You get into bed tired enough to believe tonight might be different. Then the checking starts. Am I sleepy yet? Is my jaw tight? Why is my heart doing that? How many hours are left if I fall asleep right now? The bedroom is quiet, but your body behaves as if something has gone wrong. Within minutes, sleep has stopped feeling like a natural state and started feeling like a performance review you are failing in real time.

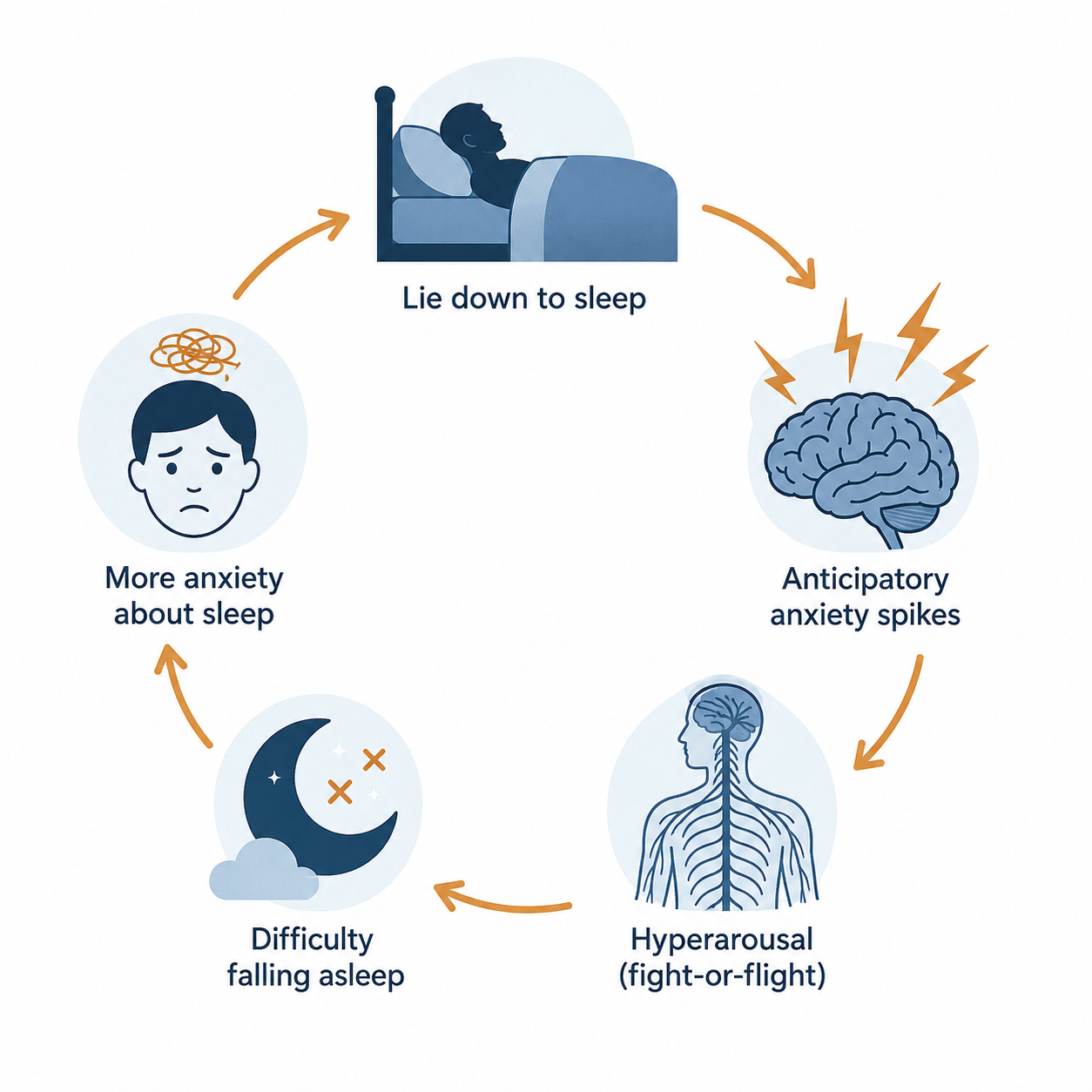
That spike of anxiety before bed is not proof that you are undisciplined, dramatic, or bad at relaxing. It often behaves like a learned alarm. After enough nights of worrying in bed, struggling in bed, clock-watching in bed, and dreading the next day in bed, the bed itself can become linked with wakefulness and threat. Cleveland Clinic describes sleep anxiety as fear or worry about going to sleep, staying asleep, or not getting enough sleep, and notes that anxiety can trigger physical arousal that makes sleep harder.[1] Sleep Foundation similarly describes nighttime anxiety as a cycle in which worry and physiological arousal interfere with falling asleep, which then gives the person more to worry about the next night.[2]
This is why treatment for sleep anxiety before bed has to aim at more than stress in general. The target is the bed-worry feedback loop. Cognitive behavioral therapy for insomnia, usually called CBT-I, is built for that loop.
