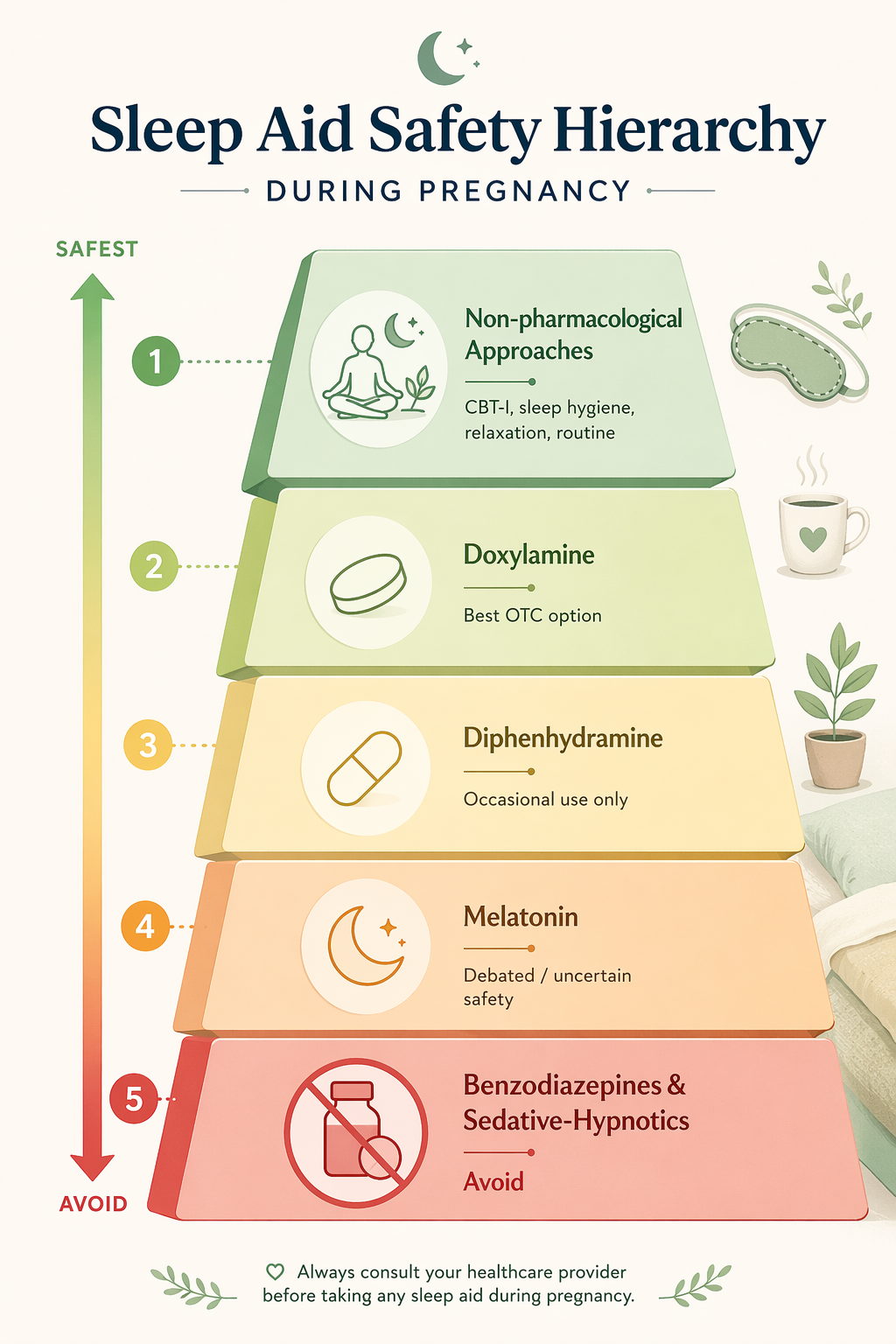
If you are awake in pregnancy and searching for sleep aids that are safe for pregnancy, the safest answer is not a single product. It is a hierarchy. Start with non-drug insomnia care, especially CBT-I. If medication is needed, doxylamine has the most useful pregnancy-specific OTC safety story, largely because of its role in the FDA-approved nausea medication Diclegis. Diphenhydramine is usually discussed as an occasional option, but its sleep-specific pregnancy evidence is thinner. Melatonin is unresolved, not automatically safe because it is “natural.” Benzodiazepines, barbiturates, alcohol, cannabis, poorly studied herbal sedatives, and late-pregnancy sedative-hypnotic shortcuts belong in the avoid-or-specialist-only zone. Disturbed sleep is common in pregnancy: one patient-facing sleep medicine source reports that about 78% of pregnant people experience disturbed sleep, and insomnia may affect up to 80% by the third trimester.[1]
| Option | Pregnancy safety position | Why it lands there |
|---|---|---|
| CBT-I and other non-drug approaches | First-line | No fetal drug exposure; randomized trials and a 2022 meta-analysis show meaningful sleep improvement.[2][3] |
| Doxylamine | Best-supported OTC candidate when a prenatal clinician agrees | The strongest data come from doxylamine plus vitamin B6 in Diclegis, not from every possible OTC dosing pattern.[4][5] |
| Diphenhydramine | Occasional-use discussion, not a default nightly plan | Often considered acceptable short term, but much pregnancy safety evidence comes from allergy or nausea contexts rather than insomnia treatment.[1] |
| Melatonin | Uncertain; avoid routine self-use | Human pregnancy data are sparse, dose-response is unclear, and major patient-facing sources advise against routine use.[6][7] |
| Benzodiazepines, barbiturates, alcohol, cannabis, many herbal sedatives, late-pregnancy zolpidem without clear clinician direction | Avoid unless a clinician is managing a specific risk-benefit situation | These options raise fetal, neonatal, dependence, respiratory, or evidence-gap concerns that do not fit casual sleep-aid use.[1] |
Why pregnancy changes the sleep-aid standard
Outside pregnancy, a sleep aid is often judged by whether it helps someone fall asleep and whether the next morning feels tolerable. During pregnancy, that is not enough. A useful option has to clear a second question: what is known about fetal exposure, neonatal effects, and use in an actual pregnant population?
