A lung transplant can make the numbers look better while the nights still feel broken. Someone may breathe with less effort, walk farther than before surgery, and still wake up after three restless hours wondering whether this is medication, anxiety, rejection, sleep apnea, or just the price of recovery.
That contradiction is not rare, and it is not simply a failure to relax. Sleep quality after lung transplant appears to behave differently from sleep after several other solid-organ transplants. In reviews comparing transplant populations, kidney, liver, and heart recipients often show some improvement in sleep after surgery, while lung transplant recipients do not show the same reliable improvement; across lung transplant studies, poor sleep has been reported in 32% to 81% of recipients, depending on the measure and timing used.[1][2]

One recent study gives the problem a sharper outline. Among 88 lung transplant recipients, 74% met the Pittsburgh Sleep Quality Index threshold for poor sleep, and the mean PSQI score was 7.1, above the usual cutoff of greater than 5 for poor sleep quality.[3] A number like that should change the tone of the conversation. Poor sleep after lung transplant is common enough that it deserves to be asked about directly, but complex enough that "try better sleep hygiene" is too thin an answer.
Why better breathing does not always mean better sleep
Before transplant, sleep may be disrupted by advanced lung disease itself: shortness of breath, oxygen needs, coughing, fear, hospitalizations, and the exhausting uncertainty of waiting. It would be reasonable to expect that once the diseased lungs are replaced, sleep would rebound. For many recipients, part of life does improve. But sleep has more moving parts than airflow alone.
After surgery, the body is living with new demands: lifelong immunosuppression, close symptom surveillance, infection precautions, clinic visits, changing exercise capacity, and the mental work of surviving something enormous. The same recipient may be relieved, grateful, frightened, physically uncomfortable, and alert to every new cough. None of that fits neatly into a bedtime routine.
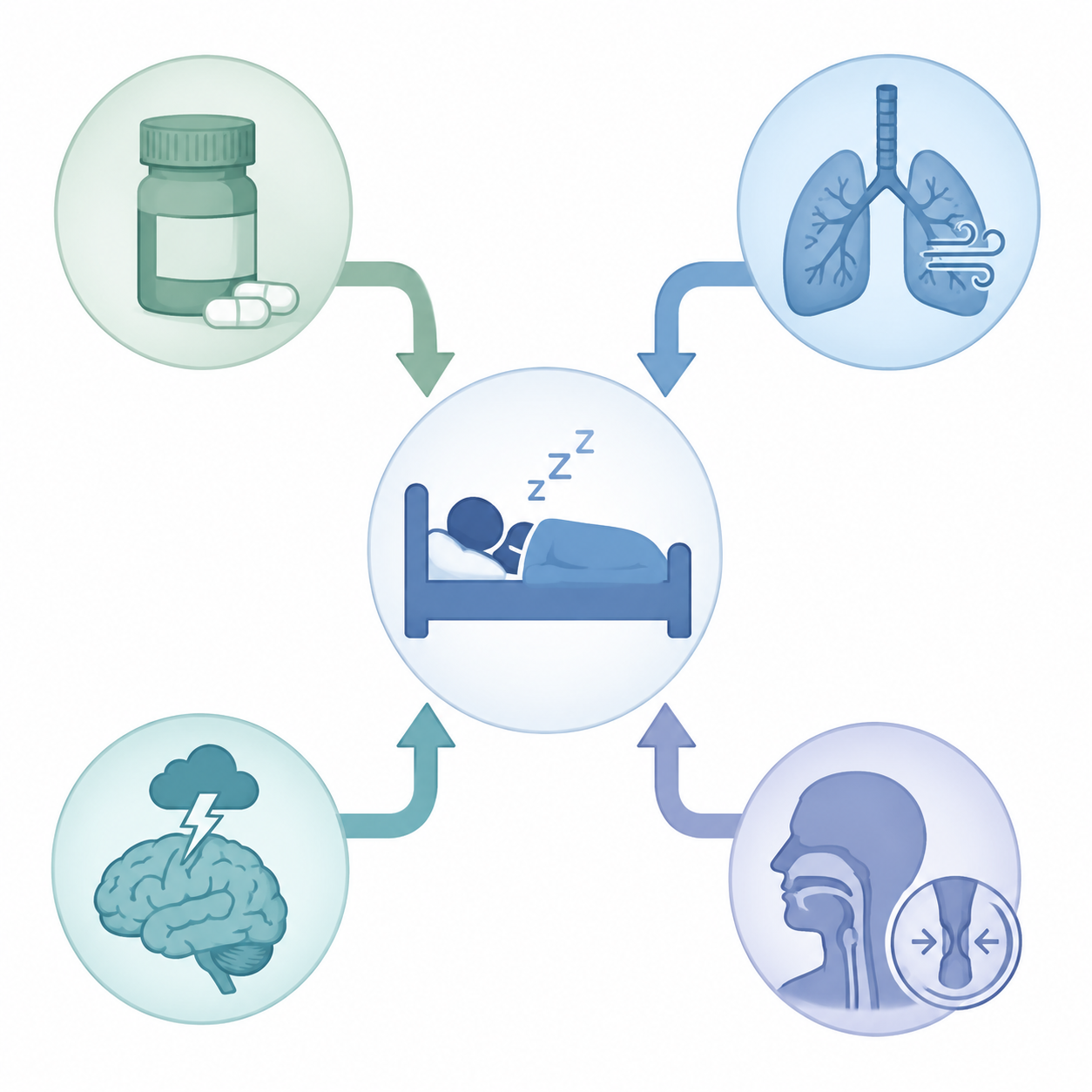
The useful way to think about lung transplant recovery sleep quality is not as one problem with one fix, but as several overlapping problems that can feel identical at 2 a.m. Insomnia from medication, wheezing that wakes the body before the mind notices it, depression that flattens daytime energy, anxiety that keeps the nervous system on duty, and obstructive sleep apnea can all present as "I am not sleeping." They need different responses.
Immunosuppressants can keep the brain switched on