When the bed becomes the cue for being awake
The loop is cruel because it uses your own effort against you. You lie down and scan for sleep. The scan finds anxiety. Anxiety raises arousal. Arousal delays sleep. The delay confirms that bedtime is dangerous. Tomorrow night, your nervous system remembers.
The experience is common enough that it deserves normalization, though not a pat on the head. In 2024, 15.4% of U.S. adults reported having trouble falling asleep most days or every day, according to a CDC/NCHS data brief published in 2026.[3] A 2024 online survey commissioned by the American Academy of Sleep Medicine found that 68% of U.S. adults reported losing sleep due to anxiety; that is self-reported sleep disruption from a survey of 2,006 adults, not a clinical diagnosis of insomnia.[4]
The useful conclusion is narrower and more hopeful than “many people are stressed.” If your anxiety reliably rises after you get into bed, the treatment has to teach your brain a new association: bed means sleep, not monitoring, bargaining, problem-solving, or panic rehearsal.
Why CBT-I is the first-line treatment, not a nicer bedtime routine
Mayo Clinic describes CBT-I as generally the first treatment recommended for people with insomnia and notes that it can be as effective as, or more effective than, sleep medicines for many people.[5] Sleep Foundation also presents CBT-I as a structured treatment that changes thoughts and behaviors that interfere with sleep, commonly including stimulus control, sleep restriction, cognitive restructuring, relaxation training, and sleep hygiene.[6]
That hierarchy matters. Lavender, herbal tea, a weighted blanket, and a gentle wind-down playlist may make the evening more humane. There is nothing wrong with humane. But if the bed has become the place where your body practices alarm, pleasant rituals alone may not reach the conditioned association that keeps firing when the lights go out.
CBT-I is not one trick. It is a sequence. Some parts reduce the amount of time you spend awake in bed. Some build enough sleep drive that sleep becomes more likely. Some challenge catastrophic predictions about tomorrow. Relaxation has a place, but it is not asked to carry the entire treatment.
