“I can’t sleep” sounds like one complaint until you ask where sleep is breaking down. For one person, the problem is the first two hours in bed. For another, sleep starts fine and then falls apart at 3 a.m. For someone else, the wake-up comes before dawn and feels final, as if the night has been cut off early.
Those are different problems. They can overlap, and they can change over time, but they point to different first moves. Before adding another supplement, app, tea, or relaxation exercise, the more useful question is: when does sleep fail?

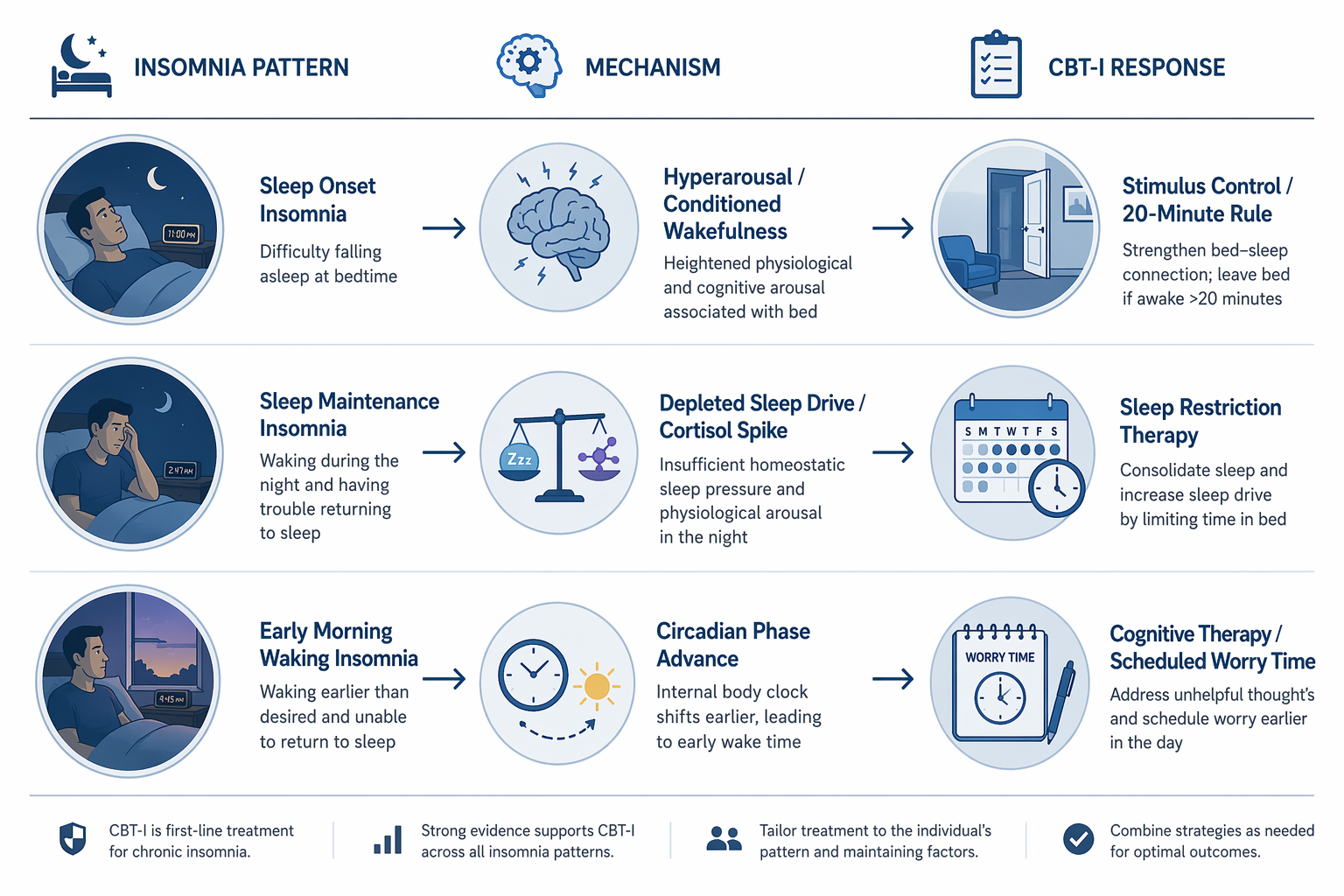
| If your main problem is... | The pattern may be... | The first CBT-I lever to understand |
|---|---|---|
| You get into bed tired but become alert, restless, or mentally busy | Sleep onset insomnia | Stimulus control and the 20-minute rule |
| You fall asleep, then wake for long stretches during the night | Sleep maintenance insomnia | Sleep restriction therapy and sleep drive |
| You wake much earlier than intended and cannot return to sleep | Early morning awakening | Circadian timing, mood screening, cognitive tools, and clinical escalation when needed |
Population data support treating these as separate patterns rather than one blurred insomnia bucket. In a CDC/NCHS analysis of U.S. adults in 2020, 14.5% reported trouble falling asleep and 17.8% reported trouble staying asleep; trouble falling asleep was highest among adults ages 18–44 at 15.5%, while trouble staying asleep was highest among adults ages 45–64 at 21.8%.[1] Those figures do not diagnose any individual reader, and the 2020 timing matters, but they do show that “can’t sleep” does not describe a single population.
Pattern 1: You Cannot Fall Asleep
Sleep onset insomnia usually has a recognizable texture. You may feel sleepy on the couch, then become sharply awake once you get into bed. Your body is still, but your attention is not. You calculate how much sleep is left, replay the day, plan tomorrow, monitor whether you are relaxing correctly, and notice every sign that sleep has not arrived.
The mechanism is often less mysterious than it feels. Bed has become associated with effort, waiting, checking, and frustration. That is conditioned wakefulness: the bedroom cues that should signal sleep start signaling performance pressure. Hyperarousal does not always feel like panic. Sometimes it feels like a quiet, stubborn alertness that appears only when you are trying to sleep.