This is also why old FDA letter categories can mislead. You may still see older sources call a drug “Category B” or “Category C,” but the FDA replaced that letter system with the Pregnancy and Lactation Labeling Rule, which began phasing in narrative risk summaries in 2015.[8] The letters were simple, but simplicity came at a cost: readers could mistake a category for a clean safety grade. Pregnancy decisions usually need more texture than that.
A second issue is context. A medication may have pregnancy data because it was used for nausea or allergies, while the person reading at night wants it for sleep. That evidence can still matter, but it should not be stretched further than it goes. Dose, timing, frequency, trimester, other medications, and underlying conditions can all change the conversation.
First-line: CBT-I is not “just sleep hygiene”
The most protective first move is evidence-based behavioral treatment for insomnia, especially cognitive behavioral therapy for insomnia, or CBT-I. That can sound underwhelming when someone is exhausted. It should not. CBT-I is a structured treatment that changes the sleep-wake patterns, conditioned arousal, and unhelpful sleep behaviors that keep insomnia going. It is different from being told to buy a better pillow or stop looking at a phone.
A 2022 systematic review and meta-analysis of non-pharmacological sleep interventions in pregnancy included six randomized controlled trials with 623 women and found an average Pittsburgh Sleep Quality Index improvement of 3.03 points compared with control conditions.[2] That result does not mean every pregnant person will sleep well after a few nights of effort. It does mean non-drug care has trial-level evidence and no teratogenic medication exposure, which is a rare combination in pregnancy insomnia.
The CBT-I data are especially worth taking seriously. In one randomized trial summarized by the MGH Center for Women’s Mental Health, CBT-I led to insomnia remission in 64% of pregnant participants, compared with 52% in the control group, and the median time to remission was 31 days versus 48 days.[3] A digital CBT-I trial reported remission in 44% of participants using the intervention compared with 22% receiving standard care, with benefits maintained at a two-month follow-up.[3]
That timeline matters. CBT-I is not an instant sedative, and a person who has not slept well for weeks may still need medical help tonight. But it gives prenatal clinicians something better than vague reassurance: a first-line treatment that can be started without adding fetal drug exposure. For a deeper explanation of how the method works, see What Actually Cures Insomnia? CBT-I Explained.
