A CPAP machine does one thing very well when it is tolerated and used correctly: it pushes pressurized air through the upper airway so the airway does not collapse during sleep. That is treatment. It is not the same as removing the reason the airway was prone to collapse in the first place.
That distinction is the medical center of the current debate over veterans benefits and sleep apnea. A mask, hose, humidifier, filters, pressure setting, and nightly cleaning routine are not evidence that obstructive sleep apnea has disappeared. They are evidence that the veteran is using an external device to keep a chronic sleep-related breathing disorder controlled for the hours the device is on.

What CPAP Actually Does
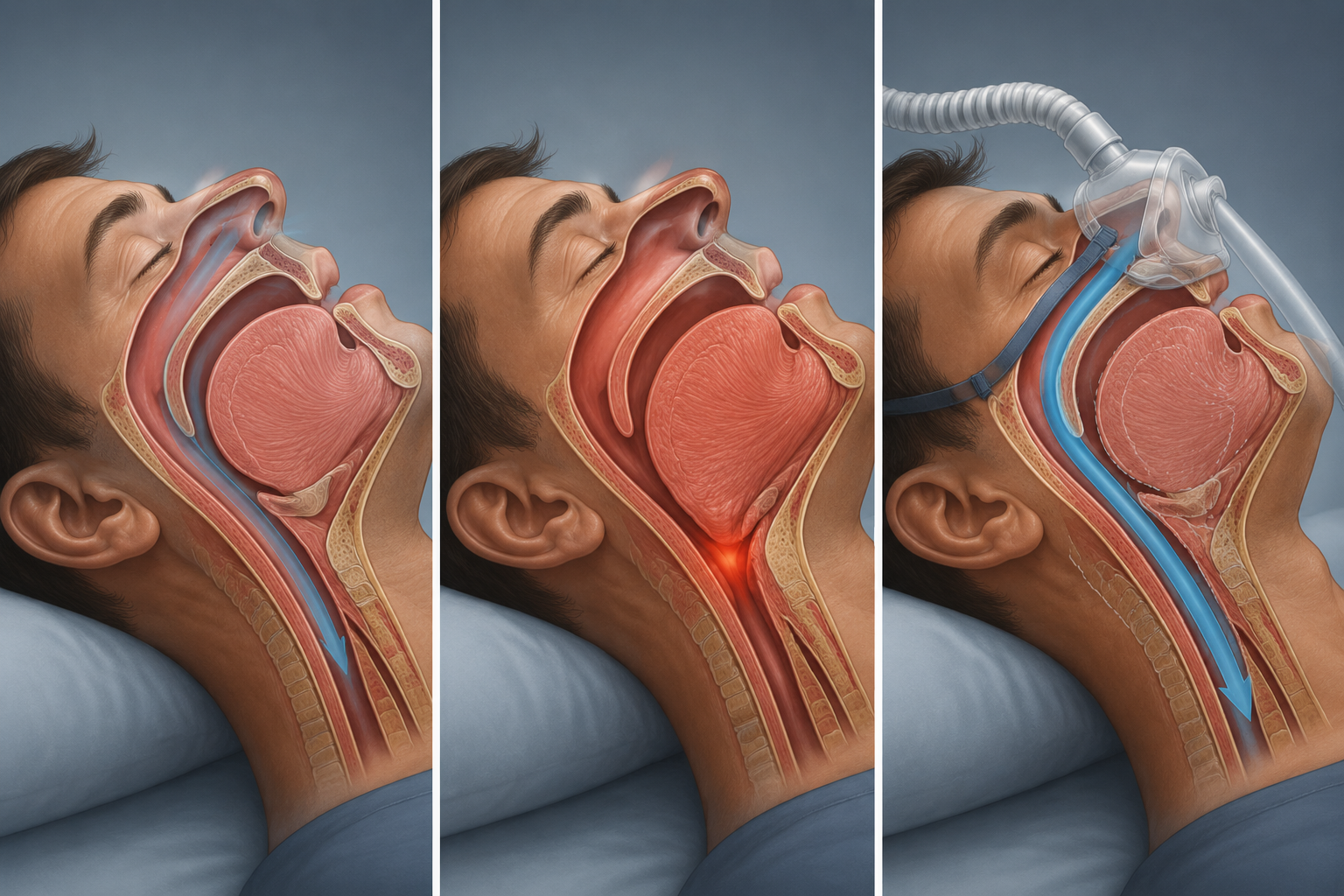
Obstructive sleep apnea is not simply “snoring with a machine.” During sleep, the muscles that help keep the throat open relax. In people with a vulnerable airway, that relaxation can let the soft tissues of the upper airway narrow or collapse. The result is repeated partial or complete obstruction, drops in airflow, oxygen stress, arousals from sleep, and the familiar cycle of fragmented rest followed by daytime impairment.
