
Introduction: Why the Anxiety-Sleep Cycle Needs a Dual-Action Approach
Anxiety and insomnia are not just frequent bedfellows; they share a common neurobiological engine. The Cleveland Clinic notes that anxiety is the most common mental health disorder in the U.S., affecting roughly 40 million people, and that the majority of those individuals also experience some form of sleep disruption. This isn't a coincidence—it's a feedback loop. Racing thoughts and elevated stress hormones make it physiologically difficult to transition into sleep, while poor sleep further erodes the brain's ability to regulate mood the next day.
Most over-the-counter sleep aids on the market today are designed for a single job: making you unconscious. They achieve this through sedation, not by addressing the underlying anxiety that is keeping your nervous system alert. For an adult with mild-to-moderate anxiety, this is a critical distinction. A sedative can knock you out, but it won't quiet the neural pathways that triggered the hyperarousal in the first place. The result is often fragmented sleep, a groggy morning, and a return of the same anxiety the following night.
This guide takes a different approach. Instead of presenting a ranked list of products, it organizes OTC options by their mechanism of action, focusing specifically on ingredients that target the shared neurochemistry of anxiety and insomnia. The goal is to help you make a choice that is not only effective but also safe for your specific situation.
How the GABA System Connects Anxiety and Sleep
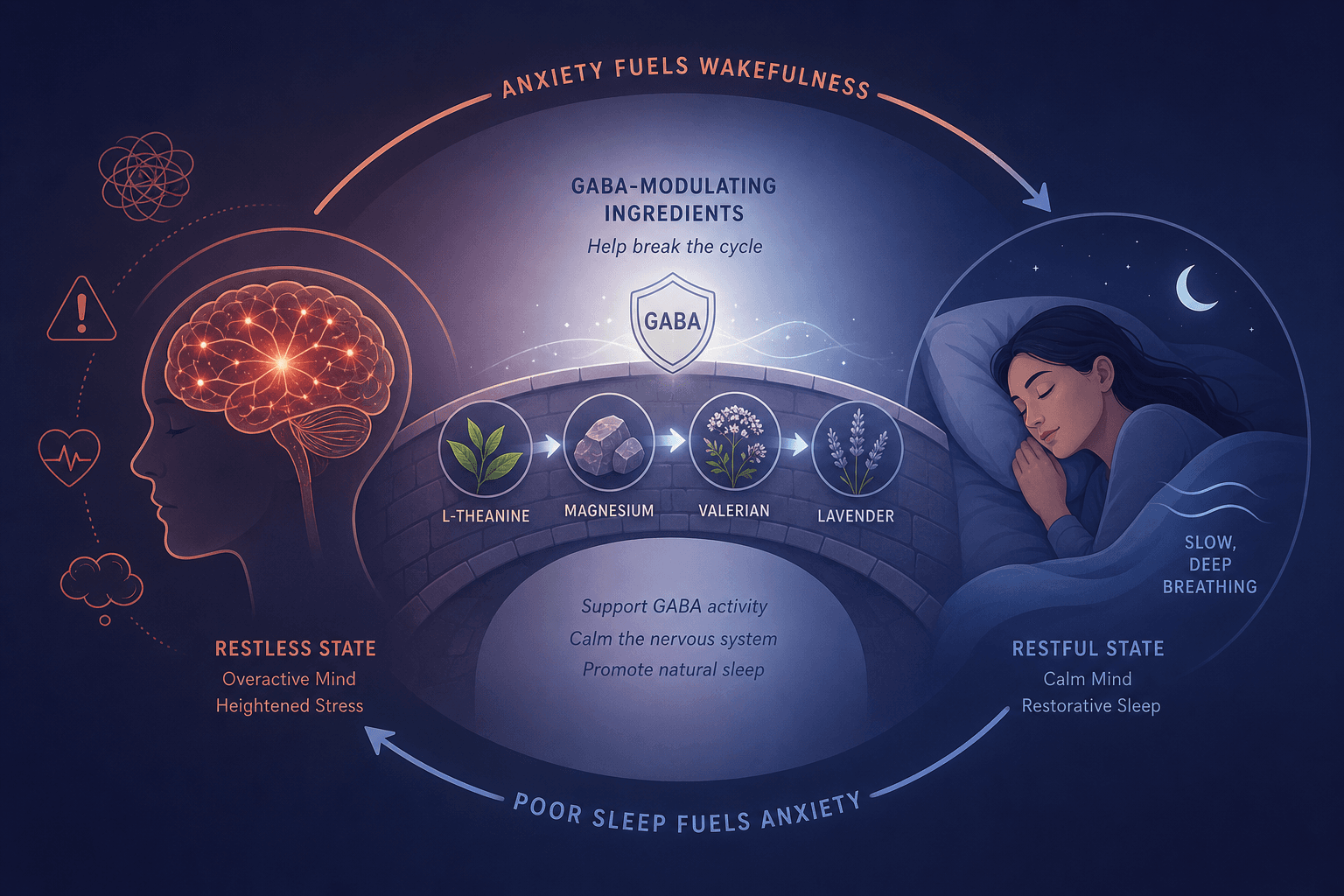
To understand why some OTC ingredients are better suited for anxiety-related insomnia, you need to meet GABA (gamma-aminobutyric acid). GABA is the brain's primary inhibitory neurotransmitter—its job is to calm neural activity. Think of it as the brain's brake pedal. When GABA levels are adequate, your neurons fire at a regulated pace, allowing you to relax and eventually fall asleep. When GABA activity is low or dysregulated, the brain remains in a state of relative excitation, which manifests as anxiety, restlessness, and difficulty initiating sleep.
Both generalized anxiety disorder and chronic insomnia have been linked to GABAergic dysfunction. This shared pathway is why benzodiazepines and Z-drugs (which enhance GABA activity) are effective for both conditions—but also why they carry significant risks of dependence and tolerance. The OTC ingredients discussed in this guide work on this same GABA system, but through gentler, non-habit-forming mechanisms.
