You can be exhausted after an earthquake and still become wide awake the moment you lie down. That contradiction is often the part people find most frightening. Sleep pressure is there. The body wants recovery. But lying still, closing your eyes, and letting your guard drop can feel like the least safe thing to do.
This is where ordinary sleep advice after an earthquake often falls short. A dark room, a calmer routine, less news, and fewer screens may help during the first rough nights. They do not always touch the deeper problem: the bed has started to mean monitoring. Instead of “this is where I sleep,” the brain learns “this is where I might be trapped, miss the first seconds of warning, or fail to wake quickly enough.”

That reaction is not irrational. It is a safety system doing too much for too long. After a quake, the nervous system may keep checking for vibration, noise, shifting light, or the feeling of being boxed in. If that checking happens night after night in bed, the bed itself can become part of the alarm pattern.
Post-earthquake sleep disturbance is common enough that it should never be dismissed as a personal failure. In a study reported by the American Academy of Sleep Medicine after the 2010 Haiti earthquake, 94% of survivors reported insomnia symptoms, and 42% still had clinically significant PTSD two years later; the sample was modest and centered on Port-au-Prince, so it should not be treated as a universal earthquake statistic, but it does show how persistent sleep disruption can be for many survivors. [1]
When the Bed Becomes a Watch Post
In healthy sleep, the bed is boring in the best possible way. It becomes a cue for dropping effort. After a frightening earthquake, that cue can be overwritten. The room becomes a place to listen. The mattress becomes a place to detect movement. The first flutter of wakefulness becomes evidence that something may be wrong.
Clinically, this is close to conditioned hyperarousal. The body pairs a sleep setting with alertness, threat scanning, and escape planning. The pairing does not require a person to believe anything unreasonable. If the first quake or aftershock happened at night, or if the person felt trapped, disoriented, or responsible for helping others, the brain has a reason to treat sleep as a vulnerable state.
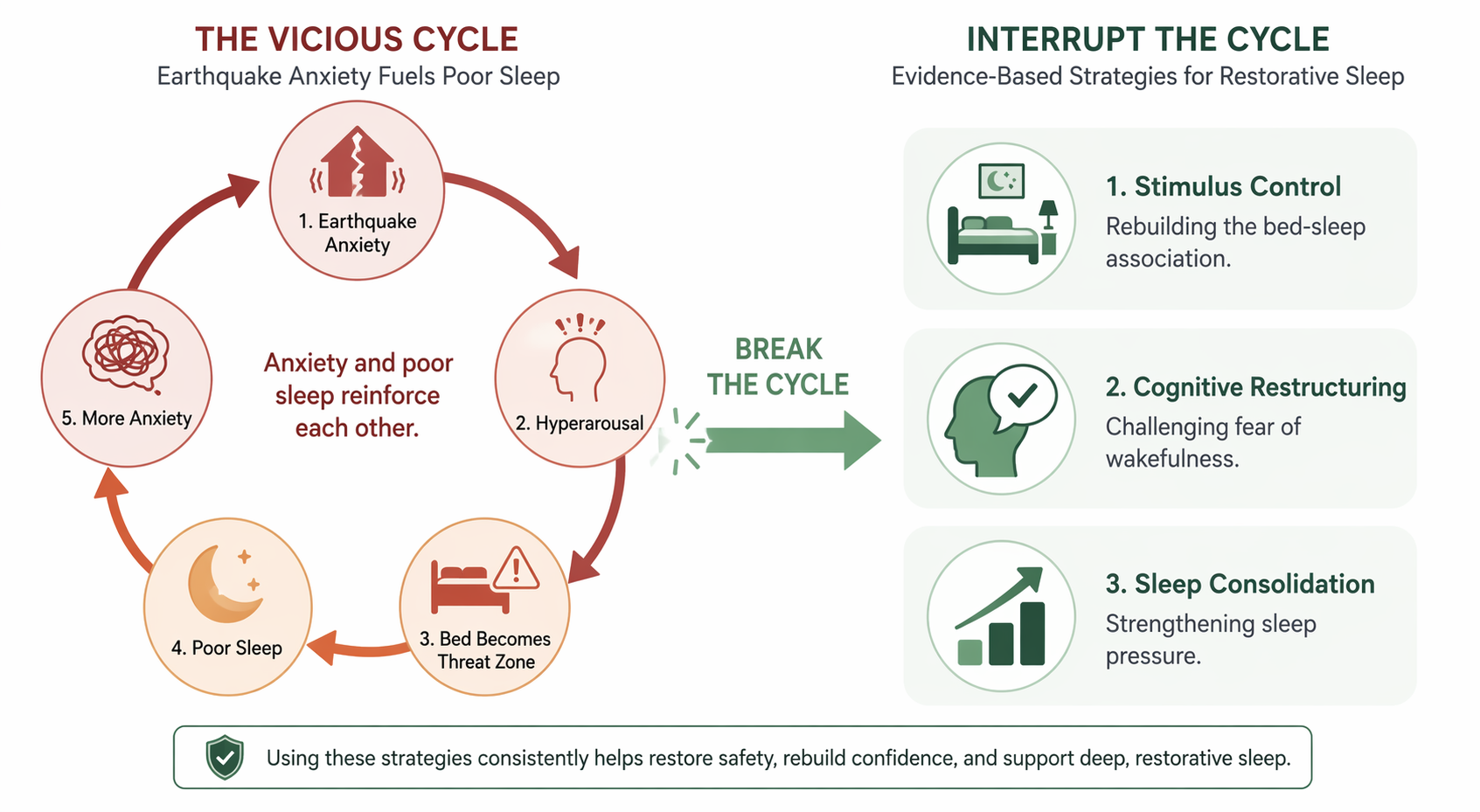