| CBT-I component | What it changes in bedtime anxiety |
|---|---|
| Stimulus control | Stops the bed from being a place where you repeatedly practice anxious wakefulness |
| Sleep restriction | Matches time in bed more closely to actual sleep so sleep drive becomes stronger |
| Cognitive restructuring | Interrupts catastrophic thoughts that turn wakefulness into emergency |
| Relaxation training | Lowers physical arousal without making calmness another test |
| Sleep hygiene | Removes obvious barriers, but does not replace the behavioral treatment |
Stimulus control: stop rehearsing fear in bed
Stimulus control is the CBT-I instruction that sounds almost rude when someone first hears it: use the bed only for sleep and sex, and if you are awake for about 20 minutes, get out of bed, go somewhere dim and quiet, and return only when sleepy. Mayo Clinic includes this kind of instruction in CBT-I, and Sleep Foundation describes stimulus control as a way to rebuild the bed as a cue for sleep rather than wakefulness.[5][6]
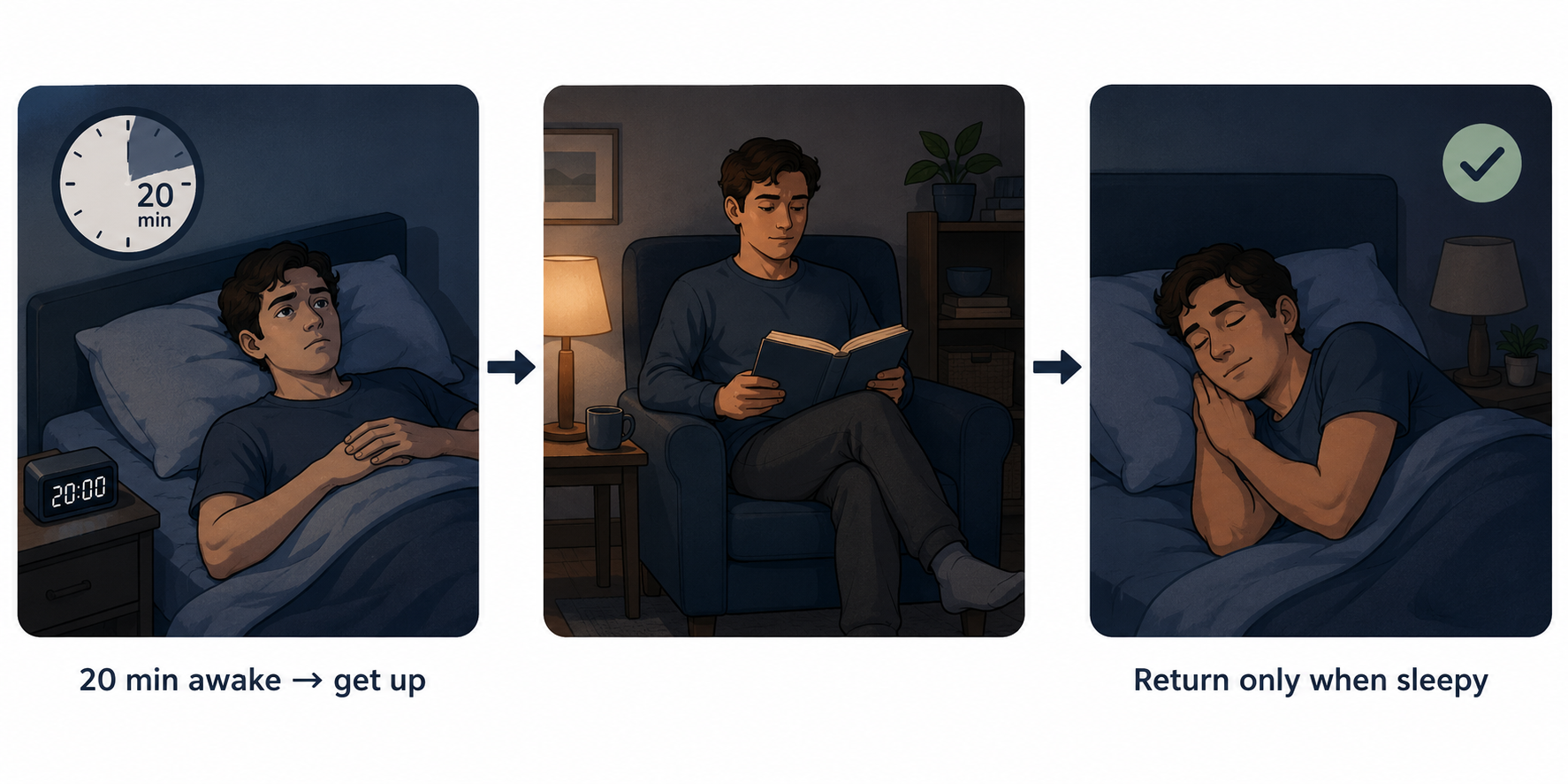
The 20-minute mark is not meant to turn you into a courtroom stenographer for your insomnia. Do not stare at the clock. The practical version is this: if you can tell you are awake, activated, and starting to wrestle with sleep, leave. The point is to interrupt the pairing of bed plus anxious wakefulness.
