The first useful question is not “Does Ozempic cause insomnia?” It is “How long have you been taking it?” A person in week three with nausea, reflux, a smaller dinner, and a brain that suddenly feels too alert at midnight is in a different situation from someone several months into treatment whose snoring has softened and whose morning headaches have faded.
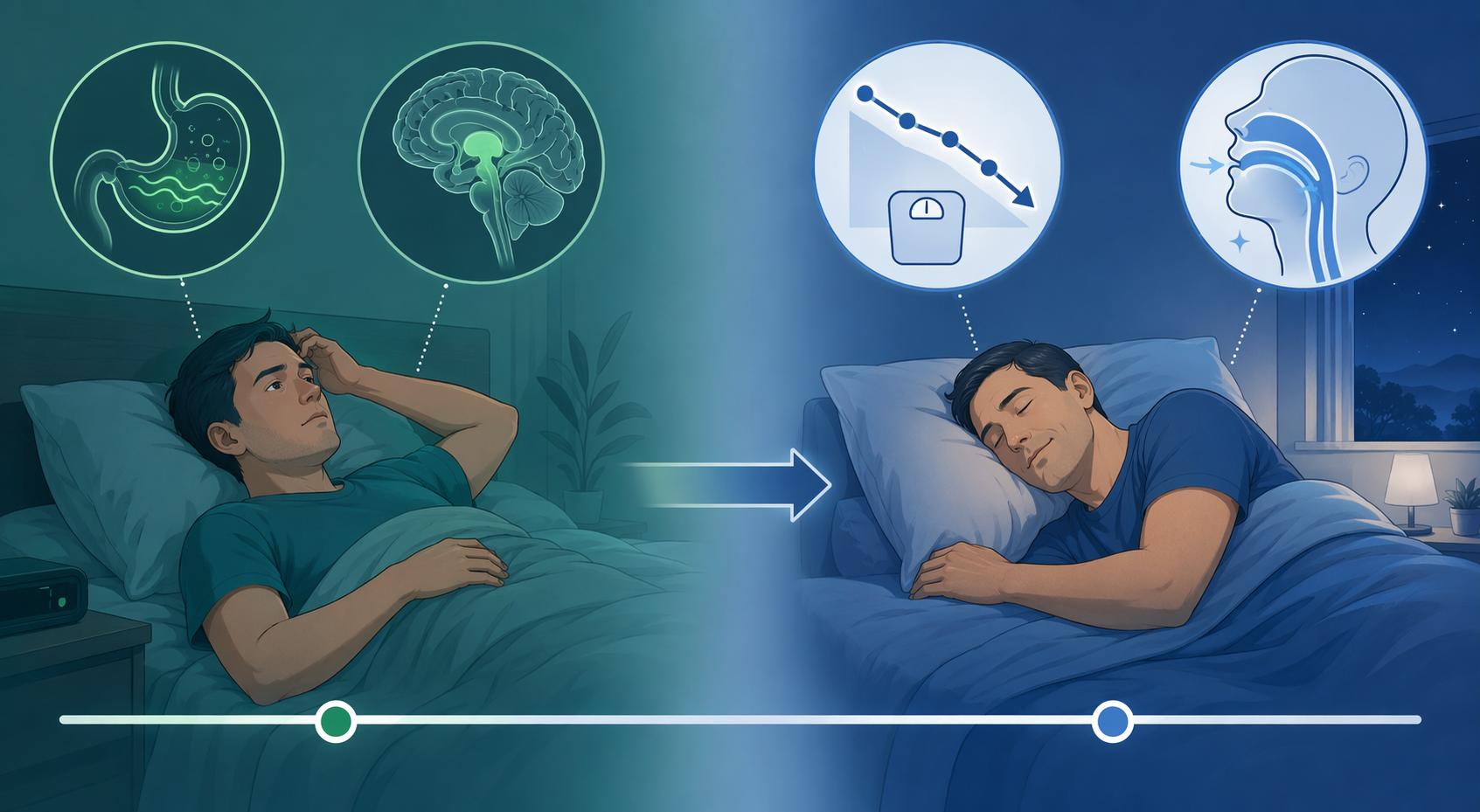
That time course matters because sleep side effects on Ozempic can point in opposite directions. In the first few weeks, GLP-1 medications can disturb sleep through gastrointestinal discomfort, shifting overnight glucose patterns, and possibly direct effects on sleep-wake signaling in the brain. Over months, the same broader treatment pathway can improve sleep for some people by reducing weight-related breathing obstruction, inflammation, and metabolic strain.

