Oral appliance therapy for sleep apnea lives in an uncomfortable middle ground. CPAP usually lowers the apnea-hypopnea index, or AHI, more powerfully on nights when it is used. A mandibular advancement oral appliance usually lowers AHI less. Yet in studies that look beyond the sleep lab and into actual use, oral appliances can produce health outcomes that look surprisingly close to CPAP for many people with mild-to-moderate obstructive sleep apnea.
That is not because comfort magically becomes treatment. It is because treatment has two parts: how well it works while worn, and how often it is actually worn. CPAP has the stronger per-night effect. Oral appliance therapy often has the stronger use pattern. In objective monitoring studies, oral appliance users averaged about 6.4 to 6.7 hours of nightly wear, and 84% to 89% were regular users at one year; long-term CPAP compliance is often described around 50%, with some studies reporting abandonment as high as 60%.[1][2]

So the real question is not whether oral appliances are “as strong” as CPAP in a technical sense. They generally are not. The better question is whether a less potent therapy that is used more consistently can relieve enough disease burden to matter. For a meaningful group of patients, the answer is yes. For another group, it is no. The hard part is telling those groups apart and checking the result instead of assuming comfort equals control.
What Oral Appliance Therapy Actually Is
In sleep apnea care, oral appliance therapy usually means a custom mandibular advancement device. It is worn in the mouth during sleep and holds the lower jaw forward to help keep the upper airway from collapsing. It is mainly used for obstructive sleep apnea, especially mild-to-moderate disease, and it should be selected after a clinical diagnosis rather than as a self-directed snoring fix.[1]
The custom part matters. Over-the-counter mouthguards may look similar to a patient standing in a pharmacy aisle, but treatment-grade oral appliances are fitted and adjusted by qualified dental sleep providers working with sleep clinicians. The device has to move the jaw enough to affect the airway without creating unnecessary jaw pain, tooth pressure, or bite changes. That balance is not a one-night decision.
Efficacy Is Not the Same as Effectiveness
A sleep study mostly measures efficacy: what happens to breathing events while the treatment is in place under measured conditions. CPAP usually wins that contest because pressurized air can splint the airway open throughout the night. Oral appliances work mechanically and indirectly, by changing jaw and tongue position, so their AHI reduction is more variable.
Effectiveness is the messier measure. It asks what happens after the prescription, when the patient is congested, tired, traveling, sleeping next to a partner, dealing with mask leaks, or deciding whether jaw pressure is worth another night. A treatment that is highly efficacious but often unused loses much of its practical value. A treatment with moderate efficacy can still matter if it is worn almost every night for most of the night.
| Question | CPAP | Oral appliance therapy |
|---|---|---|
| Which tends to reduce AHI more per night? | CPAP | Usually less than CPAP |
| Which tends to be used more consistently long term? | Often limited by comfort and tolerance | Often higher use in objective adherence data |
| Which has stronger evidence as the technical benchmark? | CPAP | Alternative for selected patients, especially mild-to-moderate OSA |
| Which needs objective follow-up? | Yes, to confirm pressure, control, and use | Yes, to confirm the appliance actually reduces breathing events |
This distinction explains why a clinician might prescribe an oral appliance without pretending it is the same machine in a smaller form. The goal is not to crown the more elegant device. The goal is to reduce disease burden in a person who has to live with the treatment.
The Adherence Data Changes the Conversation
For years, one weakness in oral appliance research was that adherence often came from self-report. That matters because people are not always precise reporters of nightly device use, and because CPAP machines can record use electronically. The comparison was not clean.
Microsensor monitoring made the oral appliance side less vague. In Vanderveken and colleagues’ objective compliance study, embedded sensors measured oral appliance wear. The reported nightly use was 6.4 to 6.7 hours, and 84% to 89% of patients were regular users at one year.[2] That does not erase sample-size limits or make every patient a nightly user. It does mean that “patients say they like it” is no longer the only adherence argument.
The Phillips randomized trial gives the tradeoff clinical weight. In a head-to-head comparison of CPAP and oral appliance treatment, CPAP reduced AHI more, but improvements in blood pressure, sleepiness measured by Epworth scores, and quality-of-life measures were not significantly different at one month and six months.[3] That is the kind of result that makes sense only if nightly physiology and nightly behavior are considered together.
This does not mean oral appliances are equivalent to CPAP for every endpoint, every patient, or severe sleep apnea. It means that for selected patients, especially in the mild-to-moderate range, the practical outcome can converge because the therapy that is somewhat less potent may be used more faithfully.
