The hard part of sleep recovery after cartilage transplant surgery is not simply finding a comfortable position. It is finding a position that stays inside your surgical rules while you are half-asleep, sore, and tired of negotiating with a brace. For many cartilage procedures, the nighttime problem has three moving parts: the brace may need to stay locked straight, the leg may need to remain non-weight-bearing for weeks, and the continuous passive motion machine may already be taking up hours of the day.
That is why advice borrowed from ACL repair, meniscus trimming, or total knee replacement can mislead you. MACI consensus recommendations describe different weight-bearing paths by lesion location: tibiofemoral lesions commonly require 7 to 9 weeks before full weight-bearing, while patellofemoral patients may weight-bear immediately with the brace locked, though these consensus guidelines were sponsored by Vericel, the MACI manufacturer, and individual surgeon protocols still override general timelines.[1]
| Recovery period | What usually matters most at night | Sleep priority |
|---|---|---|
| First nights after surgery | Brace locked in extension, swelling, pain medication timing, bathroom safety | Back-sleeping setup that protects extension and makes transfers predictable |
| Non-weight-bearing weeks | Crutches or walker, brace rules, fatigue from CPM and daytime rehab tasks | Repeatable evening routine: CPM earlier, cold therapy and medication timed before bed |
| Brace unlocking or partial weight-bearing phase | More position options, but still limited by surgeon-specific restrictions | Introduce side-sleeping only when allowed, usually with a pillow between the knees |
| Later return toward normal sleep | Residual stiffness, soreness after activity increases, habit retraining | Gradually remove supports only when extension, swelling, and brace rules allow it |
Start With the Rule That Beats Comfort
If your discharge papers say to sleep with the brace locked in full extension, treat that as the frame for every other sleep decision. The brace is not just there to keep you from kicking in your sleep. It helps protect the repair from positions and loads your knee is not ready to handle.
The detail patients often miss is where the pillows go. Osteochondral allograft discharge instructions from Twin Cities Orthopedics tell patients to place pillows under the heel, not under the knee, while sleeping, because a pillow under the knee encourages the knee to rest in flexion and can contribute to a flexion contracture.[2]
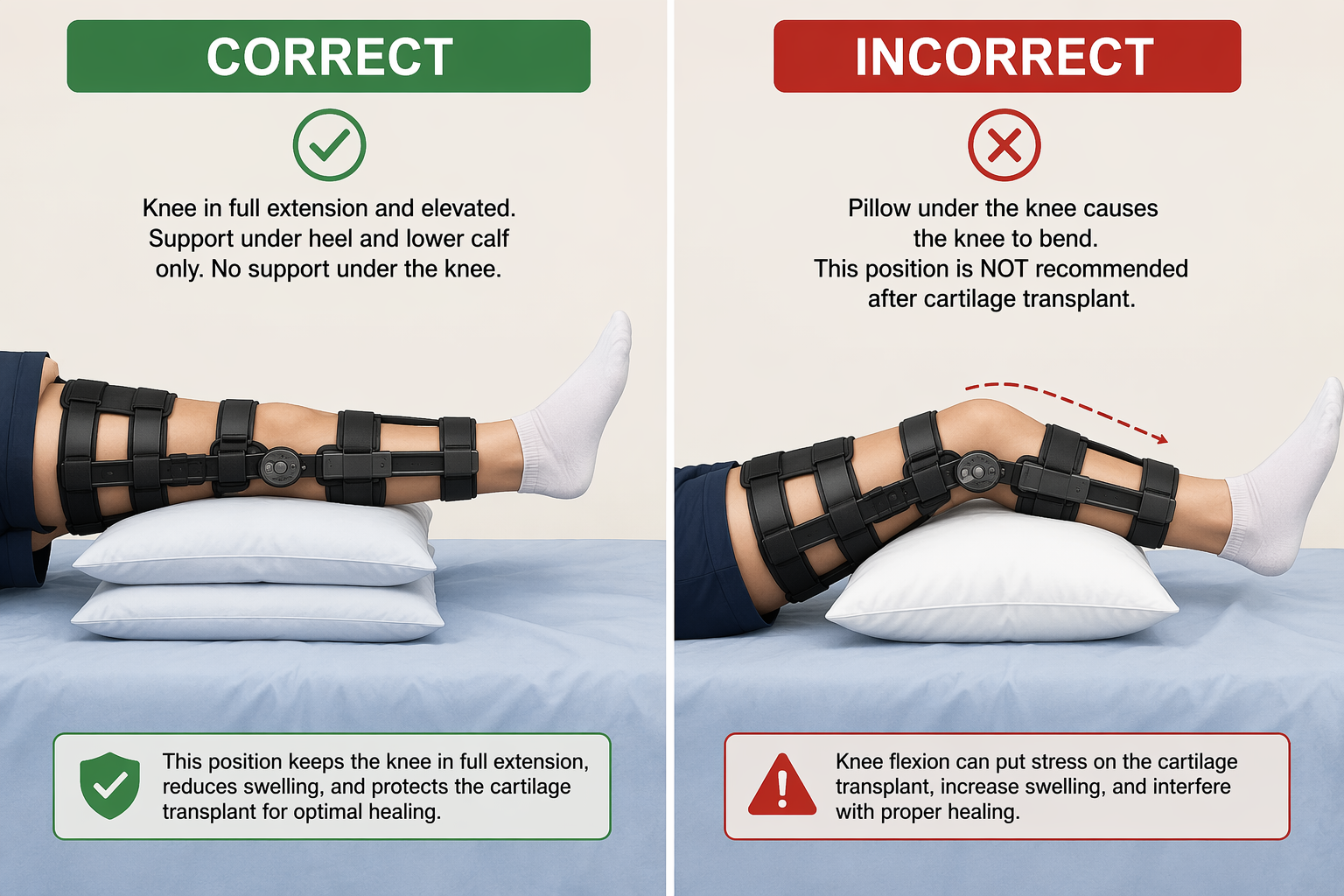
A comfortable bend under the knee can feel merciful at 2 a.m. It can also work against the goal of regaining full extension. If your surgeon has ordered heel elevation, build the bed around that instruction rather than around whatever feels softest in the moment.