This is why the first behavioral lever is usually stimulus control, not a longer list of bedtime rituals. In cognitive behavioral therapy for insomnia, stimulus control is used to rebuild the bed-sleep association, and the commonly taught 20-minute rule is part of that logic: if you cannot sleep after roughly 20 minutes, get out of bed, do something quiet and low-stimulation, and return when sleepy.[2]
The point is not to punish yourself for being awake. It is to stop giving your brain two more hours of practice being awake in bed. For sleep onset insomnia, that distinction matters. More time in bed can feel like the responsible choice, but if most of that time is spent alert and frustrated, it can train the wrong association.
Relaxation exercises can still be useful, especially when physical tension is high. But if the core pattern is conditioned wakefulness, relaxation alone may miss the part of the problem that happens through repetition: bed becomes the place where wakefulness keeps getting rehearsed.
Pattern 2: You Fall Asleep, Then Wake Up for Long Stretches
Sleep maintenance insomnia is different. You may fall asleep quickly enough, sometimes with relief, then wake in the middle of the night and remain awake. The clock time varies, but many people describe the same aggravating rhythm: sleep begins, breaks, and will not restart. If this sounds like your pattern, a deeper look at waking up at 3 a.m. every night may be more useful than another general bedtime checklist.
One behavioral mechanism here is weakened sleep drive. Sleep drive builds during wakefulness and is discharged during sleep. If you spend too much time in bed relative to how much sleep your body is currently producing, sleep can become lighter and more fragmented. The result is not always trouble starting the night. It can be wakefulness after sleep onset.
CBT-I often addresses this with sleep restriction therapy, a structured method that temporarily limits time in bed to consolidate sleep, then gradually expands the sleep window as efficiency improves. The CBT-I primer by Walker and colleagues describes sleep restriction therapy as especially relevant for wake after sleep onset, while stimulus control is more directly aimed at sleep onset problems.[2] For readers who want the mechanism in more detail, sleep maintenance insomnia as a sleep drive problem is the right next layer.
