times continue to slow, lapse frequency continues to increase, and error rates continue to climb — even as subjective reports of sleepiness plateau. The person has become acclimatized to their impaired state and is no longer able to accurately assess it.
A 2025 narrative review published in Cureus covering cognitive and behavioral consequences of sleep loss confirmed this pattern across multiple study designs. The review notes that individuals may continue to perceive their performance as unimpaired despite objective deficits — a finding that, as the authors observe, poses serious risks in environments that demand accurate self-monitoring.
This is also why anecdotal evidence about catching up on sleep tends to be misleading. People feel better after a weekend of extra sleep — and they genuinely are less sleepy. But 'less sleepy' is not the same as 'fully recovered,' and the subjective improvement does not accurately track the degree of objective restoration.
What Sleep Debt Actually Impairs: A Domain-by-Domain Breakdown
Sleep debt does not produce a uniform, generalized degradation of function. Different cognitive and physiological systems are affected through distinct mechanisms, and they do not all recover at the same rate. Understanding which systems are impaired — and why — provides a more accurate picture of what is actually at stake than a generic claim about 'cognitive impairment.'
Attention and Vigilance
Sustained vigilant attention is among the most consistently and severely impaired functions under sleep restriction. The Psychomotor Vigilance Test, which measures reaction time to unpredictable stimuli over a sustained period, reliably shows increasing lapses and slowing responses as restriction accumulates. The underlying mechanism involves disruption of the prefrontal-thalamic circuitry that supports sustained arousal and attentional control. Even mild restriction produces measurable PVT deficits within days.
Memory Consolidation
Both the encoding of new memories and their consolidation during sleep are disrupted by restriction. Slow-wave sleep (NREM Stage 3) plays a particularly important role in declarative memory consolidation — the replay and stabilization of hippocampal memory traces during slow oscillations and sleep spindles. Chronic partial restriction reduces the amount and intensity of slow-wave sleep, impairing both the formation and the long-term retention of learned material. Procedural memory, which relies more on REM sleep, is also affected.
The sleep architecture article on NREM and REM stages covers the stage-level mechanisms in detail. For the purposes of sleep debt, the key point is that slow-wave sleep intensity — not just total sleep duration — matters for memory consolidation, and this has direct implications for what makes recovery sleep restorative.
Executive Function and Decision-Making
The dorsolateral prefrontal cortex (DLPFC), which supports working memory, cognitive flexibility, and adaptive decision-making, shows markedly reduced activation after sleep loss. The practical consequences include impaired updating of working memory, reduced ability to inhibit automatic responses in favor of deliberate ones, and a blunting of feedback sensitivity — the ability to adjust behavior based on outcomes. People under sleep restriction tend to persist with suboptimal strategies longer and are less responsive to negative feedback.
Emotional Regulation
Sleep loss disrupts the prefrontal-amygdala connectivity that normally allows the prefrontal cortex to modulate emotional reactivity. The result is a pattern of heightened amygdala activation in response to emotional stimuli, combined with reduced top-down inhibition. People become more reactive, more negatively biased in their interpretation of ambiguous social cues, and less able to return to emotional baseline after a stressor. This is not a subjective impression — it is a measurable change in neural connectivity documented in neuroimaging studies.
Metabolism and Immune Function
Metabolic dysregulation under chronic sleep restriction includes alterations in insulin sensitivity, appetite-regulating hormones (leptin and ghrelin), and glucose metabolism. Immune function is also affected — markers of inflammatory stress remain elevated across cyclic restriction-and-recovery patterns, suggesting that even periods of recovery sleep do not fully reset the immune system when restriction is ongoing.
| Domain | Primary Mechanism | Recovery Speed (Relative) |
|---|---|---|
| Subjective sleepiness | Adenosine clearance, Process S dissipation | Relatively fast (days) |
| Reaction time / vigilance | Prefrontal-thalamic disruption, PVT lapses | Slow (days to over a week) |
| Memory consolidation | Reduced SWS intensity, hippocampal replay disruption | Slow; depends on slow-wave recovery |
| Executive function | DLPFC hypoactivation, feedback blunting | Slow; partially persists after recovery |
| Emotional regulation | Prefrontal-amygdala disconnect | Moderate; improves with recovery sleep |
| Metabolic markers | Hormonal dysregulation, insulin sensitivity | Slow; may not fully reverse with short-term recovery |
| Immune stress markers | Inflammatory signaling | Slow; elevated across cyclic restriction/recovery |
Recovery Timelines: How Long Does It Actually Take?