The First Nights: Make Back-Sleeping Boring and Repeatable
The first nights are usually when people improvise the most, and improvising is exactly what makes the room feel unsafe. Set up the bed before you are exhausted: brace straps checked, heel supported, cold therapy arranged if prescribed, medication schedule visible, crutches or walker on the surgical-leg side your therapist recommends, and a clear path to the bathroom.

For most patients under a locked-extension order, the safest default is supine sleeping: on your back, surgical leg straight, heel supported as instructed, and no wedge or pillow pushing the knee into a bend. If back-sleeping is new for you, the goal is not to love it immediately. The goal is to remove decisions from the middle of the night. A small pillow under the non-surgical knee, a pillow along either side of the torso, or a light blanket tucked at the hips can reduce the urge to roll without trapping you.
If your lower back complains, adjust the support around your pelvis and non-surgical leg rather than bending the surgical knee. You can use a separate guide to train yourself to sleep on your back or review the biomechanics of back-friendly sleep, but keep the surgical instruction above the generic comfort rule.
- Put the phone, water, medication log, and ice-machine control where you can reach them without twisting.
- Use a night-light so bathroom trips do not begin with fumbling in the dark.
- Keep the floor clear of cords, loose blankets, pets, and CPM tubing.
- Plan the first bathroom route while fully awake, including where the crutches or walker will be when you stand.
- If you are alone overnight, ask your care team what level of help is appropriate for transfers during the first few days.
Why Sleep Feels So Fragile After Surgery
There are no peer-reviewed sleep studies specifically following cartilage transplant patients, so the best available sleep data comes from hip and knee arthroplasty populations. That matters because those patients are often older and may weight-bear much sooner than a cartilage transplant patient. The data is still useful for understanding why the first nights can feel disproportionate to the phrase “routine recovery.”
In an actigraphy study of hip and knee arthroplasty patients, sleep efficiency dropped by about 10.8% on the first postoperative night, sleep latency increased by about 18.7 minutes, and pain scores on postoperative day 1 averaged 4.58 out of 10; higher pain correlated with lower sleep efficiency.[3] Another review reports that REM sleep can be absent on the first postoperative night, that even one hour of sleep loss can alter pain perception, and that postoperative sleep disturbance independently predicts functional impairment at 3 months.[4]
Those findings do not prove the same numbers apply to MACI, ACI, or OATS. They do explain why a patient can feel trapped in a loop: pain delays sleep, poor sleep amplifies pain, and the next day’s rehab tasks feel heavier.
Medication Timing Is Part of the Sleep Setup
Pain medication is not a full sleep plan, but poor timing can undo an otherwise careful setup. If your surgeon has prescribed a medication schedule that allows it, ask whether taking the evening dose roughly an hour before bedtime makes sense so the effect is rising as you try to fall asleep. The point is not to sedate yourself into ignoring the protocol; it is to avoid climbing into bed exactly when pain is starting to surge.
Opioids deserve special care. They may be appropriate after surgery, but they can suppress REM sleep and worsen sleep-disordered breathing, so more medication does not automatically mean better sleep.[4] Evidence from hip and knee arthroplasty also suggests that opioid-free or opioid-sparing multimodal analgesia can improve postoperative sleep quality, though that evidence is not cartilage-transplant-specific.[5]
A practical evening sequence often works better than scattered rescue decisions: finish CPM during waking hours, eat if medication requires food, use cold therapy as prescribed, take scheduled pain medication at the approved time, then get into the final brace-and-pillow position before you are too drowsy to check it. If your pain is repeatedly breaking through before the next allowed dose, that is a dosing-plan problem to discuss with the surgical team, not a reason to invent your own schedule.