CPAP, or continuous positive airway pressure, works like a pneumatic splint. It does not cut away tissue, change jaw structure, enlarge the airway, or permanently retrain the pharyngeal muscles. It supplies enough pressure to hold the airway open while the person sleeps with the mask on. Take the pressure away, and the anatomical or neuromuscular tendency toward collapse can still be there.
That matters because disability logic often turns on the difference between a condition that has resolved and a condition that is controlled only by ongoing treatment. A veteran who sleeps because a device is forcing the airway open has not become physiologically identical to someone who never had obstructive sleep apnea. The disease process is being managed in real time.
The Mask Can Normalize Airflow Without Normalizing the Whole Night
For many patients, CPAP is highly effective. It can reduce obstructive events, improve oxygenation during use, and help people wake less exhausted. That effectiveness is exactly why clinicians prescribe it. But effectiveness during use is not a cure, and it is not always a complete restoration of normal sleep.
Some users still wake with dry mouth from mask leak or mouth breathing. Some take the mask off during the night without fully waking. Some sleep longer but still feel unrefreshed. Some continue to report residual daytime sleepiness, attention problems, or cognitive fog even when the device data look acceptable. These are not all the same clinical picture, and they should not be treated as if every compliant CPAP user has identical remaining impairment. The point is narrower and more important: use of the device does not prove absence of disease.
Sleep architecture is one reason. Obstructive events do not only interrupt breathing; they can fragment the structure of sleep. A machine that prevents collapse may reduce the immediate respiratory trigger, but it does not automatically erase years of poor sleep, reverse every downstream effect, or guarantee that a veteran’s sleep becomes normal in duration, continuity, and restorative value.
Why Veterans Are Not a Small Edge Case
The rating question has become so tense partly because obstructive sleep apnea is common among veterans. A 2024 Sleep Health study reported diagnosed obstructive sleep apnea in 21% of veterans, with a 20% to 22% confidence interval, compared with 9% of nonveterans, with an 8% to 10% confidence interval. The authors described veterans as about 2.5 times more likely to have diagnosed OSA than nonveterans.[1]
That prevalence figure does not prove that military service caused every individual case. It does show why a rating change would not be a niche administrative adjustment. It would land in a population where sleep-disordered breathing is already diagnosed at a much higher rate than among nonveterans.
The financial scale is also large. DAV has projected that the proposed changes could reduce compensation by $57 billion over 10 years and affect up to 1.5 million veterans.[2] That projection is an advocacy organization’s estimate, not an independent clinical finding, but it explains why veterans’ organizations are treating the issue as consequential.
PTSD Can Make “Just Use the CPAP” a Clinical Oversimplification
CPAP adherence matters. A machine sitting unused on a nightstand cannot splint the airway. But the assumption that CPAP is a simple, universally tolerable solution fits poorly with many veterans’ sleep realities, especially when PTSD symptoms are present.
A mask can feel confining. Pressurized air can intensify the sense of being trapped. Hyperarousal can make small leaks, hose movement, or pressure changes feel impossible to ignore. Nightmares and fragmented sleep can lead to repeated mask removal. None of this makes CPAP ineffective as a therapy; it makes the nightly act of using it more complicated than an administrative checkbox suggests.
That distinction is important because rating logic built around prescribed treatment can quietly assume a level of stable use that some veterans have to fight for every night. Compliance is not merely possession of equipment. It is repeated behavior under physiological, psychological, and practical constraints.