What belongs in the non-drug tier
The non-drug tier is broader than CBT-I, but not all parts are equally powerful. Sleep hygiene, relaxation exercises, music therapy, and acupressure appeared in the pregnancy non-pharmacological evidence base reviewed in the 2022 meta-analysis.[2] They are reasonable adjuncts, especially when they reduce arousal, discomfort, or bedtime inconsistency.
- Use CBT-I as the anchor when insomnia is persistent, not merely one uncomfortable night.
- Treat sleep hygiene as support: consistent wake time, light exposure, caffeine timing, and a bedroom routine can help but may not be enough alone.
- Adjust pregnancy-specific friction points: reflux timing, nighttime urination, leg cramps, nasal congestion, fetal movement, and side-sleep discomfort.
- Escalate sooner if insomnia is paired with anxiety, depression symptoms, severe nausea, hypertension concerns, breathing pauses, or restless legs symptoms.
For practical bedtime routine changes, a general guide like Sleep Hygiene Fundamentals and an Evidence-Based Bedtime Routine can be useful, but persistent pregnancy insomnia deserves more than routine polishing. If the problem is happening most nights, ask specifically about CBT-I access, digital CBT-I, or a clinician-recommended insomnia program.
Doxylamine: the strongest OTC safety story, with one important boundary
Doxylamine is the OTC sleep aid that most clearly belongs in the pregnancy conversation, but the reason should be stated carefully. Its strongest pregnancy safety data are tied to doxylamine succinate combined with pyridoxine hydrochloride, or vitamin B6, the combination sold as Diclegis for nausea and vomiting of pregnancy. MotherToBaby states that studies have not found an increased chance of birth defects, miscarriage, preterm delivery, or low birth weight with this combination.[4]
That is a much stronger foundation than a generic “people take it and seem fine” claim. Drugs.com notes that the doxylamine-pyridoxine combination has been used in many pregnant people and that data have not shown an increased risk of fetal harm.[5] ACOG also describes vitamin B6 and doxylamine as safe, stating that they have “no harmful effects on the fetus” when used for nausea and vomiting of pregnancy.[9]
The boundary is that Diclegis is not the same thing as taking any OTC doxylamine product in any amount, on any schedule, or alongside other sedating medicines. OTC Unisom SleepTabs contain doxylamine succinate and are sometimes discussed in prenatal care, but the clearest safety evidence comes from a specific medication context: doxylamine plus B6 for pregnancy nausea. That evidence is highly relevant. It is not a blank check for self-dosing.
This is why doxylamine is best handled as a clinician-agreed option, particularly if nausea is also part of the sleep problem. A prenatal clinician can check whether the product is actually doxylamine rather than a different Unisom formulation, whether other sedating medicines are already in the picture, and whether next-day drowsiness could create a safety issue with driving, work, caregiving, or falls.
Diphenhydramine: familiar, but less specific
Diphenhydramine, the antihistamine in Benadryl and many PM-labeled products, is commonly treated as an occasional pregnancy option. Sleep Foundation notes that it has historically been listed as FDA Pregnancy Category B, though that category system has been replaced, and reports that about 10% to 15% of pregnant women use diphenhydramine.[1][8]
The caution is not that one occasional dose is known to be dangerous. The caution is that much of the comfort around diphenhydramine comes from broader antihistamine use, not from robust pregnancy insomnia trials. It can also cause next-day grogginess, dry mouth, constipation, urinary retention, and confusion in some people. In pregnancy, those side effects can land on top of reflux, constipation, nighttime bathroom trips, and already-fragile daytime functioning.
Combination products deserve extra care. “PM” pain relievers may include acetaminophen plus diphenhydramine, which is not the same decision as taking an antihistamine alone. If pain is the reason sleep is impossible, the better question may be how to treat the pain safely in pregnancy, not how to sedate through it.
Melatonin is not proven safe just because the body makes it
Melatonin is the sleep aid that most often sounds harmless before the evidence is examined. The body does make melatonin, and pregnancy changes melatonin physiology. Sleep Foundation notes that the placenta produces melatonin locally and that production is highest in the first trimester.[6] That does not answer the supplement question.