This is also where the well-meant advice to nap can backfire. A nap may feel like survival after a bad night, but for some people it reduces the pressure needed to keep the next night consolidated. That does not mean naps are always wrong; it means they have to be judged against the pattern. If your nights are broken because sleep drive is too diluted, whether to nap when you have insomnia is not a side question.
There is an important caution here. Middle-of-the-night waking is not automatically behavioral insomnia. Sleep apnea, nocturia, chronic pain, medication effects, hot flashes, reflux, alcohol use, and other medical or physiological causes can fragment sleep. This matters especially when awakenings come with gasping, snoring, frequent urination, pain, palpitations, or daytime sleepiness that feels disproportionate to the hours slept. In that situation, the first move is not to force a stricter sleep schedule; it is to consider medical evaluation.
When a clinician or qualified CBT-I program does use sleep restriction, it should be structured, not improvised aggressively. The method can be powerful because it works with homeostatic pressure, but cutting sleep opportunity too sharply can worsen daytime functioning. A safer next read is how sleep restriction therapy actually works, especially before trying to design your own schedule.
Pattern 3: You Wake Too Early and the Night Feels Over
Early morning awakening is not just “waking in the night” with a different clock time. The feeling is often distinct: you wake before your intended time, sometimes before dawn, and returning to sleep seems unavailable. You may not feel fully rested, but the body acts as if the sleep episode has ended.
One possible mechanism is circadian phase advance, where the body’s sleep-wake timing has shifted earlier. In that case, sleepiness may arrive earlier in the evening, and the final awakening may also arrive earlier than wanted. Readers who want the timing science behind this can go deeper into circadian rhythm mechanisms.
Early morning awakening also deserves a more explicit mood check than the other two patterns. Insomnia can be associated with mental health conditions, including depression, and waking too early is often treated clinically as a symptom worth asking about rather than brushing aside.[3] That does not mean one early wake-up diagnoses depression. It means repeated early final awakenings, especially with low mood, loss of interest, appetite changes, hopelessness, or thoughts of self-harm, should not be handled as a sleep-hygiene problem.
For this pattern, the first behavioral response depends on what else is present. If the early waking is paired with rumination, cognitive therapy skills and scheduled worry time may help move problem-solving out of the bed and out of the early morning hours. In a 2026 NPR discussion, sleep clinicians described scheduled worry time as a way to give anxious problem-solving a daytime container rather than letting it colonize the night.[4]
If early waking is persistent, worsening, or mood-linked, escalation should be earlier rather than later. The relevant question is not whether you are “bad at sleeping.” It is whether the early awakening is part of a circadian shift, a mood disorder, medication effect, medical condition, or chronic insomnia pattern that deserves targeted care. For more on the bidirectional relationship, see how depression and insomnia fuel each other.
Why the Problem Can Continue After the Original Trigger Is Gone
Many insomnia stories begin with a clear trigger: work stress, illness, grief, travel, caregiving, a new medication, a noisy apartment, a painful injury. The confusing part comes later, when the trigger improves but sleep does not.
The 3P model of insomnia helps explain that shift. It separates predisposing factors, precipitating factors, and perpetuating factors. The perpetuating factors are the ones people often adopt in desperation: spending extra time in bed, sleeping in, napping, canceling activity, monitoring sleep, and worrying about the next bad night. Walker and colleagues cite this model in their CBT-I primer to explain why insomnia can become self-sustaining after the original stressor fades.[2]
This is not a blame model. Most perpetuating behaviors are attempts to cope. If you slept three hours, of course you want to stay in bed longer. If you have a demanding day, of course you want to nap. If tomorrow matters, of course your brain starts calculating the consequences. The problem is that sleep can respond badly to the very strategies that feel most reasonable in the moment.
