Mechanism explainer
How Five Common Disruptors Destroy Your Sleep Architecture — And What Each One Costs
For adults who sleep eight hours yet wake unrefreshed, the problem is usually stage composition, not total duration — this deep-dive explains the mechanistically distinct ways alcohol, aging, sleep apnea, chronic insomnia, and stress each attack NREM and REM architecture, and maps those mechanisms to recognizable symptom signatures.
Eight hours in bed. Alarm goes off. You feel like you barely slept. If this sounds familiar, the problem almost certainly isn't your total sleep time — it's what happened inside those eight hours. Sleep isn't a uniform state that accumulates like water in a bucket. It's a sequence of distinct biological stages, each doing specific repair work that the others cannot substitute for.
A healthy night distributes roughly as follows: N1 (light transitional sleep) takes up about 5% of the night, N2 (spindle-rich intermediate sleep) about 45%, N3 slow-wave sleep about 25%, and REM about 25%. Lose the right proportion of any one stage and you pay a specific biological price — not just a generic sense of tiredness.
- N3 slow-wave sleep loss impairs tissue repair, glymphatic waste clearance from the brain, and insulin sensitivity.
- REM loss impairs emotional regulation and the consolidation of declarative and emotional memories.
- N2 spindle loss impairs procedural memory and the integration of newly learned motor and cognitive skills.
For the full biology of what each stage does — EEG signatures, thalamo-cortical mechanisms, cycle dynamics — see our guide to sleep architecture and the NREM and REM stages. This article picks up where that one leaves off: it focuses entirely on five specific disruptors — alcohol, aging, sleep apnea, chronic insomnia, and stress — and explains the mechanistically distinct way each one attacks your stage composition.
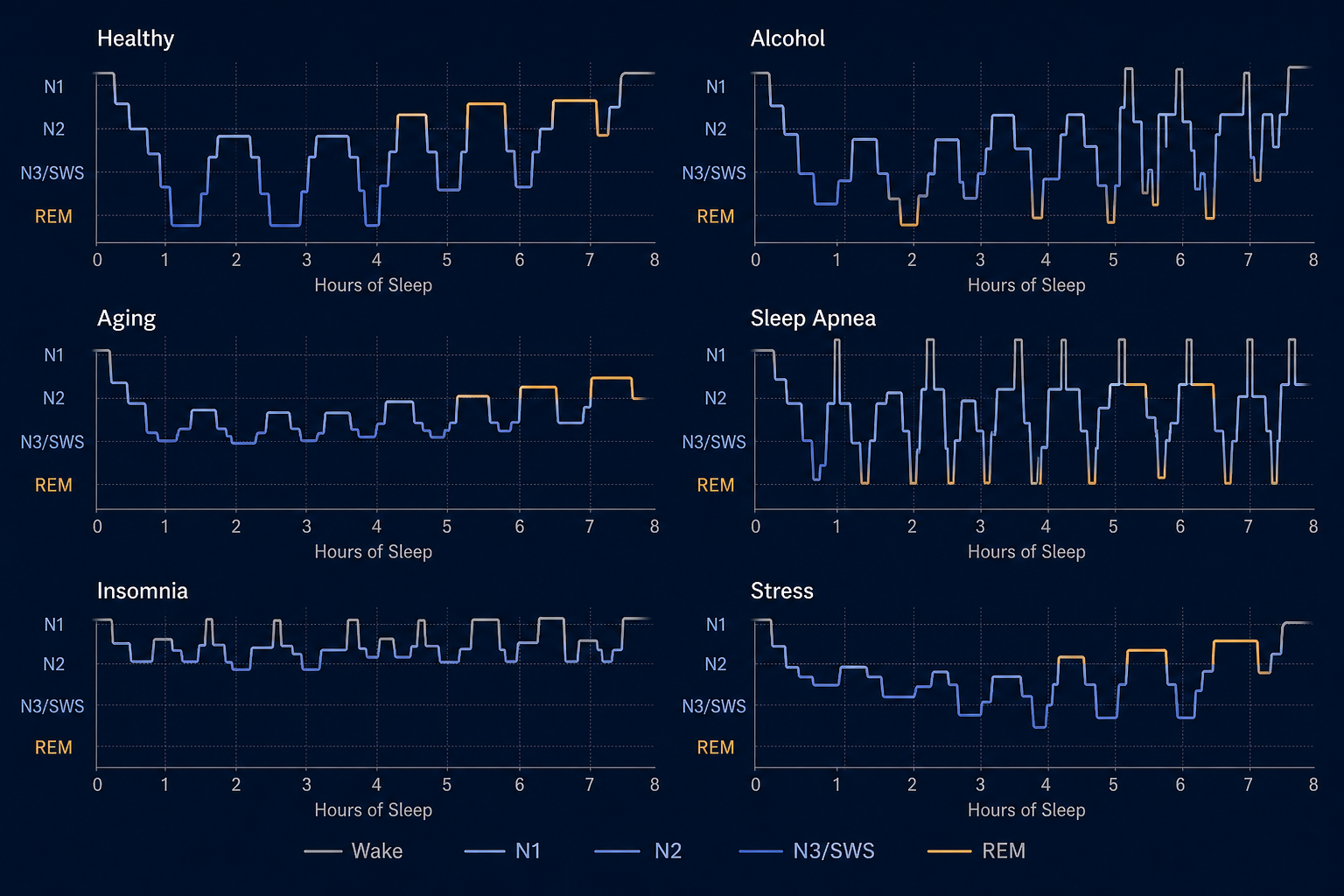
Disruptor 1 — Alcohol: The Two-Phase Architecture Trap
More than 10% of adults report using alcohol to fall asleep. The logic feels sound: alcohol is sedating, sleep onset is faster, and the first few hours feel deep. The problem is that alcohol doesn't produce normal sleep — it produces a counterfeit version that collapses in the second half of the night.
Alcohol's primary mechanism is GABA agonism: it facilitates tonic GABAergic neurotransmission, which suppresses cortical arousal and promotes slow-wave delta activity. Simultaneously, alcohol inhibits the equilibrative nucleoside transporter ENT1, blocking adenosine reuptake in the basal forebrain. This increases extracellular adenosine, which inhibits wake-promoting cholinergic neurons via A1 receptors — amplifying the NREM-promoting effect. The result in the first half of the night is increased SWS and suppressed REM, with longer REM latency and reduced REM duration.
