How Common Is Insomnia and Why a Calibrated Approach Matters
Insomnia is not a niche complaint. A 2025 systematic review of 18 studies involving 262,582 participants estimated the global adult prevalence at 16.2%, representing roughly 852 million adults worldwide. Of those, about 7.9% — approximately 415 million adults — experience severe insomnia. In the U.S. and other high-income countries, up to two-thirds of adults report occasional insomnia symptoms at some point, and 10–15% meet criteria for chronic insomnia.
These numbers matter because they reveal a fundamental mismatch: millions of people need help, but the vast majority will never see a sleep specialist. Most will turn to self-care first — and they should. The problem is that self-care advice for insomnia is often presented as a flat list of equally effective options, when the evidence clearly shows a hierarchy of effectiveness.
This article organizes insomnia self-care into three calibrated tiers based on the strength of the supporting evidence. The goal is to help you match the intensity of your self-care strategy to the severity of your symptoms — and to recognize when self-care has reached its limit.
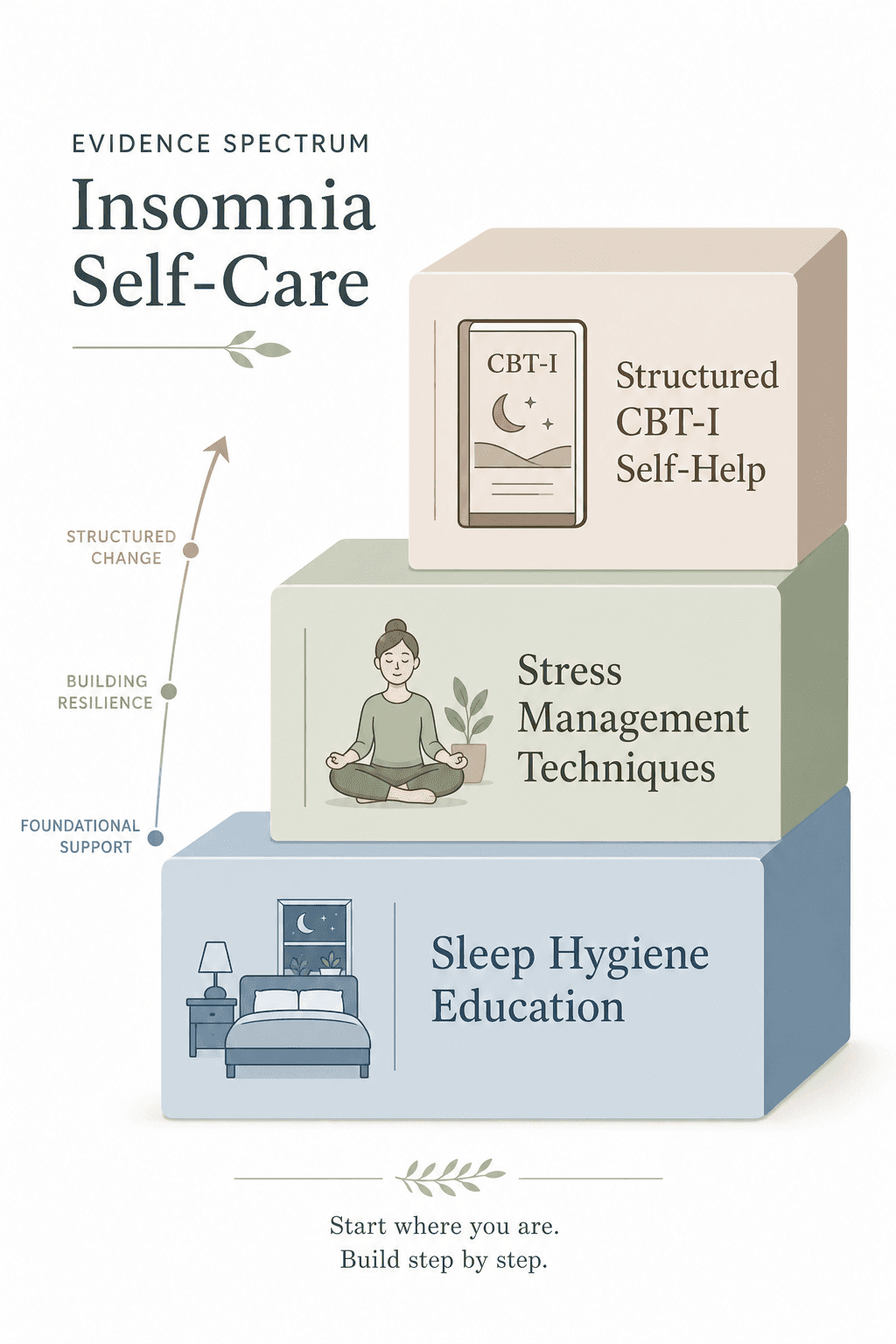
Level 1: Sleep Hygiene Education — A Modest but Real Foundation
Sleep hygiene education (SHE) is the most commonly recommended first step for insomnia. It typically covers maintaining a consistent sleep schedule, creating a cool and dark bedroom environment, avoiding caffeine and alcohol near bedtime, and limiting screen exposure before sleep.
