
Introduction: The Frustration of Doing Everything Right
You have done everything the articles say. You go to bed at the same time every night, even on weekends. You banished screens an hour before bed, switched to decaf after 2 p.m., and made your bedroom a cool, dark cave. You have followed the checklist to the letter. And yet, you are still lying awake at 2 a.m., staring at the ceiling, wondering what you are doing wrong.
This experience is far more common than most people realize. According to data from roughly 160,000 Sleep Foundation profiles, more than two-thirds of respondents have experienced poor sleep for a period of months to years. The frustration is real, and it is not your fault. The problem is not that you are failing at sleep hygiene. The problem is that sleep hygiene, on its own, has real, evidence-based limitations that are rarely discussed in the standard advice.
This article will explain why healthy sleep habits are not enough for everyone, what the research actually says about their limits, and what to try instead when you have already optimized your environment and schedule.
What Sleep Hygiene Actually Treats — And What It Doesn't
Sleep hygiene is a collection of behavioral and environmental recommendations designed to promote good sleep. These include maintaining a consistent sleep schedule, avoiding caffeine and alcohol before bed, creating a comfortable sleep environment, and limiting exposure to bright light in the evening. For many people, these practices are genuinely helpful. They address lifestyle-driven disruptions: the person who drinks coffee after dinner, keeps a bright phone screen in bed, or sleeps in a noisy room.
But there is a widespread misconception that sleep hygiene alone can treat insomnia. The Harvard Sleep Medicine page directly addresses this under its "Truth or Myth" section. It states clearly that "implementing better sleep hygiene can treat insomnia" is a myth. The page explains: "Although it is beneficial for all to adopt healthy sleep hygiene practices, insomnia cannot be treated with better sleep hygiene alone."
So what does sleep hygiene actually treat? It is most effective for situational, mild sleep difficulties caused by poor habits or a suboptimal environment. If you have recently started drinking coffee later in the day, or if your bedroom has become too warm or bright, improving your sleep hygiene will likely help. But if you have maintained good sleep habits for weeks or months and still struggle to fall asleep, stay asleep, or feel rested, your problem is likely not a hygiene problem.
For readers who want a complete review of the fundamentals, see our guide on Sleep Hygiene Fundamentals and an Evidence-Based Bedtime Routine. The rest of this article will focus on what comes next.
The Research Gap: Why Sleep Hygiene Education Falls Short Alone
The idea that sleep hygiene education alone is insufficient for treating clinical insomnia is not just expert opinion. It is supported by a growing body of research. A 2025 systematic review on sleep hygiene education for insomnia found that, while it can improve knowledge about sleep, its standalone efficacy for treating chronic insomnia is limited. The review concluded that sleep hygiene education should be considered a foundational component of sleep health, but not a standalone treatment for insomnia disorder.
Additional evidence comes from a 2023 cross-sectional study published in PMC (Alanazi et al., n=384 adults). The study found that 55.5% of participants reported poor sleep hygiene practices. However, the more telling finding was that even among those with good sleep hygiene practices, 56.1% still reported problems sleeping during the past three months. In contrast, 76.5% of those with poor hygiene reported sleep problems. This means that while poor hygiene clearly worsens sleep, good hygiene does not guarantee good sleep.
The study also found that rates of excessive daytime sleepiness were significantly higher among individuals with poor hygiene practices (22.5% vs. 11.7% for moderate sleepiness, and 5.2% vs. 1.2% for severe sleepiness). This reinforces the idea that hygiene matters for overall sleep health, but it is not a cure-all.
The Mechanism Gap: Why Hyperarousal and Conditioned Insomnia Persist
To understand why sleep hygiene has limits, it helps to understand what causes chronic insomnia in the first place. Two key mechanisms are at play: hyperarousal and conditioned insomnia.
Hyperarousal is a state of heightened physiological and cognitive activation. People with chronic insomnia often have elevated heart rate, body temperature, and cortisol levels at night compared to good sleepers. Their brains remain in a state of alertness that is incompatible with sleep. Sleep hygiene — dimming lights, avoiding caffeine — cannot directly address this underlying physiological arousal.