Then blood alcohol begins to metabolize. As the GABA effect wanes, the suppressed REM pressure reasserts itself — but in a disorganized way. The second half of the night becomes fragmented, with increased wakefulness, more N1, and a compensatory REM rebound. The net result across the whole night is reduced total REM — despite feeling sedated at sleep onset. The architecture looks like a two-phase trap: artificially deepened in the first half, destabilized in the second.
In chronic alcohol dependence, the pattern inverts entirely. Long-term heavy use reduces SWS — with decreased delta power especially in frontal regions — while increasing REM pressure and blunting homeostatic sleep recovery. Abstinent alcoholics show consistently decreased SWS and elevated REM pressure, and during withdrawal, the adenosine signaling system is so downregulated that normal homeostatic sleep drive fails to accumulate. This is the primary mechanism of withdrawal insomnia.
The practical implication: even a single evening drink close to bedtime shifts stage composition in measurable ways. The sedation is real; the sleep quality is not.
Disruptor 2 — Aging: The Slow Erosion of Deep Sleep
Of all the age-related changes in sleep, the most clinically significant is the progressive decline in N3 slow-wave sleep. This isn't simply a matter of sleeping more lightly — it reflects measurable structural changes in the brain itself. Slow oscillations originate primarily in the prefrontal cortex, and as cortical gray matter thins with age, the neural machinery for generating deep sleep degrades. The result is that older adults spend less time in N3, more time in N1, and experience more frequent nighttime awakenings.
Some estimates, drawn largely from animal models and extrapolated to human aging trajectories, suggest that slow-wave sleep activity may decline by as much as 80% between early adulthood and age 70. Human studies confirm substantial SWS decline across adulthood, though the precise magnitude varies with methodology and population. What is consistent across studies is the direction and clinical significance of the change: by late middle age, many adults have meaningfully less N3 than they had at 25.
Sleep spindle density — a hallmark of N2 and a marker of memory consolidation capacity — also declines with age, compounding the cognitive consequences of reduced N3.
Two downstream consequences of age-related SWS loss deserve specific attention.
First, glymphatic clearance. During N3, slow oscillatory brain waves drive cerebrospinal fluid flux through the brain's interstitial spaces, clearing metabolic waste products including tau proteins and amyloid-beta aggregates. This system is primarily active during slow-wave sleep. With aging, AQP4 water channels — which line astrocyte end-feet and facilitate this clearance — become mis-localized, reducing clearance efficiency independent of the SWS duration reduction itself. Less N3, plus degraded channel function, compounds into substantially reduced overnight brain cleaning.