A supplement is an added exposure. Dose, timing, product quality, and duration matter, and pregnancy-specific dose-response evidence is limited. Sleep Foundation describes melatonin as debated in pregnancy, notes sparse human data, and reports that only about 4% of pregnant women in one 2020 study used it.[6] MotherToBaby also says it is not known whether taking melatonin can increase the chance of birth defects, miscarriage, preterm delivery, or low birth weight because human data are limited.[7]
Animal and high-dose research does not translate neatly to a typical OTC bottle, but it does show why confidence would be premature. Sleep Foundation describes animal findings involving lower birth weights in rats and a study using 75 to 300 milligrams, far above common OTC doses, that affected ovarian function.[6] Those details do not prove that low-dose melatonin harms human pregnancies. They do mean the casual phrase “natural sleep aid” is doing more work than the evidence supports.
For now, melatonin sits below doxylamine and diphenhydramine in the hierarchy because the pregnancy-specific safety case is less settled. If a clinician recommends it for a narrow reason, that is different from routine self-use because it is sold next to vitamins.
Prescription sedatives and “natural” sedatives need a higher bar
Benzodiazepines, barbiturates, and sedative-hypnotics are not in the same safety bucket as antihistamines. They may be used in specific medical circumstances, but they are not casual pregnancy sleep aids. Sleep Foundation places benzodiazepines, barbiturates, alcohol, cannabis, and several herbal products in the avoid category for pregnancy sleep support, and it flags zolpidem with particular concern in later pregnancy because of neonatal respiratory depression risk.[1]
Zolpidem deserves that nuance. The issue is not that every person who has ever taken a dose before knowing she was pregnant has caused harm. The issue is that late-pregnancy sedative exposure can affect the newborn, and the decision belongs with a clinician who can weigh severe insomnia, mental health risk, other medications, trimester, dose, and delivery timing.
Herbal products also need more skepticism than marketing usually gives them. Valerian, kava, and chamomile are often presented as gentle alternatives, but “plant-derived” does not mean pregnancy-tested. Sleep Foundation notes concern about herbal sleep aids and mentions a late-pregnancy chamomile finding from one study.[1] A single study should not be inflated into a universal rule, but it is enough to keep chamomile out of the “obviously safe” category.
What to do tonight, and what to bring to prenatal care
If this is one bad night, the lowest-risk moves are boring but still useful: reduce the battle with the bed, get out of bed briefly if wakefulness has become tense, keep light low, avoid scrolling, manage reflux or nausea within your prenatal plan, and return when sleepy. If this has become a pattern, the next step is not to keep layering products. Ask for help with insomnia as a pregnancy symptom worth treating.
- Ask specifically whether CBT-I, digital CBT-I, or referral-based insomnia care is available.
- If nausea is part of the problem, ask whether doxylamine plus vitamin B6 is appropriate for you.
- Bring the exact bottle or ingredient list for any OTC sleep aid, especially Unisom or PM-labeled products.
- Do not combine doxylamine, diphenhydramine, melatonin, prescription sedatives, alcohol, cannabis, or herbal sedatives without guidance.
- Mention snoring, breathing pauses, restless legs, depression symptoms, anxiety, severe nausea, itching, high blood pressure concerns, or reduced functioning during the day.
The practical boundary is simple enough to use at 2 a.m.: start with evidence-based non-drug care; treat doxylamine as the best-supported OTC candidate to discuss with a prenatal clinician; use diphenhydramine only as an occasional, less sleep-specific option if approved; do not treat melatonin or herbs as exempt from evidence; and keep stronger sedatives out of self-treatment.
References
- Sleep Aids to Take While Pregnant, Sleep Foundation
- Non-pharmacological Interventions for Improving Sleep Quality During Pregnancy: A Systematic Review and Meta-Analysis, PMC
- Essential Reads: Cognitive Behavioral Therapy for Insomnia During Pregnancy, MGH Center for Women's Mental Health
- Doxylamine succinate-pyridoxine hydrochloride (Diclegis®), MotherToBaby
- Doxylamine Use During Pregnancy, Drugs.com
- Can You Take Melatonin While Pregnant?, Sleep Foundation
- Melatonin, MotherToBaby
- Pregnancy and Lactation Labeling (Drugs) Final Rule, U.S. Food and Drug Administration
- Morning Sickness: Nausea and Vomiting of Pregnancy, American College of Obstetricians and Gynecologists


Comments
Join the discussion with an anonymous comment.