Tier 1: GABAergic Options That Target Both Anxiety and Sleep
These are the first-line OTC options for adults whose insomnia is driven by anxiety. They work primarily through GABAergic pathways, have low grogginess risk, and are generally well-tolerated. They are classified as dietary supplements, not FDA-approved drugs for sleep or anxiety.
L-Theanine (100–200 mg)
L-theanine is an amino acid found almost exclusively in tea leaves. Its mechanism is distinct: it promotes the production of GABA and alpha brain waves, which are associated with a state of "alert calmness." Unlike sedatives, it does not cause drowsiness directly; instead, it quiets the mental chatter that prevents sleep onset. A 2022 study cited by Healthline found that 200 to 400 mg daily for 4 to 8 weeks eased anxiety with few side effects. The Sleep Foundation notes that consuming up to 200 mg per day is safe and that it may enhance sleep quality by reducing night-time awakenings.
For a deeper look at dosing and safety, see our full guide on L-Theanine for Sleep.
Magnesium Glycinate (300–420 mg)
Magnesium is involved in over 300 enzymatic reactions, including those that regulate the nervous system. The glycinate form is specifically bound to the amino acid glycine, which itself has calming properties. A randomized double-blind trial in 46 older adults found that taking 500 mg of magnesium daily for 8 weeks led to significantly increased sleep time, improved sleep efficiency, a reduced Insomnia Severity Index (ISI) score, and lower serum cortisol levels. Cortisol is the body's primary stress hormone; chronically high levels are a hallmark of anxiety-driven insomnia.
For a comprehensive comparison of magnesium forms and their specific benefits, see our guide on Magnesium Glycinate for Sleep.
Valerian Root (300–600 mg)
Valerian root has a long history of use as a sleep aid, and modern research supports its efficacy. A 2024 literature review of 18 RCTs found that valerian significantly reduced sleep latency (SMD: -0.71) and improved sleep quality (SMD: -0.46) compared to placebo. Its mechanism involves increasing GABA availability in the synaptic cleft, similar to how prescription anxiolytics work, but with a much milder effect profile. The Sleep Foundation notes that a standard 600 mg dose does not appear to cause significant morning drowsiness, though higher doses can.