The controlled evidence on recovery timelines is more sobering than most popular accounts suggest, and it varies substantially by domain.
A study from Jagiellonian University, published in PLOS ONE in 2021, followed participants through 10 days of partial sleep deprivation — approximately one-third less sleep than their usual amount — followed by seven full days of unrestricted recovery sleep. Among all the measures tested, which included behavioral, locomotor, and neurophysiological outcomes, only reaction speed returned to baseline after the seven-day recovery period. All other measures remained impaired. The authors concluded that the neurobehavioral consequences of chronic partial sleep deprivation cannot be easily overcome and last much longer than most people expect.
A separate line of research by Banks and colleagues, reviewed in a 2022 analysis published in Sleep Advances, examined what happens after more severe acute restriction. After five nights of restriction to four hours per night, even a 10-hour recovery sleep opportunity failed to fully restore vigilant attention, subjective sleepiness, and mood to pre-restriction baseline. The recovery was real — participants improved substantially — but it was not complete.
A particularly important finding from that same body of work concerns the amplification effect: when recovery from sleep debt is incomplete and a second period of restriction follows, the impairment accumulates faster and reaches greater severity than during the first restriction episode. Preliminary data from Banks and colleagues suggested that vigilant attention impairment during a second restriction period was nearly twice what it was during the first. Incomplete recovery does not just leave you at a deficit — it leaves you more vulnerable.
Individual variability is also substantial. The timelines above come from controlled laboratory studies with relatively small, homogeneous samples. Age, baseline sleep need, health status, and genetic variation in sleep homeostasis all influence how quickly a given individual recovers. The controlled study timelines represent useful reference anchors, not universal predictions.
Weekend Catch-Up Sleep: What the Evidence Actually Shows
The weekend catch-up question has produced genuinely contradictory findings in large-scale epidemiological research, and it is worth examining both sides carefully rather than defaulting to a simple verdict.
The Cardiovascular Evidence — and Why It Conflicts
At ESC Congress 2024, researchers presented findings from a UK Biobank prospective cohort study of 90,903 participants followed for a median of approximately 14 years. Those in the highest quartile of compensatory weekend sleep — measured via accelerometer — had a 19% lower risk of developing heart disease compared to those with the least catch-up sleep. Among the subgroup who reported chronic weekday sleep deprivation, the risk reduction reached 20%. The association was robust and the sample was large.
A separate accelerometer-based UK cohort study, published in the journal Sleep in 2024 (PMID 38895883), examined 73,513 participants over approximately eight years and reached the opposite conclusion. After full multivariable adjustment, weekend catch-up sleep was not associated with mortality or incident cardiovascular disease. The null finding held in dose-response analyses and in analyses restricted to adults sleeping fewer than six hours on weekdays. The authors noted directly that their results do not align with prior evidence suggesting that weekend catch-up sleep offers protective cardiovascular benefits.
These two studies are methodologically similar in many respects — both large, both prospective, both using accelerometer-measured sleep in UK populations — yet they reach opposite conclusions. The most likely explanation involves differences in how catch-up sleep was defined, how confounders were adjusted for, and which specific cardiovascular outcomes were measured. This is a live area of scientific disagreement, not a settled question. Presenting only the ESC finding would be misleading; so would presenting only the null result.