A 2025 meta-analysis of 42 randomized controlled trials involving 4,245 adults (65.5% female) provides the clearest picture yet of what SHE alone can achieve. The analysis found that sleep hygiene education as a standalone intervention reduced Insomnia Severity Index (ISI) scores by a mean difference of 3.4 points from pre- to post-treatment. That is a small-to-moderate effect — real enough to matter for someone with mild symptoms, but unlikely to resolve moderate or severe insomnia.
The more important finding is comparative. When SHE was measured against full cognitive behavioral therapy for insomnia (CBT-I), the between-group difference was 3.8 points on the ISI — meaning CBT-I outperformed SHE by a margin roughly equal to SHE's total effect. SHE was also inferior to partial CBT-I (between-group MD of 4.5 points), exercise interventions (MD of 2.9 points), and even acupressure (MD of 1.9 points).
What this means in practice: if your insomnia is mild — you have trouble falling asleep a few nights per month but function reasonably well during the day — starting with sleep hygiene education is a sensible first step. You can find a detailed breakdown of the fundamentals in our Sleep Hygiene Fundamentals and an Evidence-Based Bedtime Routine guide. But if your symptoms are more frequent or more disruptive, you should not expect sleep hygiene alone to be sufficient.
Level 2: Stress Management Techniques for Pre-Sleep Cognitive Arousal
Many people with insomnia describe the same experience: they are physically tired, but their mind will not stop racing. This is cognitive arousal — the inability to disengage from thoughts, worries, and mental planning at bedtime. Two stress management techniques have specific evidence for targeting this mechanism.
The To-Do List Writing Protocol
A 2017 polysomnography study by Scullin and colleagues tested a remarkably simple intervention. Fifty-seven healthy young adults (aged 18–30) were assigned to spend five minutes before bed writing either a to-do list of tasks to complete in the coming days or a journal entry about activities they had already completed. The group that wrote a specific to-do list fell asleep approximately nine minutes faster, with a Cohen's d effect size of 0.63 — a moderate-to-large effect.
The more specific participants were in their to-do list entries, the faster they fell asleep (r = −0.39, p = 0.04). The study controlled for stress levels, sleep history, and blood pressure, and the group difference remained significant after including these covariates.
Progressive Muscle Relaxation (PMR)
Johns Hopkins sleep expert Luis F. Buenaver, Ph.D., recommends a progressive muscle relaxation protocol of 20–25 minutes of gentle breathing and systematic muscle tensing and releasing, practiced daily for two weeks. The goal is to activate the parasympathetic relaxation response, which reduces circulating stress hormones (cortisol and adrenaline), slows heart rate and breathing, and shifts the nervous system out of the hyperarousal state that maintains insomnia.
A national survey cited by Johns Hopkins found that 44% of adults reported stress had caused sleepless nights in the past month, underscoring the relevance of stress management as a targeted insomnia intervention.
Level 3: Structured Self-Help CBT-I — The Closest You Can Get to Professional Treatment on Your Own
Cognitive behavioral therapy for insomnia is the first-line treatment recommended by the American College of Physicians, the American Academy of Sleep Medicine, and the NHS. When delivered by a trained clinician, multicomponent CBT-I produces improvement in 70–80% of patients with primary insomnia, including measurable reductions in sleep onset latency and increases in total sleep time.
The good news is that you do not necessarily need a clinician to access the core components of CBT-I. Structured self-help formats — digital programs, smartphone apps, and guided self-help books — deliver the same active ingredients (stimulus control, sleep restriction, cognitive restructuring, and sleep hygiene education) in a self-paced format. Meta-analyses have found that digital CBT-I produces outcomes similar to face-to-face approaches.
