If you are using CPAP and have heard that Zepbound can treat sleep apnea, the most useful answer is not “yes” or “no.” It is this: a GLP-1–based medication may reduce obstructive sleep apnea over time in the right patient, but it does not hold the airway open tonight. CPAP does.
That difference matters most for adults with moderate-to-severe obstructive sleep apnea, usually defined as an apnea-hypopnea index, or AHI, of 15 or higher. AHI counts breathing pauses and shallow-breathing events per hour of sleep. CPAP and related PAP devices push air through the airway to prevent collapse while the machine is being used. GLP-1 drugs work on a different problem: excess weight, metabolic inflammation, blood pressure, and related forces that can make the upper airway more collapsible.
So the better question for “GLP-1 sleep apnea vs CPAP” is not which one wins in the abstract. It is which job each treatment is being asked to do, how fast it can do it, and whether your sleep apnea is the kind likely to improve when weight and metabolic risk improve.

CPAP and GLP-1 drugs are solving different parts of the same problem
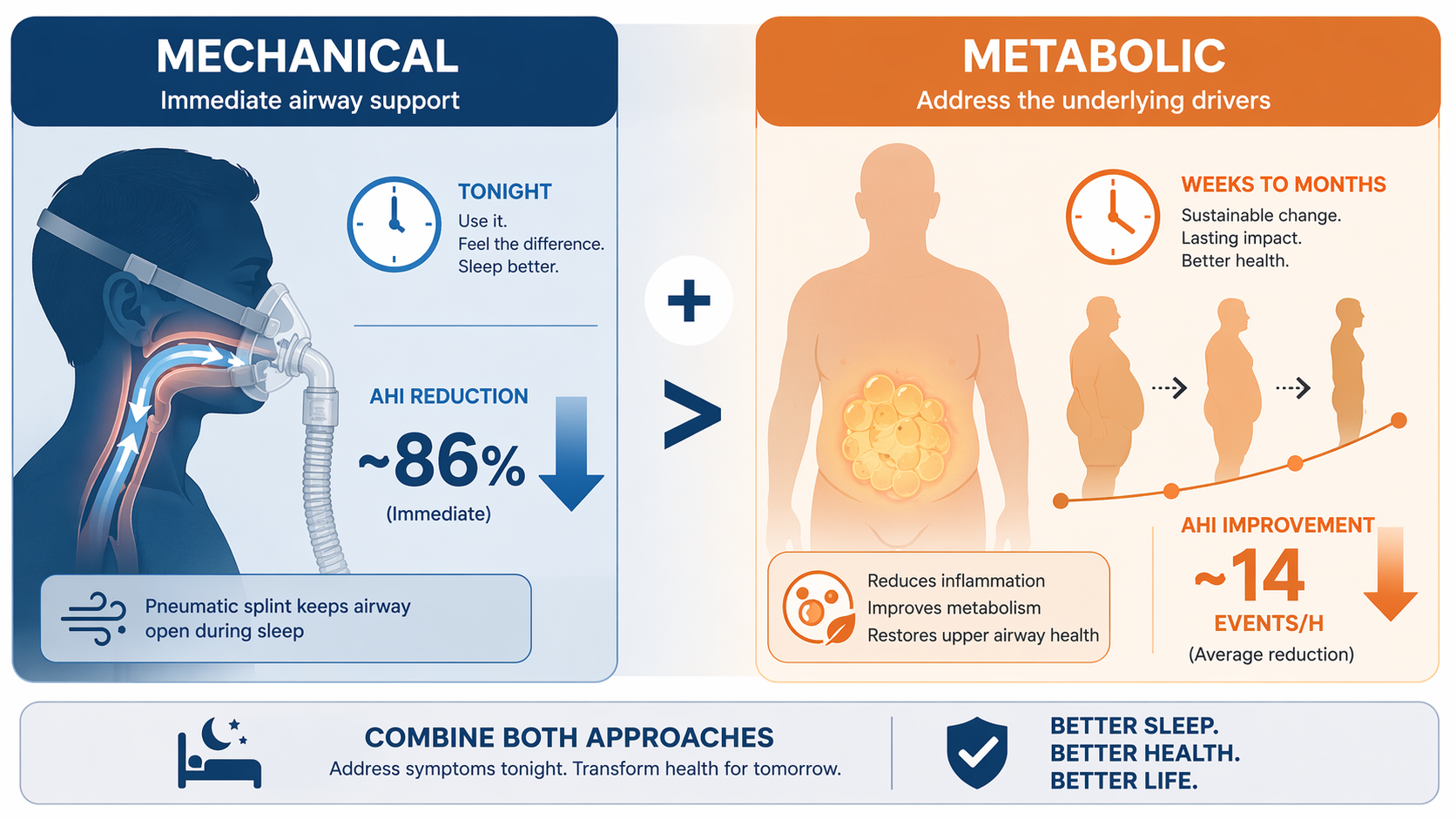
CPAP is not elegant. It is not subtle. It does not ask the airway to become healthier over the next several months. It simply creates enough positive pressure to keep the airway from repeatedly closing during sleep. That is why its AHI effect can appear so dramatic: clinical guideline data describe an average AHI reduction of about 86%, and a 2026 network meta-analysis estimated CPAP’s effect at a mean difference of −22.17 events per hour compared with no intervention.[1]
GLP-1 therapy is slower because it is working upstream. Weight loss can reduce fat deposition around the upper airway, improve lung volumes, and lower the mechanical load that promotes airway collapse. The broader metabolic effects may also matter: lower blood pressure, lower inflammatory markers, and improved cardiometabolic risk all sit close to the conditions that often travel with obesity-related OSA. But those changes accumulate over weeks to months, not over the first night.