Keep CPM Out of the Night
Continuous passive motion is already demanding because it turns recovery into a time-management exercise. Unless your surgeon specifically tells you otherwise, treat CPM as an awake-hours task. Running it at night can add noise, tubing, alarms, brace transitions, and half-awake repositioning to the very hours when your nervous system is trying to settle.
The better question is not “Can I sleep through CPM?” but “Where can I place CPM so it does not steal sleep?” Some patients do best with sessions divided across morning, afternoon, and early evening. Others need the last session finished well before bedtime so swelling, icing, bathroom trips, and medication timing are not all compressed into the same hour.
| Task | Better timing for most patients | Why it helps sleep |
|---|---|---|
| CPM session | Awake hours, often earlier in the evening rather than right before bed | Reduces nighttime equipment disruption and rushed transfers |
| Cold therapy, if prescribed | After activity or CPM, with skin checks and time limits from the care team | Helps swelling without turning the bed into a treatment station |
| Evening pain medication | At the approved interval, often planned before bedtime rather than after pain peaks | Aligns pain control with sleep onset when clinically appropriate |
| Final bathroom trip | After brace and crutch setup is ready but before drowsiness | Reduces risky half-asleep transfers |
The Non-Weight-Bearing Weeks Are a Different Sleep Problem
The multi-week non-weight-bearing phase is where cartilage recovery separates itself from many knee procedures. It is not just “a few rough nights.” It can be weeks of planning every drink of water around bathroom logistics, every blanket around brace friction, and every late-day activity around whether the knee will throb once the room goes quiet.
During this stretch, protect the boring routine. Keep the same side of the bed if transfers are working. Keep the same crutch placement. Keep the same pillow configuration unless your surgeon or therapist changes the order. If the brace rubs, ask about approved padding or strap adjustment rather than loosening it into a position that no longer holds the knee as prescribed.
Room changes can help, but they should stay in their lane. A cooler bedroom, steady background sound, and fewer bright screens can reduce unnecessary wakefulness. If noise or temperature is the main issue, a guide to sleeping with a fan on may be useful. These changes support the surgical setup; they do not replace it.
When Side-Sleeping Becomes Possible
Do not use side-sleeping as a workaround while the knee is still ordered to stay locked straight at night. Once your surgeon allows brace unlocking, partial weight-bearing, or more flexible positioning, side-sleeping may become realistic again. The usual starting point is lying on the non-surgical side with a firm pillow between the knees and lower legs so the surgical knee does not sag inward or twist.
If you are cleared to lie on the surgical side, introduce it cautiously and stop if pressure around the incision, graft area, or brace creates pain that lingers after you change positions. A pillow between the knees can still help keep the hips and knees from collapsing into rotation. For general positioning ideas, use a broader guide to sleep positions for back pain, but filter every suggestion through your cartilage protocol.
What to Confirm Before You Change the Routine
Cartilage transplant protocols vary because the operation varies. MACI, ACI, OATS, osteochondral allograft, tibiofemoral lesions, and patellofemoral lesions do not all create the same nighttime rules. Lesion size, graft location, concomitant procedures, and surgeon preference can change the brace, CPM, and weight-bearing plan.
- Ask whether your brace must stay locked in full extension during sleep, and for how long.
- Ask whether heel elevation is required and whether any support may touch the back of the knee.
- Ask when side-sleeping is allowed and whether the brace must stay on for it.
- Ask how many CPM hours are expected per day and whether they should be completed during waking hours.
- Ask what pain pattern should trigger a medication adjustment call rather than another bad night.
Call your clinical team promptly if pain is worsening instead of gradually improving, you cannot sleep despite taking medication as prescribed, opioids cause breathing problems, severe drowsiness, or concerning confusion, or you notice symptoms your discharge instructions flagged as urgent. A sleep plan is useful only while it stays inside the medical plan.
Sleep after cartilage transplant surgery becomes more manageable when the bedroom is treated as part of the protocol: brace first, heel support first, CPM during waking hours, medication timed deliberately, and position changes only when the surgeon’s rules allow them.
References
- MACI consensus guidelines from U.S. orthopedic surgeons - Cartilage, 2021 - link
- Osteochondral allograft discharge instructions - Twin Cities Orthopedics - link
- Actigraphy study of hip/knee arthroplasty - International Orthopaedics, 2023 - link
- Postoperative sleep disorders and their potential impacts on surgical outcomes - Journal of Biomedical Research, 2020 - link
- Opioid-free or opioid-sparing multimodal analgesia and sleep quality after hip/knee arthroplasty - Journal of Family Medicine and Primary Care, 2020 - link






Comments
Join the discussion with an anonymous comment.