What Lab Studies Show: Metabolism and Cognition
Controlled laboratory studies, which cannot match the scale of cohort research but can measure mechanisms directly, tell a consistent story on metabolic outcomes. Research by Depner and colleagues published in Current Biology in 2019 found that weekend catch-up sleep did not prevent the metabolic dysregulation, circadian phase delay, or increased weight gain associated with weekday sleep restriction. Participants who restricted on weekdays and recovered on weekends showed worse metabolic profiles than those who maintained consistent adequate sleep throughout.
The same body of research, reviewed in a 2022 Sleep Advances analysis, found that immune stress markers remained elevated across cyclic restriction-and-recovery patterns — suggesting that the inflammatory consequences of ongoing restriction are not reversed by periodic recovery sleep within the same week.
| Outcome Domain | Weekend Catch-Up Evidence | Study Type |
|---|---|---|
| Heart disease risk | Up to 20% lower risk in highest catch-up quartile (ESC 2024) | Large prospective cohort (90,903 participants) |
| Mortality and CVD incidence | No significant association after full adjustment | Large prospective cohort (73,513 participants, Sleep 2024) |
| Metabolic dysregulation | Not prevented by weekend recovery | Controlled lab study (Depner et al., 2019) |
| Circadian phase delay | Not prevented; persists into following week | Controlled lab study |
| Immune/inflammatory markers | Remain elevated across cyclic restriction/recovery | Controlled lab study |
| Cognitive performance | Does not fully restore vigilant attention or mood | Controlled lab study (Banks et al.) |
Sleep Banking: Building Resilience Before Anticipated Sleep Loss
Sleep banking is a distinct concept from weekend catch-up. Rather than trying to recover from debt after the fact, banking involves extending sleep before a period of anticipated restriction — building up a reserve that may reduce the severity of subsequent impairment and accelerate recovery.
The foundational study in this area was conducted by Rupp and colleagues in 2009 at Walter Reed Army Institute of Research. Military personnel were divided into two groups: one slept their habitual seven hours per night in the pre-restriction period, while the other extended to ten hours per night. Both groups then underwent a period of severe restriction to three hours per night. The ten-hour group showed less decline in alertness during the restriction period and returned to baseline more quickly afterward. The banking effect was real and measurable.
This finding has been replicated in other contexts. A 2023 study in a Miami hospital setting found that approximately 90 minutes of additional sleep over three nights improved performance on night shifts. Sport performance research has found similar patterns — rugby players, tennis players, and basketball players who extended sleep for several weeks before competition showed improvements in physical output, serving accuracy, and sprint speed. A BBC Future analysis from February 2026 reviewed this evidence alongside the mechanistic debate about what banking actually does.
Rupp's proposed mechanism is that extended sleep gives the brain additional time to clear neuronal metabolic waste and replenish glycogen stores in astrocytes — processes that may not complete fully within a standard seven-to-eight hour window. By running these processes to completion over multiple nights of extended sleep, the brain may enter a restriction period with a fuller functional reserve.
The Counter-Argument: Can You Actually Store Sleep?
Elizabeth Klerman, a sleep researcher at Harvard Medical School and Massachusetts General Hospital, challenges the banking concept at a fundamental level. Her position is that sleep is more like a credit mechanism than a savings account: you can accumulate debt, but you cannot store a surplus.
In order to show that sleep banking occurs, you need to show that somebody can sleep when they're not tired, and there is no evidence for that.
Klerman's argument rests on a basic physiological constraint: sleep is driven by Process S homeostatic pressure. When adenosine levels are low — when the brain has already cleared its sleep pressure — there is no mechanism to continue accumulating additional 'credit.' Experiments in which participants are given more time in bed than their habitual sleep duration often show that they simply fail to sleep longer. They lie awake. The extra time in bed does not translate into extra sleep.
The banking studies, by this interpretation, may be demonstrating something more modest: that participants in the extended-sleep condition were chronically mildly sleep-deprived at baseline and simply corrected that deficit during the banking period. The 'banking' effect may reflect debt repayment rather than true surplus storage.
