A home sleep test usually costs far less upfront than an in-lab sleep study. Current cash-pay home sleep tests often fall around $100–$1,000, with several direct-to-consumer options advertised at flat prices around $189–$349 that include physician interpretation; insured patients may pay roughly $0–$200 depending on the plan. In-lab polysomnography is a different bill entirely: a commonly cited national average is about $3,000, with real-world prices ranging from about $1,000 to more than $10,000 when hospital facility charges are involved. [1][2]
That makes the first answer to “home sleep test vs lab sleep study cost” easy: the home test is usually cheaper at the beginning. The harder and more useful answer is whether it is cheaper after the whole diagnostic path is finished. If a home test is negative, inconclusive, or not appropriate for your health situation, the next step may still be an in-lab study. At that point, the low first invoice can become a down payment on a longer route.

The Cost Comparison Most People Actually Need
| Cost situation | Home sleep test | In-lab sleep study |
|---|---|---|
| Typical cash-pay or out-of-pocket range | About $100–$1,000 | About $1,000–$10,000+ |
| Common direct-to-consumer flat pricing | About $189–$349, often including physician interpretation | Not usually sold as a simple flat online price |
| Often-cited national average | Varies by vendor and insurance plan | About $3,000 |
| Possible insured patient cost | About $0–$200 after plan cost-sharing | Can still be hundreds or thousands, especially before a deductible is met |
| Medicare Part B context | Covered when medically necessary, with Part B cost-sharing rules | Covered when medically necessary, with Part B cost-sharing rules |
| Main financial risk | A negative or inconclusive result may lead to a second, in-lab test | Higher upfront bill, plus separate facility, interpretation, or titration charges |
For Medicare beneficiaries in 2026, the basic Part B math matters. Medicare Part B generally covers 80% of the Medicare-approved amount for covered sleep testing after the annual $283 deductible is met, leaving the patient responsible for the remaining cost-sharing unless supplemental coverage applies. [3]
Private insurance can make either test look inexpensive or expensive depending on timing. A person with a high-deductible plan early in the year may be quoted a covered lab study and still owe a large share of the negotiated price before coinsurance begins. Sleep Foundation’s insurance guidance notes that coverage depends on medical necessity, prior authorization, deductibles, copays, and coinsurance, not simply on whether a sleep study is “covered.” [4]
That distinction is where many bad cost estimates start. “Covered” tells you the service is eligible for payment under the plan. It does not tell you whether the bill lands at $40, $400, or $1,400.
Why the Home Test Usually Wins on the First Bill
Home sleep apnea testing removes several expensive pieces from the visit. There is no overnight lab room, no hospital bed, no technologist monitoring you through the night, and usually no separate facility charge attached to the location. The device is mailed or picked up, worn at home, returned or uploaded, and interpreted by a qualified clinician.
That simpler setup is why current home-test pricing can be concrete enough to budget around. Sleeplay’s 2026 cost guide places home sleep tests around $100–$1,000 out of pocket and describes insured patient costs around $0–$200 after cost-sharing. It also reflects the direct-pay market, where flat advertised prices commonly sit in the $189–$349 range. [1]
Those flat prices can be attractive because they answer a question medical billing often avoids: “What will this cost before I agree to it?” For an uncomplicated adult with suspected obstructive sleep apnea, a home test can be the financially cleanest first step if the ordering clinician agrees it is appropriate.
The Lab Study Bill Is Not Always One Bill
In-lab polysomnography costs more partly because it does more. A lab can monitor more signals, document sleep stages, observe breathing and movement in a controlled setting, and respond when the test needs closer supervision. For some patients, that is not luxury; it is the safer and more informative first test.
The billing problem is that the advertised or estimated price may not include every charge a patient later sees. Sleep study cost breakdowns commonly separate the technical or facility portion from professional interpretation, and hospital-based studies can carry facility fees that push the final amount much higher than an independent sleep center. iSLEEP’s cost breakdown also flags second-night CPAP titration as a possible added expense, with some components adding hundreds to thousands of dollars beyond the initial diagnostic study. [5]

The charges to ask about are plain, but they are easy to miss:
- Facility fee: the charge for using the hospital or sleep-lab setting.
- Technical fee: the cost of the equipment, overnight monitoring, and staff support.
- Professional interpretation fee: the sleep physician’s charge for reading the study.
- Second-night titration: a separate night used to adjust CPAP pressure when it is not done during the first study.
- Prior authorization or network issues: not a fee by itself, but a reason an expected covered amount can change.
A quote that includes only the sleep center’s technical charge is not the same as an all-in patient estimate. If the lab is hospital-based, it is worth asking whether the estimate includes both the hospital/facility side and the physician interpretation side.