Conditioned insomnia is a learned response. After many nights of lying awake in bed, the brain begins to associate the bed with wakefulness, frustration, and anxiety rather than with sleep. The bed itself becomes a cue for being alert. This is why someone with conditioned insomnia may feel perfectly sleepy on the couch but become wide awake the moment they get into bed. No amount of blackout curtains or consistent scheduling can undo this learned association.
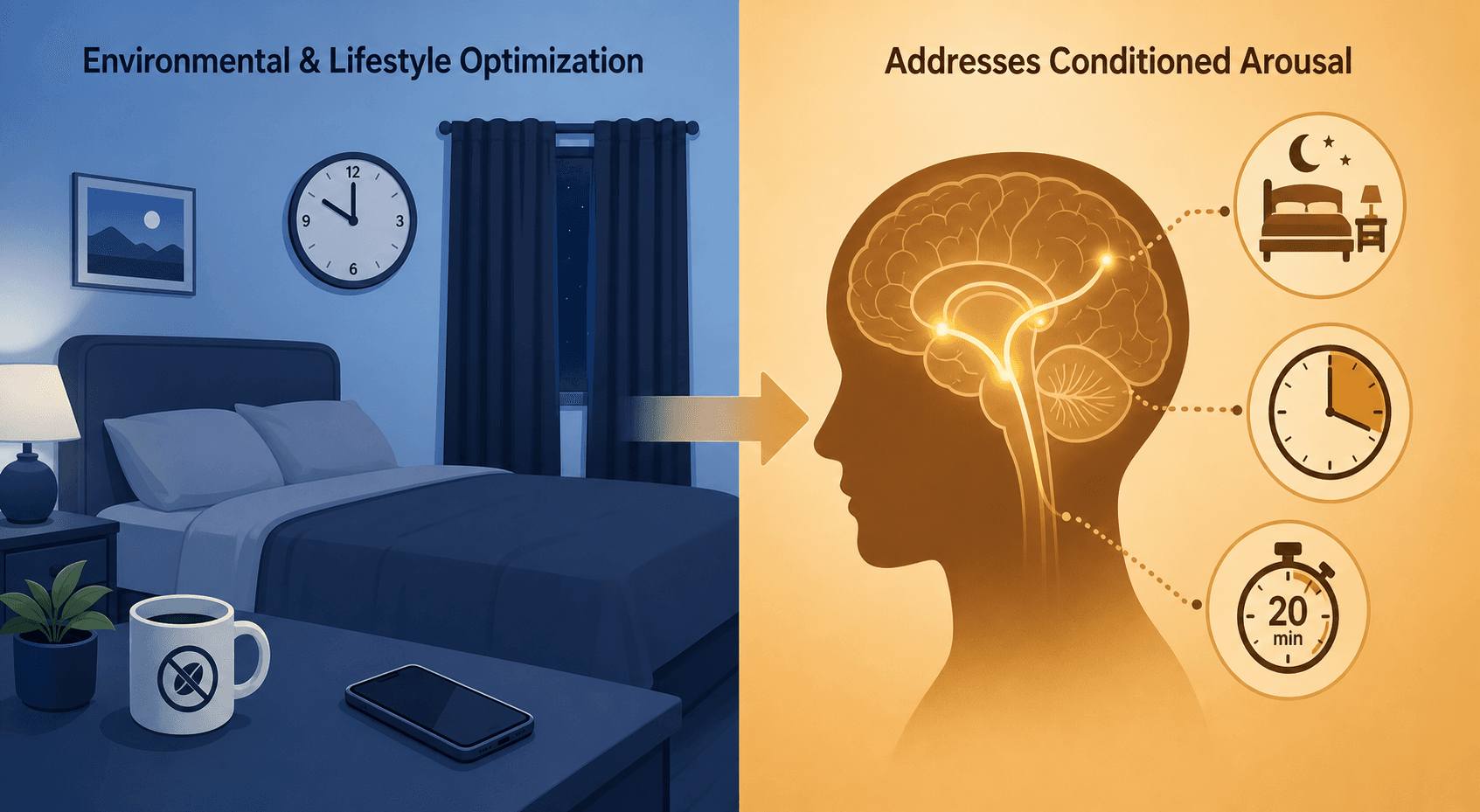
Sleep hygiene addresses the external environment and daily habits. It does not address the internal, learned, or physiological mechanisms that maintain insomnia. This is the mechanism gap, and it is the reason why so many people who "do everything right" still cannot sleep.