Adult earthquake research supports the same broad pattern, though not as a single clean proof of cause and effect. A 2025 study of 428 adult survivors in Turkey reported a mean Pittsburgh Sleep Quality Index score of 11.10 ± 3.44, consistent with poor sleep quality, and described a bidirectional relationship between sleep disruption and anxiety. The study used convenience sampling, and trauma exposure explained only a small portion of sleep-quality variance, so the careful conclusion is that earthquake-related distress and poor sleep appear to reinforce one another rather than that one exposure score fully explains insomnia. [2]
That loop matters more than the label. A bad night increases next-day shakiness, irritability, and threat sensitivity. More threat sensitivity makes bedtime feel more dangerous. Bedtime fear then fragments sleep again. A person can start by fearing aftershocks and end up fearing the act of being unable to sleep.
For readers who want the broader threat-system explanation before getting into treatment, How Earthquake and Bridge Collapse Fears Hijack Your Sleep goes deeper into the hyperarousal mechanism.
The Fear Is Often About Sleep Itself
One of the sharper findings comes from adolescent research after the 2023 Turkey earthquakes. In a 2025 study of adolescents assessed 9 to 12 months after the earthquakes, 89.4% of those with high earthquake anxiety had poor sleep, and high anxiety predicted 5.7 times worse sleep quality compared with mild anxiety; the authors specifically described fear of being trapped while asleep as a driver of reduced sleep duration. This was an adolescent sample, not adult evidence, so it should be read as an especially vivid illustration of the mechanism rather than as a direct estimate for adults. [3]
Still, the clinical theme is recognizable in adults: “If I sleep deeply, I won’t react fast enough.” “If I wake at 2 a.m., maybe my body knows something.” “If I get into bed, I’ll start listening again.” These thoughts are not random worry. They are interpretations of vulnerability.
This is also why reassurance can miss the mark. Telling someone “you’re safe now” may be factually reasonable and emotionally useless at 1:30 a.m. The conditioned brain is not asking for a lecture. It is running a prediction: bed plus darkness plus stillness equals reduced escape capacity. Treatment has to change the prediction through repeated experience.
Acute Stress Is Different From Persistent Insomnia
Not every bad sleep week after an earthquake needs formal insomnia treatment. In the immediate aftermath, sleep is often disrupted by practical danger, displacement, aftershocks, emergency alerts, injury, grief, or the simple fact that the body has been through something overwhelming. During that period, gentle stabilization can be enough: consistent wake time, daylight, food, movement, reduced late-night news checking, and a clear safety plan that does not have to be redesigned in bed.