Second, insulin sensitivity. An experimental study in healthy young adults found that three consecutive nights of selective SWS suppression produced decreases in insulin sensitivity equivalent to levels reported in populations at high risk for type 2 diabetes — without producing a compensatory increase in insulin release. This study was conducted under controlled lab conditions in a specific population, so the magnitude should not be directly extrapolated to all adults, but the directional finding is consistent with broader epidemiological evidence linking poor sleep quality to metabolic disruption.
Disruptor 3 — Sleep Apnea: Perpetual Shallow Sleep
Obstructive sleep apnea (OSA) — the most common form — produces a specific architectural pattern that is easy to misread. Total time in bed looks adequate. The person may not recall waking. But the sleep staging record tells a different story: the night is punctuated by hundreds of brief arousals, each lasting roughly 10 to 15 seconds, each resetting the sleeper to lighter stages.
The mechanism is self-reinforcing. Airway muscle tone is lowest during deeper sleep states — N3 and REM — making these the stages most vulnerable to collapse. When collapse occurs, the arousal that follows interrupts the stage before the cycle can complete. The sleeper is pushed back into N1 or N2, and the cycle restarts. Over a full night, this prevents adequate accumulation of either slow-wave sleep or REM, even when total sleep time appears normal.
This is why the cognitive recovery from CPAP treatment can feel so dramatic. It isn't that CPAP is improving sleep beyond baseline — it's restoring architectural access to N3 and REM that was being systematically blocked. The brain hasn't lost the ability to generate deep sleep; it was being interrupted before it could complete.
A large-scale study using wearable sleep data from over 6,700 participants monitored across a median of 4.5 years found that both reduced REM sleep and reduced deep sleep were independently associated with incident atrial fibrillation. Importantly, most of these associations persisted after adjusting for previous sleep apnea diagnosis — suggesting the architectural disruption itself, not just the apnea label, carries independent cardiovascular relevance.
Disruptor 4 — Chronic Insomnia: When Sleep Itself Is Hyperaroused
Chronic insomnia is architecturally distinct from the other disruptors on this list. It doesn't simply reduce sleep duration or fragment specific stages through a mechanical process. Instead, it alters the quality of the sleep that does occur — from the inside.
The dominant explanatory framework is the hyperarousal model. People with chronic insomnia show elevated EEG beta activity — a marker of cortical arousal — not just during wakefulness, but during NREM sleep stages themselves. Even when the polysomnogram records N2 or N3, the brain's electrical activity reflects a state closer to drowsy wakefulness than genuine deep sleep. The stages are present by label; the depth is not.
This is what distinguishes insomnia's architectural signature from other disruptors. Alcohol reduces REM. Aging reduces N3 duration. Apnea interrupts both through repeated arousals. Chronic insomnia reduces stage stability and N3 depth while leaving REM duration relatively less affected — the characteristic pattern is elevated NREM beta power and shallow, unstable staging rather than outright stage elimination.
A key vulnerability factor is sleep reactivity — the degree to which stress disrupts sleep. This appears to be a trait-like diathesis: people with high sleep reactivity are two to three times more likely to develop insomnia following a stressful period. Critically, sleep system sensitization can occur even in people who start with low reactivity after sustained stress exposure — and elevated reactivity can persist after the insomnia itself remits, leaving a window of continued vulnerability.
The HPA axis is also dysregulated in chronic insomnia. Insomniacs show increased nocturnal cortisol secretion throughout the 24-hour cycle — not just during stress periods — which further suppresses slow-wave sleep activity and sustains the hyperarousal state. The cortisol elevation and the elevated NREM beta mutually reinforce each other, creating a self-perpetuating loop that makes insomnia architecturally self-sustaining even when the original stressor is gone.
Disruptor 5 — Stress and Cortisol: The HPA Axis Attack on Deep Sleep
Stress disrupts sleep architecture through a specific biological pathway — not through the same mechanism as insomnia's hyperarousal, though the two interact. The primary route is the HPA axis: psychological or physiological stress activates the hypothalamic-pituitary-adrenal axis, releasing glucocorticoids (primarily cortisol). Cortisol specifically suppresses slow-wave sleep activity — it is directly antagonistic to the conditions that generate N3.