The Real First-Line Intervention: Introducing CBT-I Components
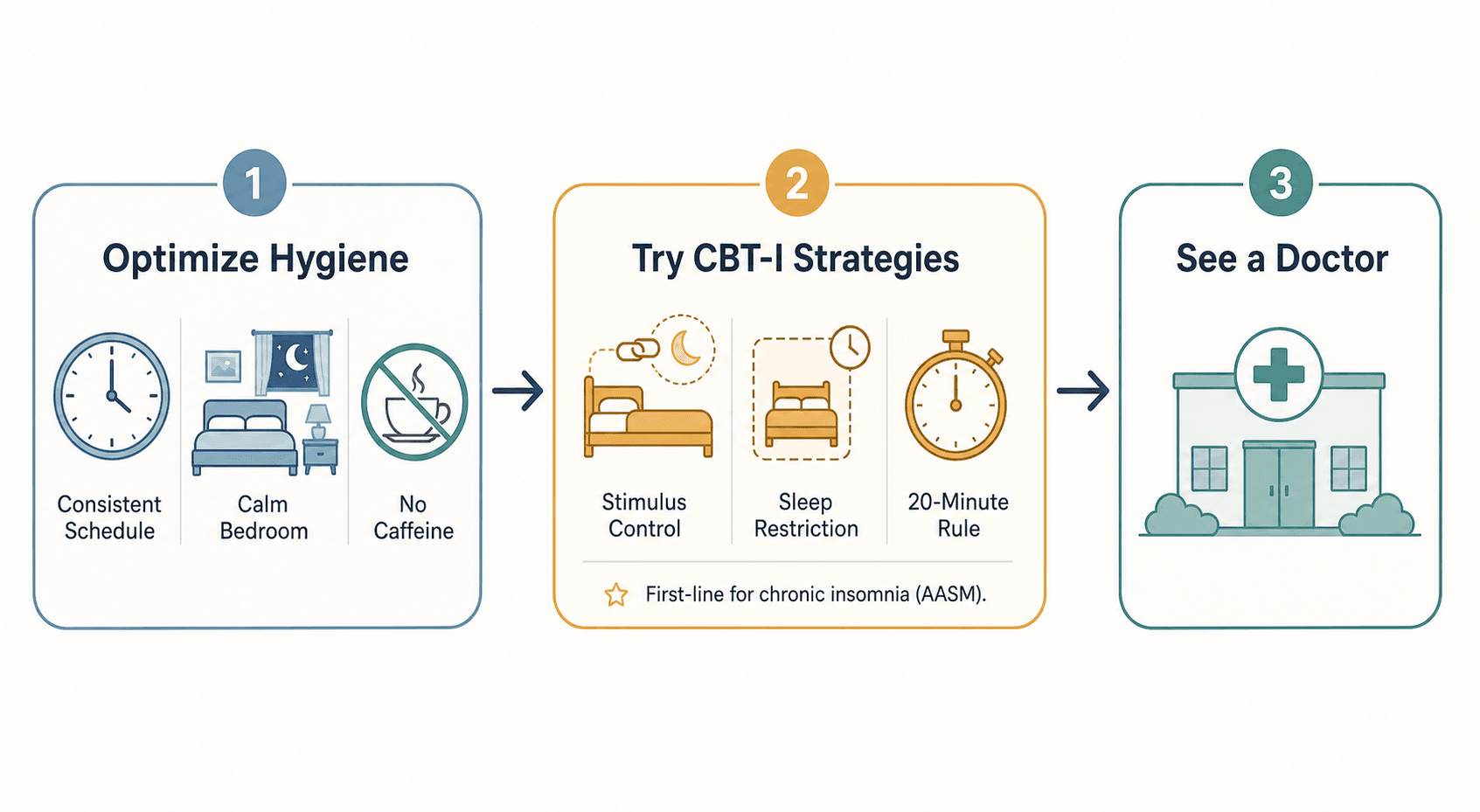
If sleep hygiene is not the answer for chronic insomnia, what is? The answer, backed by the American Academy of Sleep Medicine (AASM) and multiple clinical guidelines, is Cognitive Behavioral Therapy for Insomnia (CBT-I). CBT-I is a structured, multi-component therapy that directly addresses the mechanisms that sleep hygiene cannot touch.