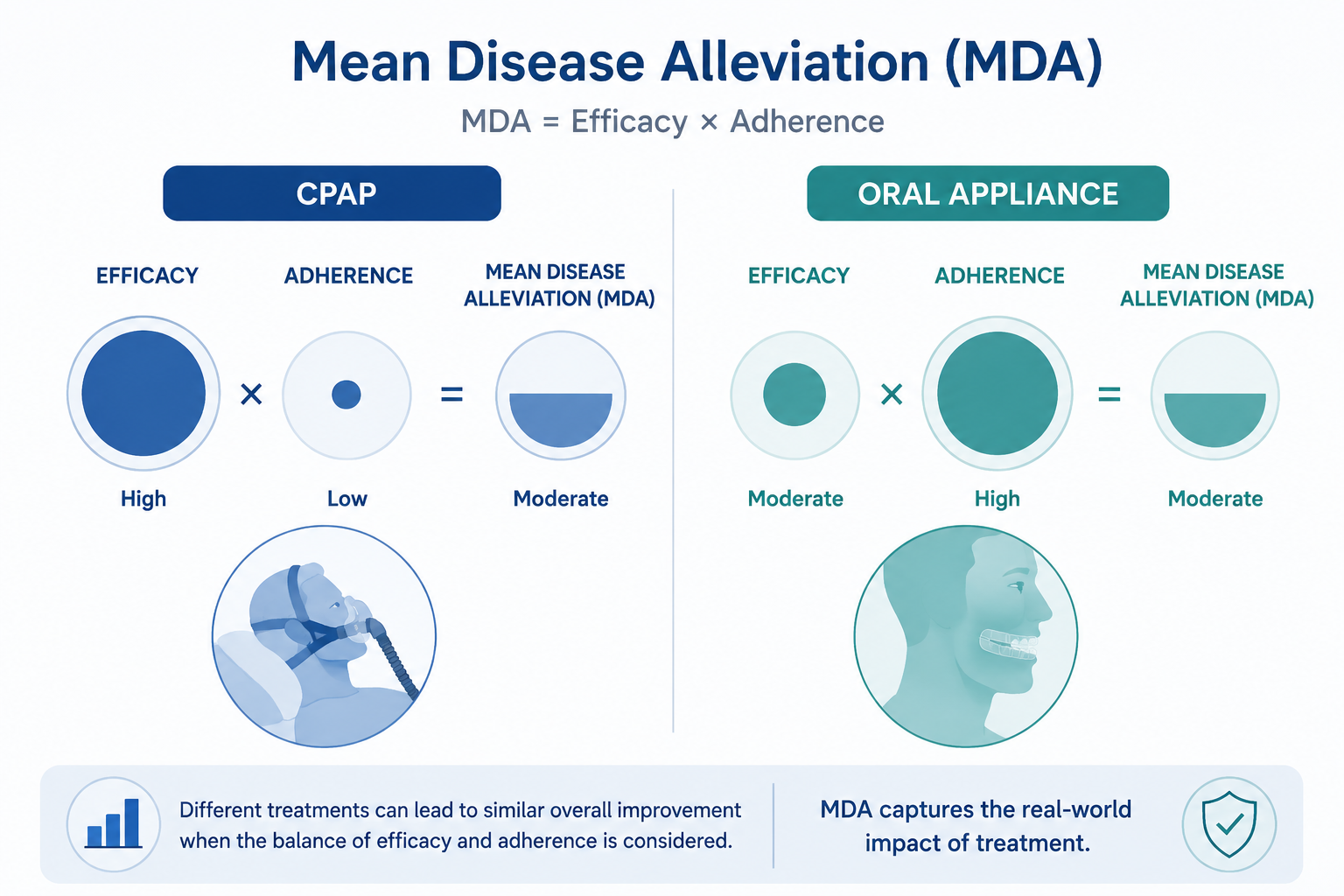
Mean Disease Alleviation: Why the Tradeoff Can Add Up
Mean Disease Alleviation, often shortened to MDA, is useful because it refuses to look at AHI reduction alone. It combines efficacy and adherence into one estimate of how much disease is actually being alleviated across real use. In the review by Dieltjens and Vanderveken, oral appliance therapy had an MDA of about 51% to 55%, a range described as comparable to CPAP once CPAP’s stronger efficacy is reduced by lower long-term adherence.[1]
A simplified hypothetical example shows the idea. If one treatment reduces breathing events dramatically but is used only half the time, the patient is untreated for the other half. If another treatment reduces breathing events moderately but is used nearly every night, its total disease relief can come closer than the lab numbers suggest. MDA is not a bedside calculator for every individual; it is a way to avoid the common mistake of treating “works while worn” as the same thing as “works in life.”