This is not punishment. It is retraining. Staying in bed for two anxious hours may feel like commitment, but your nervous system may be learning the wrong lesson: this mattress is where we fight. Getting up breaks the rehearsal. You move to a pre-chosen boring place with dim light. You do something quiet that does not reward wakefulness too much: a dull book, calm music without scrolling, a simple repetitive task. When real sleepiness returns, you go back.
The first few nights can feel inefficient. You may get up more than once. That does not mean you are doing it wrong. It means the old association is still strong, and you are refusing to strengthen it further.
Sleep restriction: the part people understandably resist
Sleep restriction is badly named for anxious sleepers because it sounds like deprivation for people who are already suffering. In CBT-I, the purpose is more specific: limit time in bed to better match the amount of time you are actually sleeping, then gradually expand the window as sleep becomes more consolidated. Mayo Clinic describes this as a CBT-I method that limits time spent in bed while awake, and a 2019 review in American Journal of Lifestyle Medicine describes sleep restriction as a way to increase sleep drive and consolidate sleep.[5][7]
A simplified hypothetical example: if someone spends 8 hours in bed but sleeps about 5.5 hours, a clinician might begin with a sleep window closer to 5.5 hours rather than allowing several extra hours of anxious wakefulness. As sleep efficiency improves, time in bed is increased gradually. In real care, this is individualized, and people with medical conditions, high safety risks, bipolar disorder, seizure disorders, or severe daytime sleepiness should not improvise aggressive sleep restriction on their own.
This is the part that can feel worse before it feels better. Daytime sleepiness can increase at first. The comfort of “at least I am resting in bed” is hard to give up, especially when you are scared of losing more sleep. But long, frustrated time in bed is exactly what teaches the brain that bed is an arena. Sleep restriction removes some of that arena time and builds stronger pressure for sleep when you do get into bed.
Cognitive restructuring: answer the alarm without arguing all night
Anxious thoughts at bedtime are rarely original, but they are persuasive at 1:17 a.m. CBT-I does not ask you to pretend they are cheerful. Cognitive restructuring asks you to treat them as predictions, not verdicts. Beck Institute Cares describes CBT strategies for nighttime anxiety that include identifying sleep-interfering thoughts and replacing them with more balanced responses.[8]
| Bedtime thought | More accurate response |
|---|---|
| I’ll never fall asleep. | I have fallen asleep many times before. Anxiety is loud right now, but it is temporary. |
| Tomorrow is ruined. | Tomorrow may be harder if I sleep poorly, but one bad night does not decide the whole day. |
| If I do not calm down now, I am making this worse. | Calm is not a performance. I can follow the plan even while anxious. |
The wording should sound like something you can actually believe. “Everything is fine” may be too far from the facts when your chest is tight and the clock is moving. A better response is often modest: “This is uncomfortable, and I know what step comes next.”
It also helps to move problem-solving earlier. Cleveland Clinic’s advice for a racing mind includes writing down worries or next-day tasks so they are not being processed for the first time in bed.[9] That is not magic; it is containment. You are giving the planning mind a scheduled place to work so the bed does not become its office.
Where relaxation fits
Relaxation training is useful when it is treated as a way to lower arousal, not as a moral requirement to become serene on command. Johns Hopkins Medicine lists techniques such as deep breathing, progressive muscle relaxation, and guided imagery as stress relief methods that can support sleep.[10]
For bedtime anxiety, the instruction should be deliberately low-pressure. Try slow breathing or progressive muscle relaxation for a short period. If it helps, good. If it does not, you have not failed relaxation. You move to stimulus control rather than lying there trying to manufacture calm while becoming more alert with every breath count.
Sleep hygiene belongs in the same supporting role. Caffeine timing, alcohol, light exposure, screens, room temperature, and irregular wake times can all matter. But for someone whose anxiety reliably ignites in bed, hygiene is the floor, not the treatment plan. A clean bedroom routine does not automatically undo conditioned arousal.