CBT-I is not a single technique. It is a combination of behavioral, cognitive, and educational components. The three most powerful behavioral components are:
- Stimulus Control: This is the most direct treatment for conditioned insomnia. The goal is to rebuild the association between the bed and sleep. The core rules include: only go to bed when sleepy; get out of bed if you cannot fall asleep within about 20 minutes; use the bed only for sleep and sex; and wake up at the same time every day regardless of how much you slept. For a full breakdown, see our guide on Stimulus Control Therapy for Insomnia.
- Sleep Restriction Therapy: This component addresses the fragmented, light sleep that often results from spending too much time in bed. By initially limiting the time spent in bed to match the actual amount of sleep a person gets, sleep becomes more consolidated. Over time, the time in bed is gradually increased as sleep efficiency improves.
- The 20-Minute Rule: This is a practical application of stimulus control. The Sleep Foundation recommends that "if you have spent around 20 minutes in bed and are having trouble sleeping, it is best to get out of bed and do something relaxing in low light, and then return to bed once you feel tired." This breaks the cycle of lying in bed frustrated and reinforces the bed-sleep association.
A Practical Decision Framework: When to Optimize, When to Escalate, When to See a Doctor
Knowing what to do next depends on the severity and duration of your sleep difficulties. The following framework can help you decide which path is right for you.
| Your Situation | What to Do | Typical Timeframe |
|---|---|---|
| Mild, situational sleep issues (e.g., after a stressful event, travel, or a temporary schedule change) | Optimize sleep hygiene. Review the fundamentals and address any obvious environmental or behavioral factors. | 1–2 weeks |
| Persistent difficulty falling asleep or staying asleep despite good sleep hygiene for 2–4 weeks | Try CBT-I strategies. Begin with stimulus control and the 20-minute rule. Consider sleep restriction if sleep is fragmented. | 2–6 weeks for initial improvement |
| Chronic insomnia (symptoms occurring at least 3 nights per week for 3 months or more) | Seek professional help. Find a CBT-I trained provider or use a structured digital CBT-I program. Consult your primary care doctor. | Varies; CBT-I typically requires 4–8 sessions |
| Suspected sleep disorder (e.g., loud snoring, gasping for air, restless legs, or excessive daytime sleepiness despite adequate sleep) | See a doctor. These symptoms may indicate sleep apnea, restless legs syndrome, or another condition requiring medical evaluation. | As soon as possible |
| Sleep difficulties with co-occurring mental health concerns (anxiety, depression, or high stress) | See a doctor or mental health professional. Treating the underlying condition is often necessary for sleep to improve. | As soon as possible |
The Harvard Sleep Medicine page offers a practical benchmark: "if no improvement has been achieved after 2-4 weeks, seek proper treatment." This is a useful rule of thumb. If you have been diligently following sleep hygiene for a month with no meaningful change, it is time to escalate.
For a broader view of what works at each level of severity, see our Evidence-Based Sleep Improvement Hierarchy and our Insomnia Self-Care guide.
Closing: Self-Compassion and the Path Forward
If you have been struggling with sleep despite doing everything "right," please hear this clearly: it is not your fault. The limitations of sleep hygiene are a feature of the science, not a reflection of your effort or willpower. You have not failed. You have simply reached the boundary of what one set of tools can do.
The path forward is not about trying harder. It is about using the right tools for the right problem. For many people, that means moving from optimizing the environment to retraining the brain's relationship with sleep through CBT-I. For others, it means seeking medical evaluation for an underlying condition.
Seeking CBT-I or medical care is not a sign of defeat. It is a sign of informed self-advocacy. You recognized that the first-line advice was not enough, and you are looking for the next, more effective step. That is exactly the right thing to do.
Comments
Join the discussion with an anonymous comment.