The Hypertension Analogy Is Not Perfect, but It Is Useful
The National Veterans Foundation has argued that rating sleep apnea at 0% because CPAP manages its most acute symptom is inconsistent with how VA treats other chronic conditions, including hypertension and diabetes, when medication or treatment controls measurable danger.[3]

The analogy works because nobody would say a veteran’s hypertension has been cured simply because medication lowers the blood pressure reading that day. The medication is doing the controlling. Stop the medication, and the underlying tendency may return. The disease remains chronic even when the risk is being actively managed.
CPAP fits that chronic-management pattern. The machine prevents airway collapse while it is used. It does not remove the vulnerable airway anatomy, the sleep-related muscle relaxation, or the predisposition to obstruction. In that sense, the medically relevant question is not whether CPAP can help. It clearly can. The question is whether a rating system should treat successful nightly management as near-absence of the condition.
There are differences between blood pressure medication and CPAP. Hypertension can be measured during a clinic visit; sleep apnea often has to be understood through overnight breathing events, device data, symptoms, and sleep quality. Medication is swallowed in seconds; CPAP requires hours of mask tolerance during sleep. Those differences make the comparison imperfect, but they do not weaken the central point. Ongoing treatment is not the same as cure.
Where the Proposed 0–10% Rating Runs Into the Physiology
The contested policy premise is that a veteran whose sleep apnea is controlled by CPAP may belong at a much lower disability rating, potentially in the 0% to 10% range, than under the older framework that gave substantial weight to the need for a breathing assistance device. The medical problem with that premise is not that CPAP is worthless. The problem is that CPAP’s value depends on proving the opposite: the airway still needs external pressure to stay open.
If a device is necessary every night to prevent repeated airway collapse, the need for the device is part of the disease burden. The machine does not merely document past illness. It participates in the veteran’s breathing during sleep. That is why the phrase “compliant with CPAP” should not be read as “medically normal.” It means the person is performing the treatment that keeps the condition controlled.
Residual risk is also a poor fit for a simple resolved-or-not-resolved framework. Obstructive sleep apnea is tied to oxygen stress, sleep fragmentation, cardiovascular strain, and cognitive symptoms. CPAP can reduce key harms when it is effective and used consistently, but the presence of treatment does not by itself answer whether the veteran still has daytime sleepiness, impaired concentration, blood pressure problems, or other consequences that matter in ordinary life.
The fairest version of the VA’s concern is that ratings should reflect actual impairment, not merely the fact that a device was prescribed years ago. That concern is legitimate. A system that ignores improvement would be medically blunt in the other direction. But a system that assumes controlled airway collapse is nearly equivalent to no airway disease at all is also blunt, and it is blunt in a way that conflicts with the mechanism of CPAP.
The Policy Status Is Still Moving
As of July 19, 2026, the policy picture should be treated as unsettled. VA messaging in June 2026 included two signals that are hard to reconcile cleanly: that no changes were planned or imminent, and that the rule would be finalized by October 1, 2026. Those statements leave veterans with uncertainty rather than a stable rule to interpret.
The legislative side is also fluid. The Take Care of America’s Veterans Act was pulled from the House floor on July 16, 2026, and Speaker Johnson indicated it could return in September 2026. That means the benefits debate is active, but it does not mean a final outcome can be stated with confidence.
Veterans service organizations are not speaking with one voice. The American Legion supports TCAVA, while DAV, VFW, and IAVA oppose it. That split should be read as a real policy disagreement among reputable organizations, not as proof that one side owns the medical truth.
The medical point is narrower than the politics around it. CPAP can be necessary and effective without being curative. Any benefits framework that treats compliant CPAP use as near-absence of sleep apnea needs to justify that assumption against the physiology of obstructive sleep apnea and against the way chronic managed conditions are treated elsewhere in disability logic.
References
- Diagnosed obstructive sleep apnea among veterans and nonveterans, Sleep Health, 2024
- DAV News 2026, DAV, 2026
- Veterans React to VA’s Proposed Sleep Apnea Rating Changes, National Veterans Foundation






Comments
Join the discussion with an anonymous comment.