Chamomile and Passionflower
These botanicals are milder than valerian but still exert GABAergic effects. Chamomile contains apigenin, a flavonoid that binds to benzodiazepine receptors. Passionflower has been shown in some studies to increase GABA levels. While the evidence for these is less robust than for valerian or L-theanine, they are safe options for very mild anxiety-related sleep disruption and can be consumed as teas.
Tier 2: Antihistamine Sedatives — Why They Are Not Ideal for Anxiety
Diphenhydramine (found in Benadryl and many generic sleep aids) and doxylamine (found in Unisom) are FDA-regulated OTC drugs. They are the most common active ingredients in non-prescription sleep medications. Their mechanism is straightforward: they block histamine receptors in the brain, which induces drowsiness.
The problem for someone with anxiety is that histamine blockade does nothing to address the underlying neural hyperarousal. You may fall asleep faster, but you are still going to bed with an anxious brain. Furthermore, the Mayo Clinic warns that tolerance to the sedative effects of antihistamines develops quickly—often within a few days—meaning you need higher doses to achieve the same effect, while the side effects remain.
These side effects are significant. They include next-day grogginess (the "hangover effect"), dry mouth, constipation, and urinary retention. The AASM and geriatric guidelines specifically advise against using diphenhydramine as a regular sleep aid. It stays in the system for 6 to 12 hours or more and can impair memory, reaction time, and focus the following day.
For adults over 65, the risks are even more pronounced. The Beers Criteria, a standard for potentially inappropriate medication use in older adults, explicitly recommends avoiding diphenhydramine due to its anticholinergic effects, which are associated with confusion, memory problems, and an increased risk of dementia with chronic use. About 12% of adults 65 and older take OTC sleeping pills, according to the Sleep Foundation, making this a widespread but dangerous practice.
Tier 3: Melatonin for Circadian Timing Issues in Anxiety
Melatonin is a hormone, not a sedative. Its primary role is to signal to your body that it is time to sleep by regulating the circadian rhythm. For this reason, it is most effective for conditions involving circadian misalignment, such as jet lag, shift work, or delayed sleep phase syndrome.
In the context of anxiety, melatonin can be useful if your anxiety manifests as a delayed sleep phase—for example, if you lie in bed with racing thoughts until 2 a.m. and then sleep until noon. A meta-analysis of 19 RCTs found that melatonin (0.5–5 mg) significantly reduced sleep latency and increased total sleep time in primary insomnia. However, the Mayo Clinic notes that the effect is typically mild.
Crucially, melatonin does not reduce anxiety. If your primary issue is a generalized feeling of worry or tension that prevents sleep, melatonin is unlikely to be the right first choice. It also has a narrow therapeutic window: lower doses (0.5–3 mg) are generally more effective and cause fewer side effects than higher doses. Taking 10 mg or more can lead to next-day drowsiness, vivid dreams, and headaches.
Tier 4: Silexan (Lavender Oil 80 mg) — The Best-Researched OTC Anxiolytic with Sleep Benefits
Silexan is a proprietary oral preparation of lavender oil, standardized to 80 mg per capsule. It stands apart from every other OTC option on this list because it was developed and studied specifically as an anxiolytic, with sleep improvement measured as a secondary outcome. The evidence base is unusually strong for a non-prescription product.
A 2023 meta-analysis of five double-blind, randomized, placebo-controlled trials (n=1,213) found that Silexan (80 mg/day for 10 weeks) was significantly superior to placebo in reducing the Hamilton Anxiety Rating Scale (HAMA) total score, with an average 2.9-point advantage and a standardized mean difference (SMD) of 0.35. This effect size is comparable to that of prescription SSRIs and SNRIs. The number needed to treat (NNT) for a 50% or greater reduction in HAMA score was 8 across all trials, and 6 for subthreshold anxiety. On the Clinical Global Impression (CGI) scale, 59.5% of Silexan patients were rated as much or very much improved, compared to 39.8% on placebo (NNT=5).