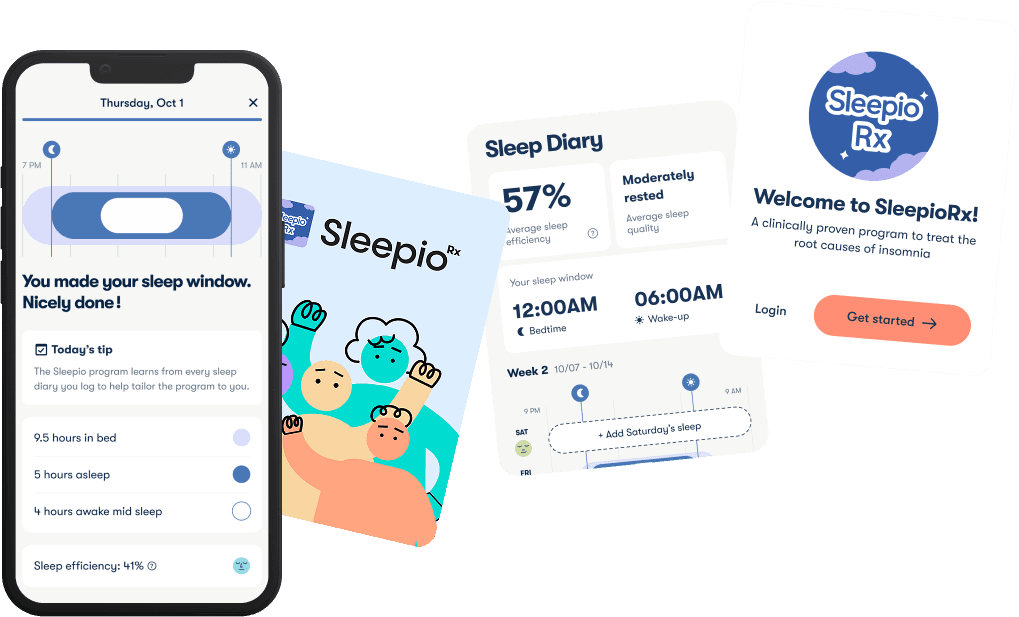
Sleepio: A Real-World Digital CBT-I Program
NHS Scotland offers the Sleepio digital program as a free six-week CBT-I intervention. As of 2024, over 80,000 people in Scotland had used the program, and 67% of patients experienced clinical improvement in their insomnia symptoms. The program covers stimulus control (using the bed only for sleep, getting up if awake for more than 10 minutes), consistent wake times, and behavioral adjustments such as avoiding caffeine after midday and alcohol within roughly four hours of bedtime.
CBT-I Coach: A Free VA App
The CBT-I Coach app, developed by the U.S. Department of Veterans Affairs, provides another free, structured self-help option. It includes sleep tracking, a sleep restriction scheduler, stimulus control guidance, and cognitive restructuring exercises. Like Sleepio, it is designed to be used either as a standalone tool or alongside clinician-delivered therapy.
For readers with co-occurring conditions — depression, anxiety, chronic pain — self-help CBT-I may still be effective, but the evidence base is more nuanced. Our CBT-I for Comorbid Insomnia article covers when self-help is appropriate and when professional guidance becomes necessary for people managing multiple conditions.
How to Choose Your Self-Care Level: A Decision Framework
The most common mistake people make with insomnia self-care is using a Level 1 strategy when they need Level 3. The table below provides a structured way to match your symptom profile to the appropriate self-care intensity.
| Factor | Level 1 (Sleep Hygiene) | Level 2 (Stress Management) | Level 3 (Self-Help CBT-I) |
|---|---|---|---|
| Symptom frequency | Occasional (a few nights per month) | 1–3 nights per week | 3+ nights per week |
| Symptom duration | Less than 1 month | 1–3 months | 3+ months (chronic) |
| Daytime impact | Mild fatigue, no functional impairment | Noticeable fatigue, some concentration difficulty | Significant impairment in work, mood, or safety |
| Response to lower levels | N/A (starting point) | Partial improvement from Level 1 | Insufficient improvement from Level 1 or 2 |
| Expected ISI improvement | ~3–4 points | Variable; no meta-analytic estimate available | Approaches 70–80% clinical improvement rate |
| Best suited for | Mild, situational insomnia | Stress-precipitated insomnia with cognitive arousal | Chronic insomnia with sleep maintenance or onset problems |
If you fall into the Level 1 column, start with sleep hygiene education and monitor your ISI score (a free self-assessment tool) over two to four weeks. If you are in the Level 2 column, add a stress management technique like the to-do list writing protocol or PMR. If you are in the Level 3 column, skip directly to structured self-help CBT-I — you are unlikely to get sufficient relief from the lower tiers alone.
When Self-Care Is Not Enough: Red Flags and Next Steps
Self-care has limits. If you have been consistent with a Level 3 self-help CBT-I program for six to eight weeks and your ISI score has not improved by at least 4–5 points, or if your symptoms have persisted for three months or longer despite your best efforts, it is time to escalate.
The following red flags warrant professional evaluation regardless of how long you have been trying self-care:
- Loud snoring, gasping for air, or witnessed pauses in breathing during sleep (possible sleep apnea)
- Uncontrollable urge to move your legs in the evening (possible restless legs syndrome)
- Falling asleep while driving or during other safety-critical activities
- Symptoms of depression, anxiety, or other mental health conditions that are interfering with daily life
- Significant weight loss or gain, or other physical symptoms that accompany your sleep problems
If any of these apply, seek evaluation from a primary care provider or a sleep specialist. For chronic insomnia without red flags, the next step is referral to a qualified CBT-I clinician. The Society of Behavioral Sleep Medicine maintains a provider directory, and many therapists now offer CBT-I via telehealth, which has been shown to be as effective as in-person delivery.




Comments
Join the discussion with an anonymous comment.