That timing difference is where a lot of bad decisions can begin. A patient who hates CPAP may hear “sleep apnea drug” and understandably imagine putting the machine in a closet. A clinician hears the same phrase and worries that someone with uncontrolled moderate-to-severe OSA is about to stop the one treatment that prevents airway collapse while the medication is still titrating, still causing side effects, or still not producing enough weight loss to change AHI.
What the numbers actually show
The cleanest way to compare the evidence is to separate immediate airway control from metabolic disease modification. CPAP looks strongest when the outcome is AHI reduction during use. GLP-1 drugs look more interesting when the outcome includes body weight, blood pressure, HbA1c, and the possibility that obesity-related OSA becomes less severe over time.
| Treatment question | What the evidence supports | Decision meaning |
|---|---|---|
| What lowers AHI right away? | CPAP reduces AHI by about 86% on average and showed a mean difference of −22.17 events/hour versus no intervention in a 2026 network meta-analysis.[1] | Best fit for immediate airway protection while it is being used. |
| What does GLP-1 therapy do to AHI on average? | A 2026 meta-analysis of 4 randomized trials with 917 patients found a pooled AHI reduction of −13.89 events/hour, along with −12.46 kg body weight and −4.86 mmHg systolic blood pressure.[2] | Meaningful improvement, but not an overnight substitute for mechanical airway splinting. |
| Why are people excited about tirzepatide? | SURMOUNT-OSA studied 469 adults for 52 weeks and reported AHI reductions of about 25–29 events/hour with tirzepatide versus 5–6 with placebo; 42–50% reached AHI below 15 plus symptom resolution.[3] | Some eligible patients can move from severe disease toward a much less dangerous range, but over a year of treatment. |
| Is every GLP-1 drug equivalent for OSA? | In the network meta-analysis, tirzepatide showed a much larger AHI reduction than liraglutide: −23.80 versus −5.20 events/hour, with p < 0.0001.[1] | “GLP-1” is too broad a label for treatment expectations. |
Those numbers do not tell a simple replacement story. CPAP’s AHI effect is direct and conditional: it works while the device is being used. GLP-1 therapy’s AHI effect is partly mediated through weight loss and related metabolic change, so the same prescription can mean very different things depending on starting BMI, anatomy, medication response, dose tolerance, and whether treatment continues.