Critically for the anxious sleeper, Silexan produced no sedation, no abuse potential, and no withdrawal symptoms—even with abrupt discontinuation. It also did not impair driving performance. Its mechanism involves modulation of GABA receptors through both olfactory (inhalation of volatile compounds) and pharmacological (systemic absorption) pathways.
Comparison Table: All Options Ranked by Dual-Target Efficacy, Grogginess Risk, and Safety
| Ingredient | Mechanism | Evidence Quality | Typical Dosage | Grogginess Risk | Population Safety Notes | Regulatory Status |
|---|---|---|---|---|---|---|
| Silexan (Lavender Oil) | Anxiolytic + Sleep (GABA modulation) | RCT-supported (5 RCTs, n=1,213; SMD 0.35 on HAMA) | 80 mg once daily | None (no sedation reported) | Safe in trials; no data for pregnancy/breastfeeding | Dietary supplement (US); OTC drug (EU/AU) |
| L-Theanine | Anxiolytic + Sleep (GABA, alpha waves) | RCT-supported (anxiety reduction) | 100–200 mg at bedtime | Very low | Generally safe; limited pregnancy data | Dietary supplement |
| Magnesium Glycinate | Anxiolytic + Sleep (GABA, cortisol reduction) | RCT-supported (sleep in older adults) | 300–420 mg at bedtime | Very low | Safe for most; caution with kidney impairment | Dietary supplement |
| Valerian Root | Sedative + Sleep (GABA increase) | Meta-analysis supported (SMD -0.71 sleep latency) | 300–600 mg before bed | Low to moderate (at high doses) | Generally safe; avoid with liver disease | Dietary supplement |
| Melatonin | Circadian regulator | Meta-analysis supported (mild effect on sleep latency) | 0.5–3 mg at bedtime | Low (at low doses); moderate at high doses | Safe short-term; limited long-term data | Dietary supplement |
| Diphenhydramine | Sedative only (histamine blockade) | Limited; tolerance develops rapidly | 25–50 mg at bedtime | High (hangover effect) | Avoid in elderly (Beers Criteria); caution with glaucoma, urinary retention | FDA-regulated OTC drug |
| Doxylamine | Sedative only (histamine blockade) | Limited; tolerance develops rapidly | 6.25–25 mg at bedtime | High (hangover effect) | Avoid in elderly; caution with glaucoma, urinary retention | FDA-regulated OTC drug |
Safety Caveats, Red Flags, and When to See a Doctor
No OTC sleep aid should be used as a long-term solution for chronic insomnia. The clinical first-line treatment for chronic insomnia, per AASM guidelines, is Cognitive Behavioral Therapy for Insomnia (CBT-I). OTC options are best understood as short-term or adjunctive tools.
- Avoid antihistamines in older adults: The Beers Criteria explicitly warns against diphenhydramine and doxylamine due to anticholinergic risks, including confusion, falls, and potential dementia association.
- Pregnancy and breastfeeding: Most OTC sleep aids lack robust safety data for pregnancy. Doxylamine is sometimes used for nausea in pregnancy, but always consult a healthcare provider before using any sleep aid while pregnant or nursing.
- Interaction risks: Valerian root can potentiate the effects of benzodiazepines and other CNS depressants. If you are already taking medication for anxiety or depression, talk to your doctor before adding a supplement.
- Duration of use: If you find yourself relying on any OTC sleep aid for more than 2–4 weeks, or if your anxiety symptoms are severe (including panic attacks or suicidal ideation), it is time to seek professional evaluation.
For a detailed explanation of the non-pharmacological first-line treatment, see our FAQ on CBT-I for Insomnia.
The most effective strategy for anxiety-related insomnia is rarely a single ingredient. It is a layered approach: using a GABAergic supplement like L-theanine or magnesium glycinate to take the edge off at night, combined with good sleep hygiene and, if needed, professional support like CBT-I. Understanding the mechanism behind your choice is the first step toward breaking the cycle.


Comments
Join the discussion with an anonymous comment.