That distinction is especially important for people who have already tried CPAP and struggled despite genuine effort. Mask leaks, nasal congestion, claustrophobia, skin irritation, noise, hose positioning, and the simple fatigue of assembling a setup every night can turn a technically excellent therapy into an intermittently used therapy. None of that makes CPAP a bad treatment. It makes adherence part of the treatment, not a character test.
The Response Pattern Is Uneven
The most dangerous version of the oral appliance story is the neat one: smaller, easier, comfortable, therefore effective. The evidence is more uneven. About 70% of mandibular advancement device users achieve at least a 50% reduction in AHI, but outcomes are roughly split into thirds: about one-third reach complete resolution with AHI below 5 events per hour, one-third have a partial response, and one-third have negligible improvement. Those proportions depend on how success is defined, but the pattern is the point: response is real, and response is variable.[1]

This is where follow-up sleep testing protects patients from false reassurance. An appliance can feel comfortable, reduce snoring, and still leave clinically important apnea behind. Snoring improvement is welcome for the household, but it is not the same as proving that oxygen drops, arousals, and breathing-event frequency are controlled.
For someone choosing oral appliance therapy, the practical decision rule is not “try it because it is easier.” It is: use it when the clinical profile makes sense, have it fitted and adjusted properly, and verify the result objectively. The person in the partial-response group may still benefit, especially if symptoms and cardiovascular markers improve, but they should not be silently counted as a complete responder.
Who Is Most Likely to Be a Reasonable Candidate?
Oral appliance therapy is most often considered for adults with mild-to-moderate obstructive sleep apnea, especially when CPAP is not tolerated or when the patient strongly prefers a non-CPAP option after understanding the tradeoff.[1] It may also be discussed when travel, bed-partner issues, or repeated CPAP discomfort make long-term adherence unlikely.
Candidacy is not just an AHI category. A patient needs enough healthy teeth or dental support for the device, the ability to tolerate jaw advancement, and access to follow-up dental care. Temporomandibular joint problems, significant bite concerns, severe dental instability, or inability to return for adjustments may change the risk-benefit calculation.
- More favorable situations: mild-to-moderate obstructive sleep apnea, strong likelihood of nightly wear, CPAP intolerance despite troubleshooting, and willingness to complete follow-up sleep testing.
- More cautious situations: severe sleep apnea, major oxygen desaturation, significant dental or jaw problems, or a need for the most predictable AHI reduction.
- Non-negotiable safeguards: clinical diagnosis, custom fitting, gradual adjustment when needed, dental monitoring, and objective reassessment of sleep apnea control.
Severe obstructive sleep apnea does not automatically rule out every alternative in every real-world circumstance, but it raises the stakes. If breathing events and oxygen drops are substantial, a weaker or unverified response is not a small inconvenience. It can mean leaving disease undertreated.
Pros of Oral Appliance Therapy
The biggest advantage is tolerability that can translate into use. A device that sits in the mouth is often easier to travel with, quieter, and less disruptive than a bedside machine, mask, hose, and power setup. For patients who remove a CPAP mask in frustration after an hour, the practical advantage is not cosmetic.
- Higher observed adherence in objective oral appliance monitoring, including 6.4 to 6.7 hours of nightly wear and 84% to 89% regular use at one year in one microsensor study.[2]
- Comparable improvements to CPAP in blood pressure, sleepiness, and quality-of-life measures in the Phillips randomized trial, despite CPAP’s larger AHI reduction.[3]
- No mask, hose, airflow sensation, or machine noise, which may help patients who struggle with claustrophobia, nasal symptoms, or bed-partner disruption.
- Portability for travel and simpler nightly setup, which can matter for people whose adherence falls apart outside their usual bedroom.
These advantages matter most when they change behavior. If a patient would use CPAP reliably and gets excellent control, the convenience of an oral appliance is not automatically a reason to switch. If the CPAP is sitting unused, the comparison changes.
Cons and Side Effects That Deserve Attention
Short-term side effects are common enough that patients should expect some adjustment rather than interpret every symptom as failure. Jaw soreness, salivation changes, dry mouth, tooth discomfort, and TMJ tenderness can occur early. One systematic review reported jaw soreness in about 65% of new users, and short-term symptoms often improve over weeks as the patient adapts and the device is adjusted.[4]
The longer-term issue is bite change. Mandibular advancement devices place sustained forces on the teeth and jaw over repeated nights. Long-term reviews have reported decreases in overjet of about 0.6 to 2.6 mm and decreases in overbite of about 0.7 to 2.8 mm.[4][5] Those numbers may sound small, but bite changes can be progressive and noticeable to the person chewing with that bite every day.