The glymphatic pathway is also affected. Research in animal models has shown that chronic stress reduces glymphatic influx and efflux, causes loss of AQP4 channel polarization in astrocytes, and reduces the number of AQP4-bearing astrocytes overall. The mechanism: glucocorticoids decrease astrocyte numbers and downregulate AQP4 channels, directly linking cortisol elevation to impaired N3-dependent brain waste clearance. While this evidence is primarily from rodent studies and should be interpreted cautiously in human contexts, it provides a plausible mechanistic pathway connecting chronic stress to the neurodegenerative risk associated with poor sleep quality.
There is also emerging rodent-model evidence that the quality of N3 micro-architecture — not just its duration — determines glymphatic clearance efficiency. Infraslow oscillations in norepinephrine, cerebral blood volume, and cerebrospinal fluid are phase-locked during NREM sleep and appear to drive the slow vasomotion that pumps CSF through brain tissue. Interestingly, the frequency of micro-arousals during NREM correlated more strongly with glymphatic clearance than total NREM duration or EEG delta power in this animal model — suggesting that fragmented N3, even when present by duration, may be functionally insufficient. These findings are from rodent studies and require replication in humans before clinical conclusions can be drawn.
Cortisol also antagonizes melatonin signaling, disrupting the circadian timing of sleep onset and further compressing the early-night SWS window. The result of chronic stress is a distinct architectural pattern: suppressed SWS depth early in the night, with relatively preserved but fragmented REM — a profile different from both insomnia's hyperarousal signature and apnea's arousal-mediated interruption.
Why When You Sleep Matters: The Timing Asymmetry of Stage Loss
Sleep stages are not distributed evenly across the night. N3 slow-wave sleep dominates the first half — the deepest SWS cycles typically occur in the first one to two cycles after sleep onset. REM dominates the second half — the longest REM periods, sometimes lasting close to an hour, occur in the final cycles before waking.
This asymmetry means that the timing of sleep truncation determines which stage bears the disproportionate cost. Cutting sleep short in the first half of the night — whether by a late bedtime, early waking, or a disruptor that specifically attacks early-night sleep — disproportionately reduces SWS. Cutting it short in the second half — early alarm, early morning waking, or a disruptor that attacks late-night sleep — disproportionately reduces REM.
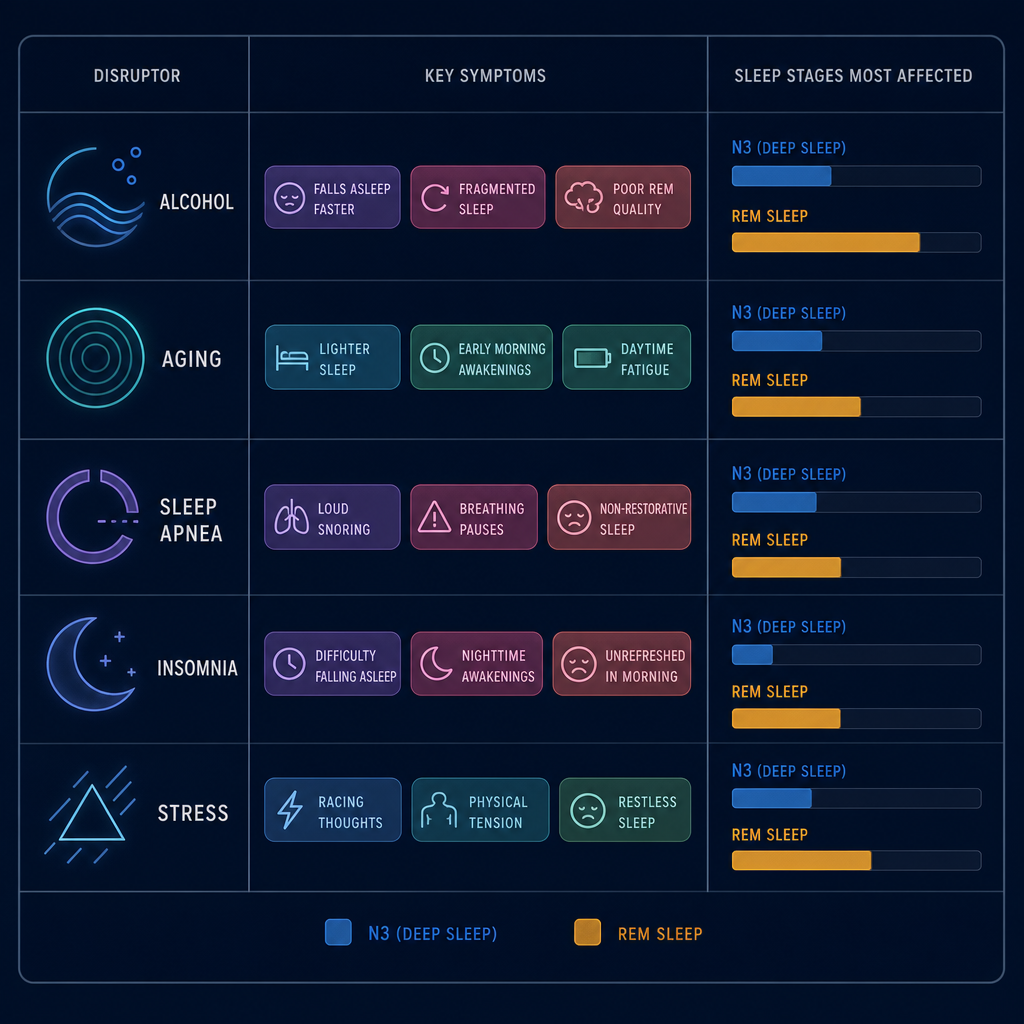
Mapping Your Symptoms to the Most Likely Disruptor
Each disruptor produces a recognizable symptom pattern. The table below maps common presentations to the most probable mechanism, the stage most affected, and the recommended next step. This is a triage framework, not a diagnostic tool — but it can help you identify which conversation to have first.