Medication effects are one of the most transplant-specific reasons sleep advice often misses the mark. Lung recipients do not take immunosuppressants as optional add-ons; these drugs protect the transplanted lungs. But some of the same medications that protect the graft can also disturb sleep.
Tacrolimus and corticosteroids have both been linked with insomnia after lung transplantation.[4] A recipient may describe this as feeling wired, waking repeatedly, or being unable to return to sleep after an early-morning awakening. A caregiver may notice that sleep worsens after a medication adjustment or during a steroid burst. That pattern is worth reporting, not because the patient should independently change the dose, but because timing, dose changes, and competing causes can only be sorted out safely with the transplant team.
This is also where ordinary insomnia advice can accidentally sound accusatory. If a person is taking a medication known to disturb sleep, then lying awake is not evidence of poor discipline. It is a clinical clue.
Respiratory symptoms still matter after the operation
A transplanted lung does not make every respiratory symptom meaningless. Cough, sputum, wheezing, infections, airway issues, reflux-related irritation, and other post-transplant problems can still fragment sleep. Some symptoms wake the person fully. Others may pull sleep into lighter stages without leaving a clear memory of why the night felt bad.
In the 2025 study of 88 recipients, wheezing was associated with much higher odds of poor sleep, with an odds ratio of 10.88.[3] That result is attention-getting, but it needs careful handling: the confidence interval was very wide, from 1.65 to 222.02, which means the estimate is imprecise and should not be treated as settled law.[3] The practical takeaway is narrower and still important. Wheezing that shows up with poor sleep deserves a transplant-team conversation. It should not be dismissed as just nighttime annoyance.
The same study also found that a hospital stay longer than 30 days was associated with seven-fold higher odds of being in the worst sleep-quality group.[3] That does not mean a long hospitalization causes chronic poor sleep by itself. It does suggest that people with more complicated recoveries may carry a heavier sleep burden later, and they may need sleep assessed as part of recovery rather than as a separate lifestyle issue.
Anxiety and depression are not side notes
Poor sleep after transplant is sometimes described as if the body is the serious part and distress is the soft part. That split is not useful. The transplant recipient has lived through respiratory failure, surgery, intensive monitoring, medication uncertainty, and the ongoing knowledge that symptoms may matter. Sleep is exactly where that vigilance can become visible.