If you are looking for that lighter layer of coping while things are still unsettled, Earthquake Anxiety Keeping You Awake? How to Finally Sleep is the more practical companion piece.
The threshold changes when the pattern lasts for weeks to months and begins to organize itself around the bed. That may look like taking hours to fall asleep because you are listening for movement, waking repeatedly to scan the room, avoiding bed until extreme exhaustion, sleeping better on a couch because the bedroom feels too loaded, or becoming frightened of wakefulness itself. At that point, the problem is no longer just “stress before bed.” It is learned insomnia.
It can help to name the pattern before choosing a treatment target. Sleep-onset insomnia, sleep-maintenance insomnia, and early-morning waking respond to overlapping CBT-I tools, but the emphasis can differ. Not Being Able to Sleep? Identify Your Insomnia Pattern can help sort out which version is dominating.
Why Sleep Hygiene Alone Often Cannot Undo This
Sleep hygiene is not foolish. A cooler room, a predictable wind-down, less caffeine, and fewer late-night alerts can remove friction from sleep. Those changes are useful when the sleep system is basically intact but irritated.
Conditioned insomnia is different. A person may follow every reasonable sleep-hygiene rule and still become more alert at bedtime because the strongest cue in the room is not light, temperature, or phone use. It is the learned meaning of the bed.
This distinction matters because it protects people from shame. If you are lying there tense despite doing “everything right,” the missing ingredient may not be discipline. It may be a treatment that directly retrains the bed-sleep association and the fear attached to wakefulness.
How CBT-I Matches the Mechanism
Cognitive behavioral therapy for insomnia, or CBT-I, is not simply advice to relax. It is a structured insomnia treatment that changes the behaviors and interpretations that keep wakefulness paired with the bed. The evidence base is strongest for general insomnia, not for a dedicated randomized trial limited to earthquake survivors. So the honest claim is narrower: CBT-I principles are well supported for insomnia and clinically fit the post-earthquake conditioned-arousal pattern.
A 2019 meta-analysis in the American Journal of Lifestyle Medicine reported that CBT-I reduced sleep latency by an average of 19 minutes, reduced wake after sleep onset by 26 minutes, improved sleep efficiency by 10%, and showed continued improvement after treatment ended. [4]
Those averages are not a promise for any one survivor. They are useful because they show that CBT-I can improve the parts of sleep that conditioned arousal tends to damage: getting into sleep, staying asleep, and spending less time awake in bed. For readers who want the general framework before applying it to earthquake fear, CBT-I for Sleep Anxiety covers the broader method.
Stimulus Control: Teaching the Bed to Mean Sleep Again
Stimulus control is often the most important CBT-I component when the bed has become a threat zone. The principle is simple and demanding: reserve the bed for sleep and intimacy, and stop using it as the place where the nervous system practices being awake.
For earthquake-related insomnia, this may mean getting out of bed when wakeful monitoring takes over, moving to a low-stimulation place, and returning only when sleepy again. The goal is not punishment. It is to stop giving the brain another hour of evidence that bed means listening, calculating, bracing, and checking.
This can feel counterintuitive to someone who is already exhausted. Many people think, “If I leave the bed, I’ll lose my chance to sleep.” But when the bed has become a rehearsal space for danger, staying there wide awake can strengthen the very association that is keeping sleep away.
A practical version is not dramatic. If you notice you are alert, scanning, or mentally replaying escape routes, you leave the bed briefly. You keep lights low. You avoid news, structural checking, social feeds, and anything that turns the safety system back on. You return when sleepiness, not defeat, is pulling you back. Over time, the bed gets fewer repetitions as a watch post and more repetitions as a sleep cue.
Cognitive Restructuring: Working With the Fear of Wakefulness
The cognitive part of CBT-I is sometimes misunderstood as “think positive.” That is too thin for earthquake insomnia. The useful work is more precise: identify the thoughts that make wakefulness feel dangerous, then test whether they are accurate, complete, and helpful at 2 a.m.
Common post-earthquake sleep thoughts include:
- “If I sleep deeply, I won’t wake up fast enough.”
- “If I’m awake, it means my body is warning me.”
- “If I don’t sleep tonight, I won’t be able to function or protect anyone tomorrow.”