The SURMOUNT-OSA results deserve the attention they are getting. A 25–29 event/hour reduction is not a cosmetic change in a sleep study; for many patients, that is the difference between severe OSA and a category that may be easier to manage. But it was measured after 52 weeks, not after the first injection, and the trial excluded people with type 2 diabetes, which limits how confidently the findings can be carried over to the large share of OSA patients who also have diabetes.[3]
The pooled GLP-1 estimate from the 2026 meta-analysis is smaller than the tirzepatide trial result because it combines different drugs and trials. That is not a contradiction. It is a warning against treating the drug class as one uniform intervention. Liraglutide and tirzepatide are not interchangeable in the OSA evidence, and tirzepatide itself is a dual GIP/GLP-1 agonist rather than a plain copy of older GLP-1 receptor agonists.[1][2]
The fairest comparison is not a true head-to-head trial
There is a practical problem with confident “GLP-1 vs CPAP” claims: the strongest comparative statements are not coming from a direct randomized trial that assigns similar patients to CPAP or a GLP-1 drug and follows AHI as the primary endpoint. The 2026 network meta-analysis is useful because it compares interventions across a broader evidence network, but that is still not the same thing as a direct head-to-head RCT.[1]
Network meta-analysis can help rank treatments, especially when direct comparisons are missing. It cannot erase the differences between trial populations, adherence patterns, background therapy, follow-up time, and drug exposure. That matters here because CPAP’s outcome depends heavily on nightly use, while GLP-1 outcomes depend on dose escalation, tolerability, weight response, and continued treatment.
Still, the pattern is clinically coherent. The network meta-analysis found CPAP superior for AHI, while GLP-1 receptor agonists were superior for BMI and HbA1c. That is almost exactly what mechanism would predict: the machine wins at splinting the airway; the medication wins at changing metabolic terrain.[1]
When using both makes more sense than choosing one
For many eligible adults with obesity-related moderate-to-severe OSA, the most defensible plan is staged: keep the airway protected with PAP while using medication to reduce the metabolic burden that helped make the airway vulnerable in the first place. That approach is less dramatic than “the shot replaces the mask,” but it fits the evidence better.
SURMOUNT-OSA included people who were using PAP and people who were not. In the subgroup using PAP, tirzepatide users lost about 50 pounds, or 20% of body weight, compared with about 45 pounds, or 18%, in those not using PAP.[3] That does not prove CPAP makes the drug work better. It does suggest that staying on PAP does not prevent substantial medication-associated weight loss, which is often the fear behind abandoning the machine too early.
The combination signal also appears in the 2026 network meta-analysis: liraglutide plus CPAP produced the greatest BMI reduction among studied interventions, with a mean difference of −2.00 kg/m².[1] That finding should be read carefully. It supports complementarity, not a guarantee that every patient will lose more weight simply because CPAP and a GLP-1 are prescribed together.
Real-world data point in the same general direction, though with the usual limits of observational evidence. Resmed and IQVIA reported that patients prescribed a GLP-1 were 10.8 percentage points more likely to initiate CPAP than those without a GLP-1 prescription.[4] That may reflect better engagement, more clinical contact, insurance patterns, motivation, or other confounding. It is not proof that GLP-1 prescriptions cause CPAP uptake. But it does undermine the lazy assumption that medication and PAP are always competing choices.
A staged decision framework
The decision usually becomes clearer when it is sorted by patient type rather than by treatment loyalty.
Likely add-on candidates
The strongest case for GLP-1 therapy is an adult with obesity-related moderate-to-severe OSA who still needs airway protection now but also has a clear metabolic driver that CPAP cannot treat. This is the patient whose AHI may improve meaningfully if body weight, blood pressure, and inflammatory burden improve, but who should not be left untreated during the months it takes to find out.