In the Moon et al. study, anxiety was present in 23.9% of recipients and depression in 30.7%.[3] The strongest predictor of poor sleep was combined anxiety and depression, associated with an odds ratio of 13.72 for poor sleep.[3] That figure does not say distress is the only driver. It does say that when anxiety and depression travel together, sleep complaints need to be treated as part of the clinical picture, not as background noise.
This matters for caregivers, too. A person who wakes often may not be able to tell whether they are anxious because they slept poorly or sleeping poorly because they are anxious. The direction can run both ways in daily life. What helps is not debating which came first, but screening for distress and treating it without shame.
Sleep apnea can increase after transplant
Obstructive sleep apnea is easy to miss in this setting because the transplant story seems to point elsewhere. If someone is exhausted after lung transplant, the first guesses may be medication, deconditioning, mood, infection worry, or recovery from surgery. Those may be real. But sleep-disordered breathing can sit underneath them.
One study of sleep-related breathing disorders found that obstructive sleep apnea prevalence rose from 38% before lung transplant to 86% six months after transplant.[5] That is a striking shift, and it makes routine suspicion reasonable, especially when poor sleep comes with snoring, witnessed pauses in breathing, morning headaches, dry mouth, high blood pressure, nocturnal oxygen changes, or heavy daytime sleepiness.

A sleep evaluation should not feel like a punishment or an accusation. For a lung transplant recipient, it can be a normal extension of respiratory follow-up: checking whether the airway stays open during sleep, whether oxygen levels drop, and whether a treatable breathing disorder is stealing recovery time.
Why clinicians should not wave this away
Sleep quality is easy to under-rank in transplant care because there are more urgent-sounding words in the room: rejection, infection, bronchoscopy, spirometry, immunosuppression, chronic lung allograft dysfunction. But poor sleep is not only about comfort.
In the UCSF Breathe Again cohort of 141 lung transplant recipients, worse sleep was associated with worse patient-reported outcomes and with clinical outcomes. Each minimally important difference worsening on the Sleep Problems Index was associated with a 29% higher mortality risk, and recipients in the worst sleep quartile had a 2.18-fold higher risk of chronic lung allograft dysfunction.[6]
Those findings should be taken seriously and not over-read. This was a single-center cohort, and the results show association, not proof that poor sleep causes CLAD or death, or that treating insomnia will prevent those outcomes. Still, the signal is strong enough to make one point plain: when a lung transplant recipient keeps saying, "I am just not sleeping," that complaint belongs in the medical conversation.
What actually helps
The safest next step depends on the pattern. The goal is not to collect more bedtime rules. It is to identify which driver is most likely keeping sleep poor and match the response to that driver.
| If the pattern looks like this | Ask about this | Why it matters |
|---|---|---|
| Snoring, witnessed pauses, morning headaches, oxygen drops, or heavy daytime sleepiness | Sleep apnea evaluation or screening | OSA may become more common after transplant and is treatable. |
| Wired feeling, new insomnia after medication changes, or worse sleep during steroid periods | Medication timing and side-effect review with the transplant team | Tacrolimus and corticosteroids have been linked with insomnia. |
| Wheezing, cough, sputum, or nighttime breathing discomfort | Respiratory symptom assessment | Night symptoms can fragment sleep and may signal a treatable issue. |
| Persistent worry, low mood, panic-like awakenings, loss of interest, or guilt about struggling | Anxiety and depression screening | Combined anxiety and depression strongly tracks with poor sleep. |
| Trouble falling asleep, long awakenings, clock-watching, and fear of the bed becoming another failure | CBT-I | It treats insomnia without adding sedative drug burden. |
Ask specifically about sleep apnea screening
If there is one practical issue that deserves more attention in lung transplant recovery sleep quality, it is sleep apnea. The post-transplant rise reported in the sleep-related breathing disorder study is too large to leave apnea as an afterthought.[5] A recipient does not need to fit the old stereotype of an apnea patient before it is worth asking.