That is why CBT-I is usually more relevant than another generic sleep-hygiene pass. The CBT-I primer reports large treatment effects, with effect sizes of 1.0–1.2, and about a 50% post-treatment reduction in insomnia symptoms maintained for up to 24 months.[2] Those figures do not mean every person responds the same way, and they do not replace medical evaluation when symptoms suggest another disorder. They do explain why the behavioral component matched to your pattern deserves attention before the supplement aisle does.
How to Choose the First Move
If you are trying to sort this out on your own, do not start by rating your sleep as good or bad. Track the failure point for one to two weeks: bedtime, approximate sleep onset, awakenings, final wake time, out-of-bed time, naps, alcohol, major stressors, and daytime impairment. The pattern is often clearer on paper than it is at 4 a.m.
- If most of the awake time happens before sleep starts, focus first on stimulus control, the 20-minute rule, and reducing conditioned wakefulness in bed.
- If sleep starts but breaks into long awakenings, look first at sleep drive, time in bed, naps, and whether medical causes of fragmentation need to be ruled out.
- If the main problem is waking too early, look at circadian timing, morning and evening light patterns, mood symptoms, and whether the pattern warrants clinical evaluation.
- If rumination appears in any pattern, use cognitive tools such as scheduled worry time rather than trying to solve life from bed.
This is also the right order for considering sleep aids. A supplement may have a different rationale depending on whether the issue is sleep timing, sleep onset anxiety, or fragmented sleep. If you still want to compare options after identifying the pattern, use a pattern-based guide to choosing a sleep supplement for your specific sleep problem rather than treating every sleepless night as the same target.
For self-directed behavioral work, a broader companion resource on the behavioral home remedy for insomnia that outperforms pills can help translate CBT-I principles into a plan. The important part is not doing every sleep tip at once. It is choosing the component that matches where sleep is failing.
When “I Can’t Sleep” Needs More Than Self-Help
Chronic insomnia is commonly defined as sleep difficulty at least three nights per week for at least three months, with daytime impairment.[3] A 2024 American Academy of Sleep Medicine survey found that 12% of U.S. adults reported having been diagnosed with chronic insomnia.[5] Diagnosis is not the point of self-tracking, but duration and daytime consequences matter.
Seek evaluation sooner if sleep difficulty is paired with loud snoring or gasping, severe daytime sleepiness, chest symptoms, uncontrolled pain, frequent urination, new or changed medication, neurologic symptoms, pregnancy-related concerns, substance use concerns, or significant mood symptoms. Early morning awakening with hopelessness or thoughts of self-harm is urgent, not a sleep optimization project.
If the threshold is less urgent but the pattern is persistent, when trouble sleeping at night warrants a doctor’s visit is the next sorting step. Pattern recognition is useful because it makes that conversation more specific: not simply “I can’t sleep,” but “I take two hours to fall asleep,” “I wake for 90 minutes most nights,” or “I wake at 4:30 a.m. and cannot return to sleep.”
That specificity changes the next move. Sleep onset points toward conditioned wakefulness and stimulus control. Sleep maintenance points toward sleep drive, wake after sleep onset, and possible medical fragmentation. Early morning awakening points toward circadian timing, mood screening, and a lower threshold for help. “I can’t sleep” is the starting sentence. The useful answer begins when you can say where sleep is failing.
References
- Sleep Difficulties in Adults: United States, 2020, CDC/NCHS Data Brief 436, June 2022
- Cognitive Behavioral Therapy for Insomnia (CBT-I): A Primer, PMC
- Insomnia, Cleveland Clinic
- To beat anxiety and insomnia, schedule a time to worry, NPR, January 15, 2026
- Survey shows 12% of Americans have been diagnosed with chronic insomnia, American Academy of Sleep Medicine






Comments
Join the discussion with an anonymous comment.