- Continue CPAP or PAP while medication is started and titrated.
- Track symptoms, weight, blood pressure, and medication tolerability, but do not treat those as substitutes for AHI.
- Repeat sleep testing before changing PAP settings or stopping therapy.
- Expect the medication question to be long-term, because stopping therapy may allow weight regain and OSA worsening.
Possible candidates for reducing CPAP reliance later
Some patients may eventually need less pressure, fewer nights of PAP in selected circumstances, or a different long-term OSA plan. That should be earned by measured improvement, not assumed from weight loss alone. A lower number on the scale is encouraging; a lower AHI on a follow-up sleep study is the evidence that the airway is actually behaving differently during sleep.
The SURMOUNT-OSA threshold is useful here because it combined AHI below 15 with symptom resolution in 42–50% of tirzepatide-treated participants.[3] That is closer to a clinically meaningful destination than weight loss alone. Even then, it leaves many patients who improved but did not cross that line.
Poor candidates for treating GLP-1 therapy as a substitute
People without obesity, or whose OSA is mainly driven by craniofacial anatomy, enlarged tonsils, neuromuscular factors, sedative exposure, or other non-weight-related causes, should be cautious about expecting a GLP-1 drug to solve the airway problem. Roughly 20% of OSA is non-obesity-related, and that group is not the group most likely to benefit from a weight-mediated treatment pathway.
The same caution applies to anyone with severe daytime sleepiness, safety-sensitive driving or work, major oxygen desaturation, or cardiovascular risk that makes untreated OSA especially dangerous. In those situations, waiting months to see whether a drug lowers AHI enough is not a neutral experiment. It is time spent with an airway that may still be collapsing night after night.
The hard part is not knowing CPAP works. It is knowing what to do when you cannot stand it
Patients who hate CPAP do not need another lecture that begins and ends with “just use it.” Mask leak, pressure intolerance, dry mouth, claustrophobia, noise, travel, bed-partner awkwardness, and the simple resentment of being tethered to a machine can make perfect physiologic sense feel impossible at 2 a.m.
But CPAP difficulty should trigger troubleshooting, not premature replacement. Different masks, humidification, pressure adjustments, bilevel PAP, positional therapy, oral appliances, and ENT evaluation may all enter the conversation depending on the patient. A GLP-1 drug can be part of that conversation when obesity is a major driver, but it should not quietly become permission to leave moderate-to-severe OSA untreated while hoping weight loss catches up.
There is also a durability problem that does not get enough airtime in excited coverage. GLP-1–based obesity treatment is generally chronic therapy. If the medication is stopped and weight returns, the OSA improvement may also fade. Current OSA trial data do not establish durable protection beyond long-term continued treatment, and SURMOUNT-OSA followed patients for 52 weeks.[3]
A practical bottom line
For eligible adults with obesity-related moderate-to-severe obstructive sleep apnea, GLP-1–based therapy is best understood as a metabolic add-on and, for some patients, a supervised pathway toward less CPAP dependence. It can reduce AHI, body weight, blood pressure, and metabolic risk over time. Tirzepatide in particular has produced large OSA improvements in the studied population.
CPAP remains the treatment that protects the airway immediately. That does not make it morally superior, and it does not make mask intolerance trivial. It means its job is different. If a GLP-1 drug changes the underlying terrain enough, the CPAP plan may change later. The safe sequence is to prove that with follow-up testing rather than assuming it because the scale, the headlines, or the prescription changed.
References
- Chiappa et al. network meta-analysis, Diabetes, Obesity and Metabolism, February 2026.
- Dandamudi et al. 2026 meta-analysis, PMC.
- Tirzepatide for the Treatment of Obstructive Sleep Apnea and Obesity, The New England Journal of Medicine.
- Emerging Therapies, Resmed.






Comments
Join the discussion with an anonymous comment.