- “The bedroom is unsafe because that is where I felt helpless.”
None of these should be mocked. They are attempts to reduce danger. The question is whether they are still serving the person now. A CBT-I clinician may help separate preparedness from nighttime rumination. Preparedness happens before bed: shoes accessible, flashlight placed, family plan reviewed once, alerts set appropriately. Rumination happens in bed and asks for one more scan, one more mental simulation, one more hour of partial vigilance.
A more balanced thought is not “nothing bad can happen.” It might be: “I have done the safety steps I can do tonight. Staying half-awake is harming tomorrow’s judgment. If an alert or strong movement happens, I will respond then.” That kind of statement does not erase uncertainty. It stops wakefulness from being treated as a moral duty.
For readers who want the deeper physiology behind why the body can feel so activated long after danger has passed, Neurobiology of Sleep Anxiety explains the HPA-axis, cortisol, and hyperarousal in more detail.
Sleep Consolidation: Reducing the Time Spent Awake in Bed
Sleep consolidation is the CBT-I element many people know as sleep restriction, though the clinical intention is not deprivation for its own sake. The aim is to reduce long, fragmented stretches in bed and build stronger sleep pressure across a more consistent sleep window.
For someone with earthquake anxiety, this matters because extra time in bed is often not neutral. It can become extra time for checking, anticipating aftershocks, and proving to the brain that the bedroom is where wakefulness happens. A carefully set sleep window can make sleep more compact, then gradually expand as efficiency improves.
This part should be handled carefully, especially for people with bipolar disorder, seizure disorders, significant medical illness, severe daytime sleepiness, safety-sensitive jobs, pregnancy, or complex trauma symptoms. Self-guided sleep restriction can be too blunt. A trained CBT-I provider can adjust the plan so it strengthens sleep pressure without creating unnecessary risk.
What Progress Usually Looks Like
CBT-I progress is often behavioral before it feels emotional. The first changes may be less time spent awake in bed, fewer long monitoring sessions, a more stable wake time, or a clearer boundary between daytime safety planning and nighttime rumination. The room may not feel peaceful right away. It may simply become less useful as a place to rehearse danger.
That distinction helps set expectations. The goal is not to force the body into calm on command. The goal is to give the sleep system repeated evidence that lying down does not require surveillance. Calm often follows that learning; it is not always the first step.
Medication can sometimes have a short-term role, especially when acute distress is severe or sleep loss is becoming unsafe, but it does not by itself retrain the bed-sleep association. The meta-analytic CBT-I findings are important partly because improvement can continue after treatment ends, which is what one would hope for when the target is learned insomnia rather than only nightly sedation. [4]
When to Get Professional Help
Professional care is appropriate if insomnia has lasted several weeks, is worsening, or is causing unsafe daytime sleepiness, panic at bedtime, heavy alcohol or sedative use, or inability to work, drive, parent, study, or recover physically. It is especially important if sleep problems come with nightmares, flashbacks, avoidance, persistent startle responses, depression, thoughts of self-harm, or a sense that life is no longer safe even outside the bedroom.
A clinician can also check for conditions that masquerade as insomnia or make it harder to treat: sleep apnea, restless legs syndrome, circadian rhythm disruption, medication effects, pain, thyroid problems, substance use, major depression, PTSD, or another anxiety disorder. CBT-I can still be useful in many of these situations, but the plan may need to be coordinated with trauma-focused therapy, medical care, or medication support.
If the bed has learned danger, recovery is not just calming down before bed. It is the repeated, deliberate process of teaching the brain that the bed is no longer the place where it has to keep watch.
References
- Disturbed sleep linked to mental health problems among earthquake survivors, American Academy of Sleep Medicine, 2019.
- Evaluation of sleep quality and anxiety among adult earthquake survivors, PMC, 2025.
- Earthquake anxiety and sleep quality among adolescents after the 2023 Turkey earthquakes, Scientific Reports, July 2025.
- Cognitive Behavioral Therapy for Insomnia: A Meta-Analysis of Long-Term Effects in Controlled Studies, American Journal of Lifestyle Medicine, 2019.






Comments
Join the discussion with an anonymous comment.