When the Cheaper Home Test Can Cost More
The financial trap is not that home tests are secretly expensive. It is that they can be incomplete for the wrong patient or the wrong clinical question. A negative home test does not always end the diagnostic process, especially when symptoms remain convincing.
Everything Sleep Idaho summarizes an AASM-cited false-negative estimate of up to 17% for home sleep apnea testing, while also noting that performance varies by device type and patient factors. That estimate should not be treated as a guarantee that any one device will miss 17% of cases. It is a warning about the pathway: a home test can come back negative even when obstructive sleep apnea is still clinically suspected. [6]
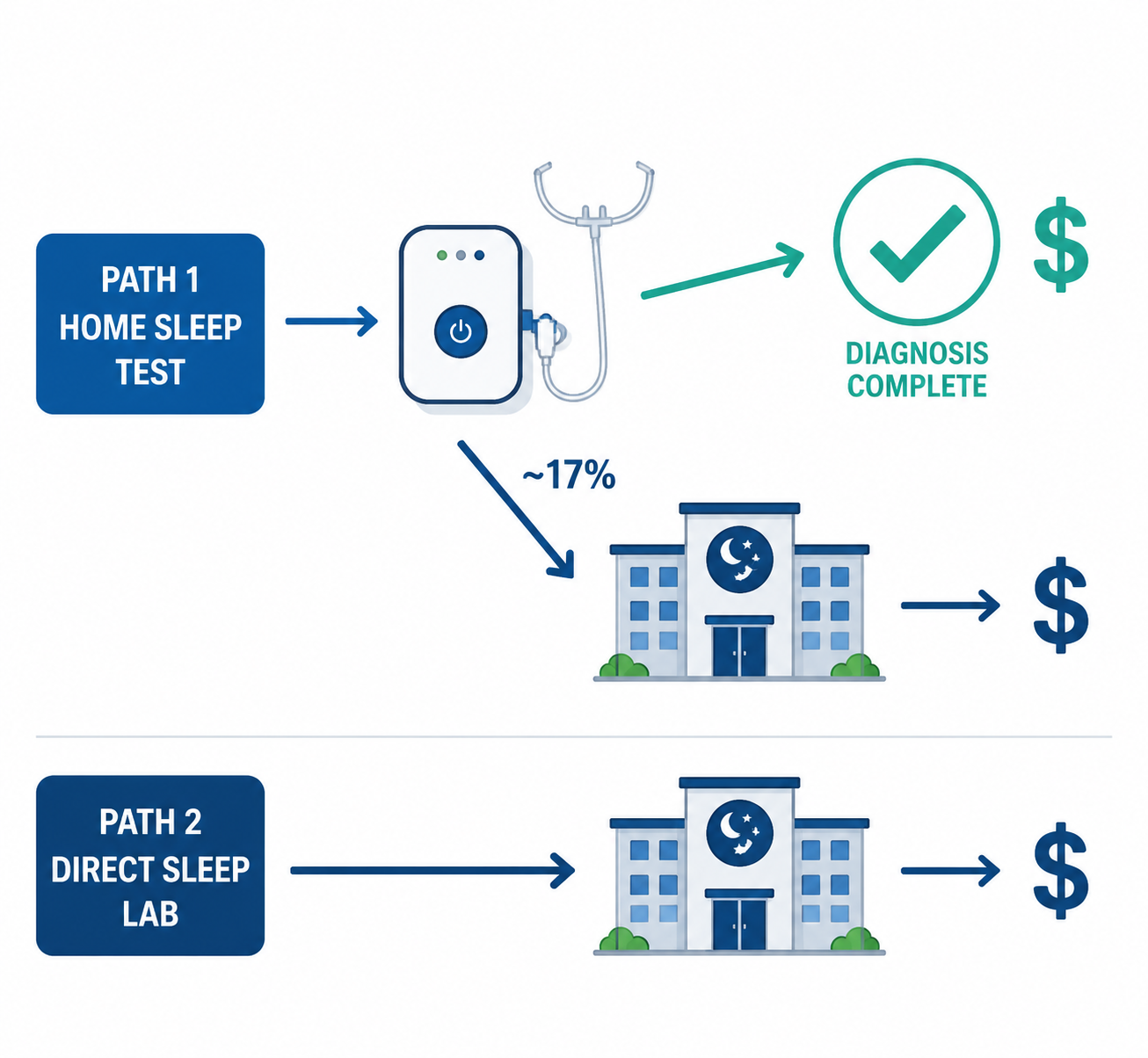
A simple hypothetical shows the cost problem without pretending every patient will follow the same route. Suppose a person pays a flat cash price for a home test. If the result clearly confirms obstructive sleep apnea and the clinician accepts it, that may be the end of diagnostic spending. If the result is negative or inconclusive but symptoms remain strong, the clinician may recommend an in-lab study anyway. The total diagnostic cost then becomes the home test plus the lab study, not one or the other.