The question can be simple: "Given my transplant history and ongoing poor sleep, should I be screened for obstructive sleep apnea or have a sleep study?" The transplant team can decide whether home testing, in-lab polysomnography, oximetry review, or referral to a sleep specialist fits the situation. If positive airway pressure is recommended, it should be coordinated with the transplant and sleep teams so mask fit, infection precautions, airway comfort, and adherence problems are handled early.
Use CBT-I as the main insomnia treatment, not as a consolation prize
Cognitive behavioral therapy for insomnia, or CBT-I, is often misunderstood as a nicer name for sleep hygiene. It is more structured than that. CBT-I works with the learned patterns that keep insomnia going: spending too much time awake in bed, irregular sleep timing, fear of not sleeping, clock monitoring, and the gradual loss of confidence that sleep will happen.
For lung transplant recipients, its strongest advantage is safety. It does not add drug interactions, does not increase fall risk, and does not suppress breathing. The limitation is also important: the CBT-I recommendation in this specific population is largely extrapolated from broader insomnia care rather than proven by a lung-transplant-specific randomized trial. Even with that gap, it is a sensible first-line approach in medically complex patients because it treats insomnia without adding another medication problem.
The same reasoning is used in other medically sensitive sleep situations. For example, Restful Ground's discussion of CBT-I as a first-line sleep aid during pregnancy makes the same basic point: when medication choices are constrained, behavioral insomnia treatment moves from "nice to try" to clinically practical.
A transplant recipient starting CBT-I should still tell the therapist about transplant status, infection precautions, medication schedules, fatigue patterns, and any instructions from the transplant team. Sleep restriction, for example, may need careful tailoring in someone with severe fatigue, fall risk, or unstable medical symptoms. Good CBT-I is not rigid; it is structured enough to work and flexible enough to respect the body in front of it.
Be cautious with sleeping pills
The understandable impulse is to ask for a pill, especially when sleep has been poor for months. But after lung transplant, sedatives deserve extra caution. Cleveland Clinic's lung transplant recovery guidance explicitly tells patients not to take sleeping pills, stating that they are "very harmful when taken with other transplant medications."[7]
That warning should not be stretched beyond what it says. The available material here does not map every possible sedative against every immunosuppressant. It does, however, support a conservative rule: do not self-treat post-transplant insomnia with sleeping pills, over-the-counter sedatives, cannabis products, alcohol, or borrowed medication. If medication is being considered, it belongs in a transplant-aware discussion that weighs interactions, breathing effects, delirium risk, falls, and next-day impairment.
Target the branch that is actually active
Some sleep problems improve when a respiratory symptom is treated. Some improve when steroid timing changes, if the transplant team says that is safe. Some improve only after anxiety, depression, or trauma symptoms are addressed directly. Some will not move much until sleep apnea is diagnosed and treated. A person can also have more than one branch active at once, which is why one failed intervention does not mean the sleep complaint was exaggerated.
Basic sleep habits still have a place, but they should not carry the whole burden. A consistent wake time, light exposure in the morning, a cool bedroom, reduced late caffeine, and less clock-watching can support treatment. They cannot substitute for evaluating wheezing, medication-related insomnia, depression, or sleep apnea in a lung transplant recipient who remains exhausted.
Persistent poor sleep after lung transplant is common, multifactorial, and clinically worth addressing. The strongest path is targeted evaluation and non-drug insomnia care: ask about sleep apnea when symptoms fit, bring medication and breathing patterns to the transplant team, screen and treat distress, and consider CBT-I early rather than waiting until sleep has become another long-term complication.
References
- Sleep Quality in Adult Lung Transplant Recipients - SAGE, 2022.
- Self-reported poor sleep in solid organ transplant - ScienceDirect.
- Exploring Factors Associated with Sleep Quality After Lung Transplantation - PMC, 2025.
- Insomnia and Immunosuppressant Therapy After Lung Transplantation - SAGE.
- Sleep-Related Breathing Disorders and Lung Transplantation - PubMed.
- Disturbed sleep after lung transplantation is associated with worse patient-reported outcomes and CLAD - PMC.
- Discharge, Planning & Recovery - Cleveland Clinic.






Comments
Join the discussion with an anonymous comment.