A 2025 paper published in Science identified RE-ZI neuron circuits as a discrete neural substrate governing homeostatic sleep debt tracking and repayment. This finding, if confirmed, would provide a circuit-level mechanism for how the brain registers and discharges sleep debt. However, the primary source could not be directly verified for this article, and this claim should be treated as emerging rather than established.
A Practical, Evidence-Grounded Recovery Protocol
The research does not support a simple prescription, but it does point toward several principles that are better grounded than the conventional wisdom of 'sleep in on the weekend.'
- Prioritize consistent recovery over total rebound hours. A week of seven-to-eight hours per night will restore more function than two nights of ten hours followed by a return to restriction. The brain responds better to sustained adequate sleep than to large intermittent doses.
- Recognize that slow-wave sleep intensity matters alongside duration. Recovery sleep produces a rebound in slow-wave activity — the homeostatic response to prior restriction. This rebound is part of what makes recovery sleep more restorative than equivalent-duration habitual sleep. Conditions that fragment sleep (alcohol, stimulants, noise) disrupt this rebound even when total time in bed is preserved.
- Use prophylactic napping before anticipated deprivation. Pre-deprivation napping has documented benefit for reducing subsequent impairment. A 20-to-30 minute nap in the afternoon before a night of expected sleep loss reduces the severity of cognitive decline during that night.
- Restore sleep schedules incrementally rather than abruptly. Large abrupt shifts in sleep timing — sleeping in three hours later on a weekend — advance the circadian phase in ways that make it harder to fall asleep on Sunday night, setting up the following week's restriction before it begins. Gradual schedule restoration minimizes this effect.
- Split sleep has equivalent performance value when total time is equal. Research on split sleep schedules — for example, a core nighttime sleep plus a brief afternoon nap — shows that performance is broadly equivalent to consolidated sleep of the same total duration, provided the split is consistent. This has practical relevance for shift workers and those with fragmented schedules.
- If banking before anticipated deprivation, extend sleep gradually over at least one week. The Rupp protocol involved 10-hour opportunities over multiple nights. Single nights of extended sleep are unlikely to produce the same effect, and some individuals may not be able to sleep longer even with the opportunity.
When Persistent Sleep Difficulty Signals Something More Than Behavioral Debt
Most of what this article describes applies to people who are not getting enough sleep because of behavioral and lifestyle factors — work demands, late schedules, inconsistent timing. For these individuals, the path forward is behavioral: protect sleep opportunity, stabilize timing, and allow adequate time for recovery.
But there is a distinct pattern that warrants clinical attention: adequate sleep opportunity that consistently fails to produce restorative sleep. If you are spending eight or more hours in bed and still waking unrefreshed, still accumulating what feels like debt despite sufficient time asleep, the explanation may not be behavioral sleep restriction. It may be an underlying disorder.
Obstructive sleep apnea (OSA) is one of the most common and underdiagnosed causes of this pattern. Repeated breathing disruptions throughout the night fragment sleep architecture and suppress slow-wave sleep, producing objective sleep debt even when total time in bed is adequate. The person wakes feeling unrefreshed and accumulates cognitive deficits consistent with restriction — because, from the brain's perspective, restriction is what has occurred. The OSA condition page covers the diagnostic criteria and treatment options in detail.
Chronic insomnia — defined by difficulty initiating or maintaining sleep despite adequate opportunity, persisting for at least three months — is another condition where behavioral debt framing does not apply. The first-line evidence-based treatment for chronic insomnia is not sleep extension or catch-up strategies; it is Cognitive Behavioral Therapy for Insomnia (CBT-I), a structured multicomponent intervention with strong RCT support.
Supports these guides
Spot an error or have clinical feedback?
Because this article covers clinical, medication, or safety information, we use a moderated correction channel instead of open public comments. Let us know if something about “Sleep Debt and Recovery Science: Can You Actually Catch Up on Lost Sleep?” needs a closer look.
Send feedback on this article