What the evidence can and cannot promise
CBT-I earns its reputation because it changes sleep behavior, not because it sounds soothing. The 2019 review in American Journal of Lifestyle Medicine describes CBT-I as producing results equivalent to sleep medication, with no medication side effects, fewer relapses, and sustained improvement after treatment.[7] Sleep Foundation summarizes that about 70% to 80% of people with primary insomnia experience improvement with CBT-I, though that broad figure comes from varied studies and should not be read as a guarantee for any one person.[6]
A meta-analysis reported clinically meaningful average changes: about a 19-minute reduction in time to fall asleep, about a 26-minute reduction in wake time after sleep onset, and about a 10% improvement in sleep efficiency.[7] Those numbers are not an overnight personality transplant. They are treatment effects measured across people, and they fit what CBT-I is trying to do: less time awake in bed, more consolidated sleep, and a weaker link between bedtime and alarm.
This is why generic advice can feel insulting even when it is kindly meant. The problem is not that you have never heard of relaxation. The problem is that your body has learned a sequence, and learned sequences usually need repeated corrective experience.
A realistic first-night protocol
Tonight does not need to become a full self-improvement project. The first goal is to stop feeding the bed-anxiety association.
- Before entering the bedroom, write down the main worry and one next action for tomorrow. If there is no action, write “not solvable at midnight.”
- Choose your stimulus-control spot in advance: a chair, couch, or quiet corner with dim light and something boring to read.
- Get into bed and use one brief downshift technique, such as slow breathing or progressive muscle relaxation. Keep it gentle, not heroic.
- If you are clearly awake and activated after roughly 20 minutes, leave the bed. Do not negotiate with the mattress.
- Return only when sleepy. If anxiety restarts, repeat the same rule.
One night of this may not feel like success. In fact, if you are used to staying in bed and fighting for sleep, getting up can feel like losing. Judge the night by whether you followed the retraining plan, not by whether sleep arrived on command.
When to get help, and what kind
If sleep trouble happens at least 3 nights a week for 3 months or longer, or if anxiety is severe, worsening, or interfering with daytime functioning, it is time to involve a clinician rather than keep inventing private rules in the dark. Cleveland Clinic and Mayo Clinic both distinguish persistent insomnia and sleep anxiety as treatable concerns, not character defects.[1][5]
Look specifically for CBT-I, not just general sleep tips. Treatment is often structured over several sessions; Cleveland Clinic notes CBT for insomnia may involve 6 to 8 sessions.[1] Digital CBT-I programs and tools may also help when in-person access is limited, and Sleep Foundation describes online CBT-I options as part of the treatment landscape.[6]
Medication may have a role for some people, especially short term and under medical guidance, but it is not the same as retraining the bed-sleep association. Mayo Clinic cautions that over-the-counter sleep aids containing antihistamines such as diphenhydramine or doxylamine can cause side effects including daytime drowsiness, and prescription sleep medicines have risks that should be discussed with a clinician.[5]
The point of CBT-I is not to become the kind of person who never feels anxious in bed. It is to stop making the bed the place where anxiety gets hours of practice. That is why the odd instructions matter: leave the bed when wakefulness takes over, narrow time in bed when sleep is badly fragmented, answer catastrophic thoughts without debating them until dawn, and use relaxation as support rather than proof that you deserve sleep.
References
- Sleep Anxiety: What It Is, Causes, Symptoms & Treatment — Cleveland Clinic
- Anxiety at Night: Causes and Tips for Relief — Sleep Foundation
- Short Sleep Duration and Sleep Difficulties Among Adults: United States, 2024 — CDC/NCHS Data Brief #559, Apr 2026
- Stress, anxiety, depression and sleep: New AASM survey results — AASM, 2025
- Insomnia treatment: Cognitive behavioral therapy instead of sleeping pills — Mayo Clinic
- Cognitive Behavioral Therapy for Insomnia (CBT-I): How It Works — Sleep Foundation
- CBT-I: An Effective and Underutilized Treatment for Insomnia — PMC / American Journal of Lifestyle Medicine, 2019
- Nighttime Anxiety and Insomnia: CBT Strategies for Better Sleep — Beck Institute Cares, 2025
- How To Stop Your Mind from Racing and Get To Sleep — Cleveland Clinic
- Sleepless Nights? Try Stress Relief Techniques — Johns Hopkins Medicine






Comments
Join the discussion with an anonymous comment.