That is how a “cheap” first test can produce a $1,000+ diagnostic path. It is not because the home device was overpriced; it is because the first answer did not settle the question.
The HomePAP randomized trial helps frame this without overselling it. In that study, a home-based pathway cost payers $1,575 per patient compared with $1,840 for the laboratory pathway, a $264 difference. The study is useful because it compares diagnostic pathways rather than just device prices, but its absolute dollar figures come from 2011 Medicare rates and the trial excluded complex patients, so it should not be read as a current household bill estimate. [7]
The lesson from HomePAP is more modest and more practical: home-based diagnosis can reduce payer costs in selected patients, but the savings are not infinite, and they depend on choosing patients for whom the home pathway is likely to give a usable answer.
Accuracy Claims Need a Label
Some home-test devices perform better than others, and some use different signals than a basic airflow-and-oxygen setup. Everything Sleep Idaho cites WatchPAT One validation data showing about 98% correlation with in-lab polysomnography, but that is a technology-specific point about PAT-signal testing. It should not be stretched into “all home sleep tests are 98% as accurate as a lab.” [6]
That matters financially because accuracy is not an abstract quality score. It affects whether the first test gives a clinician enough confidence to diagnose, rule out, or escalate. A cheaper test that answers the question is a bargain. A cheaper test that cannot answer the question becomes another line item.
Who Is Most Likely to Save With a Home Test?
Home sleep apnea testing is most financially attractive when the patient looks like the person it is designed to evaluate: an adult with a high suspicion of uncomplicated obstructive sleep apnea and without major conditions that make the result harder to interpret.
Clinical appropriateness guidance is narrower than the advertising copy around home testing sometimes makes it sound. ENTtoday’s discussion of test selection emphasizes that home sleep apnea testing fits selected patients with suspected obstructive sleep apnea, while in-lab testing is more appropriate when there are complicating medical conditions, concern for other sleep disorders, or a need for more complete physiologic monitoring. [8]
That is not a defense of expensive testing for its own sake. It is a way to avoid paying twice. If a clinician already believes a lab study will be needed because of heart or lung disease, neuromuscular disease, significant insomnia, suspected central sleep apnea, unusual movements, or a prior inconclusive test, the home-test savings may be less real than they look.
How to Get a Real Estimate Before You Choose
The best cost question is not “How much is the test?” It is “What will I owe if this is the only test, and what will I owe if it is not enough?”
- Ask the ordering clinician: “Am I an uncomplicated suspected obstructive sleep apnea patient, or is there a reason a lab study is more appropriate first?”
- Ask the home-test provider: “Does the price include the device, shipping, physician interpretation, and a written report?”
- Ask the sleep lab: “Is this estimate all-in, including facility, technical, and physician interpretation fees?”
- Ask the insurer: “What is my expected out-of-pocket cost after deductible, copay, coinsurance, and network rules?”
- Ask about the fallback: “If the home test is negative or inconclusive, will I likely need an in-lab study, and would that require a new authorization?”
Those questions are boring in exactly the right way. They turn a vague promise of coverage into a path estimate.
The Bottom Line on Home Sleep Test vs Lab Sleep Study Cost
For many cost-sensitive adults with straightforward suspected obstructive sleep apnea, a home sleep test is the lower-cost first diagnostic step. The upfront gap is real: roughly $100–$1,000 for home testing, often $189–$349 in direct-pay flat-rate offers, compared with a lab-study range that can run from about $1,000 to more than $10,000. [1][2]
But the cheapest first charge is not always the cheapest completed diagnosis. If the home result is negative, inconclusive, or clinically insufficient, the lab study may still be waiting at the end of the path. The better standard is to choose the test that is cheapest for the likely complete sequence, not the one with the smallest first invoice.
If you are still deciding whether your symptoms justify testing, start with this obstructive sleep apnea overview. If you want the broader patient path from symptoms to diagnosis and treatment, use the sleep apnea FAQ. And if a watch or wearable nudged you toward testing, read how an Apple Watch sleep apnea alert differs from a clinical diagnosis before treating the alert as an answer.
References
- Home Sleep Test Cost 2026: Prices, Insurance & Medicare — Sleeplay.
- How Much Does a Sleep Study Cost? — Sleep Foundation.
- 2026 Medicare Costs — Medicare.gov.
- Are Sleep Studies Covered by Insurance? — Sleep Foundation.
- Sleep Study Cost Breakdown: Lab vs Home Test Pricing — iSLEEP.
- Lab Sleep Study (Polysomnography) versus Home Sleep Test (HSAT) — Everything Sleep Idaho.
- An Economic Evaluation of Home Versus Laboratory-Based Diagnosis of Obstructive Sleep Apnea — PMC, 2015.
- What Type of Sleep Study Is Best for My Patient? — ENTtoday.
Comments
Join the discussion with an anonymous comment.