| Symptom Pattern | Most Likely Disruptor | Stage Most Affected | Recommended Next Step |
|---|---|---|---|
| Sleep feels adequate but you wake groggy; symptoms worse on nights after drinking; second half of the night is restless | Alcohol (two-phase disruption) | REM (first-half suppression); N2/N1 (second-half fragmentation) | Eliminate alcohol within 3–4 hours of bedtime; reassess after 2 weeks |
| Sleep has progressively lightened over years; more nighttime awakenings; feel less refreshed than you did a decade ago | Aging (progressive SWS decline) | N3 slow-wave sleep | Rule out apnea and insomnia as contributors; discuss sleep quality (not just duration) with a clinician |
| Partner reports snoring or breathing pauses; excessive daytime sleepiness despite adequate time in bed; waking with headaches | Obstructive sleep apnea | N3 and REM (arousal-mediated interruption) | Seek formal sleep study (polysomnography or home sleep test); CPAP evaluation if diagnosed |
| Racing mind at bedtime and during the night; sleep tracker shows low deep sleep; sleep worsens during stress periods; pattern has persisted for months | Chronic insomnia (hyperarousal model) | N3 (reduced depth and stability); NREM quality broadly | CBT-I is the evidence-based first-line treatment — see our CBT-I FAQ for how to access it |
| Sleep became unrestorative during a high-stress period; SWS feels shallow; emotionally reactive or cognitively foggy after adequate duration | Stress / HPA axis cortisol elevation | N3 (cortisol-mediated SWS suppression) | For mild to moderate stress profiles not yet requiring clinical referral, structured wind-down practices can reduce cortisol before sleep onset |
A few clarifications on using this framework:
- Disruptors stack. Aging plus untreated apnea is extremely common in adults over 50. Chronic insomnia and stress-related SWS suppression overlap substantially and often require the same first-line intervention.
- Consumer wearable sleep stage data has real limitations — four-stage classification accuracy averages around 65% across devices compared to polysomnography. A low deep-sleep score on your tracker is a signal worth investigating, not a diagnosis.
- If your symptom pattern maps to sleep apnea, pursue formal evaluation regardless of other factors. Apnea is underdiagnosed, especially in women, and CPAP treatment has the most dramatic architectural recovery of any intervention on this list.
- If your pattern maps to chronic insomnia, CBT-I is the first-line treatment — not supplements, not sleep restriction alone, and not waiting for the stress to pass.
Supports these guides
Spot an error or have clinical feedback?
Because this article covers clinical, medication, or safety information, we use a moderated correction channel instead of open public comments. Let us know if something about “How Five Common Disruptors Destroy Your Sleep Architecture — And What Each One Costs” needs a closer look.
Send feedback on this article