This is not a reason to frighten every patient away from oral appliance therapy. It is a reason to stop treating the dental follow-up as optional. Regular monitoring can catch tooth movement, bite changes, appliance fit problems, and jaw symptoms early enough to adjust the plan. The patient should know before starting that the mouth is not a passive holder for the device; it is part of the treatment system.
| Risk | What it can feel like | What protects the patient |
|---|---|---|
| Jaw or TMJ soreness | Morning tenderness, tightness, discomfort with advancement | Gradual titration, dental adjustment, symptom review |
| Dry mouth or salivation changes | Dryness, drooling, altered mouth feel | Fit adjustment and time for adaptation |
| Tooth discomfort | Pressure on teeth or gums | Device adjustment and dental assessment |
| Bite changes | Changes in how teeth meet, chewing changes | Long-term dental monitoring |
| Incomplete apnea control | Snoring may improve while AHI remains elevated | Follow-up sleep testing |
Cost Is Real, but Sticker Price Can Mislead
In the United States, custom oral appliance therapy is often estimated around $1,500 to $2,500, while CPAP equipment is often estimated around $300 to $1,200.[6] Those ranges are useful for orientation, but they are not enough to predict what one person will pay.
Insurance coverage, deductibles, prior authorization, medical versus dental billing, in-network providers, replacement schedules, follow-up visits, and required documentation can all change the final burden. Many insurers cover medically prescribed treatment, but “covered” does not always mean inexpensive or simple. A low equipment price can also become less meaningful if the device is abandoned, replaced, or repeatedly troubleshot without consistent use.
How to Know Whether It Is Working
The first clue is often symptom change: less snoring, fewer witnessed apneas, less morning headache, better daytime alertness, or improved bed-partner sleep. Those changes are valuable, but they are not enough. People can feel better and still have residual obstructive sleep apnea. They can also feel tired for reasons unrelated to airway control.
Objective reassessment is the safeguard. After the appliance is fitted and advanced to a tolerable therapeutic position, a follow-up sleep test can show whether AHI, oxygenation, and related measures have improved enough. If the result is incomplete, the options may include further appliance adjustment, combination approaches, renewed CPAP troubleshooting, positional strategies when appropriate, weight-related interventions when relevant, or another clinical plan.
The same standard should apply in the other direction. If a patient is prescribed CPAP but uses it only occasionally, machine-recorded adherence and residual AHI matter. A prescription is not treatment until it is used, and a comfortable device is not treatment until it controls the disease.
A Practical Bottom Line
Oral appliance therapy can be a serious treatment for many adults with mild-to-moderate obstructive sleep apnea. Its best evidence is not that it beats CPAP at lowering AHI on a treated night. It usually does not. Its best evidence is that higher long-term use can narrow the gap in real-world outcomes, a pattern captured by adherence data, the Phillips clinical outcome trial, and the Mean Disease Alleviation framework.[1][2][3]
The tradeoff has to be kept honest. Oral appliances are not automatically effective, not side-effect-free, and not a substitute for diagnosis, proper fitting, dental monitoring, and objective follow-up testing. For the right patient, used consistently and verified objectively, they can work well enough to change the course of sleep apnea treatment. For the wrong patient, or for an untested responder, they can simply make undertreatment feel more comfortable.
References
- Oral Appliances in Obstructive Sleep Apnea. PMC, 2019.
- Objective measurement of compliance during oral appliance therapy for sleep-disordered breathing. Thorax, 2013.
- Health Outcomes of Continuous Positive Airway Pressure versus Oral Appliance Treatment for Obstructive Sleep Apnea: A Randomized Controlled Trial. American Journal of Respiratory and Critical Care Medicine, 2013.
- Occlusal Side Effects of Mandibular Advancement Device Therapy in Adult Patients with Obstructive Sleep Apnea: A Systematic Review. PMC, 2023.
- Long-Term Side Effects of Sleep Apnea Treatment with Oral Appliances: Nature, Magnitude and Predictors of Long-Term Changes. Sleep Medicine, 2019.
- CPAP vs. Oral Appliance. SleepApnea.org.






Comments
Join the discussion with an anonymous comment.