The first 2–6 weeks are the noisy phase
Early sleep disruption is often boring in the most clinically useful way: the stomach is not settled. Semaglutide slows gastric emptying. That is part of how it helps with appetite, but it can also mean nausea, fullness, burping, reflux, constipation, or waking with abdominal discomfort. A lighter appetite does not automatically mean a calmer night if dinner sits heavily or reflux starts when the person lies flat.
This is where many internet stories become too dramatic too quickly. A medication can disturb sleep without “ruining” sleep. If someone starts a GLP-1 drug, changes dinner size, eats later because daytime appetite is low, drinks less fluid, has constipation, and wakes at 3 a.m., the drug may be part of the chain. It may not be acting like a classic stimulant.
Blood glucose adaptation can add another layer. Some people eat much less in the evening after starting treatment, or they change carbohydrate intake abruptly. The body may need time to settle into that new overnight pattern. A person can experience lighter, more fragmented sleep while the digestive and metabolic routines are being renegotiated, especially during dose initiation or dose increases.
There is also a more interesting, less settled possibility: GLP-1 activity may affect sleep-wake signaling directly. The leading mechanistic hypothesis is that GLP-1 receptors in sleep-relevant brain regions, including the dorsomedial hypothalamus, may influence orexin, GABA, and melatonin-related signaling. That gives a biological explanation for the “wired but tired” description some patients use. It is plausible, but it should not be treated as proven in the same way as nausea or delayed gastric emptying.
That distinction changes what a person should try first. If the problem is reflux, constipation, or overnight nausea, piling on sedating supplements is usually the wrong target. The better first pass is to move the last substantial meal earlier, avoid high-fat meals close to bed, treat constipation promptly, hydrate consistently, and tell the prescribing clinician if symptoms are escalating rather than settling. Medication-induced insomnia is one of the patterns worth checking before assuming the problem is stress, poor discipline, or a mysterious new sleep disorder; it belongs on the same practical list as the hidden causes of insomnia.
Why the trial picture can look calmer than the patient stories
Large trials are still the place to start when judging whether a drug is a major population-level insomnia trigger. They reduce the risk of mistaking coincidence for causation. Insomnia has been reported at similar rates in semaglutide and placebo groups in large trial summaries, which is a useful reality check before blaming every bad night on the injection. Insomnia is common in adults even without a new medication, and the week someone starts a drug is also often the week they are changing diet, anxiety level, alcohol intake, caffeine timing, exercise, and glucose monitoring. If sleep worsens after the first injection, the timing deserves attention. It does not automatically prove the injection is the only cause.
At the same time, patient reports should not be waved away. A 2023 mixed-methods analysis reviewed 43,710 social media posts about GLP-1 receptor agonists across Reddit, YouTube, and TikTok. It found 620 sleep or insomnia mentions, more than anxiety mentions at 353 and depression mentions at 204, making sleep the most-discussed mental-health theme in that dataset.[1]
That finding does not tell us how often Ozempic causes insomnia. Social media cannot supply a clean denominator, confirm diagnoses, control for dose timing, or separate semaglutide from other GLP-1 drugs with the precision a trial can. What it does show is that enough people are noticing sleep changes to create a real-world signal. Signals are not verdicts. They are reasons to ask better questions.
| If the sleep change started... | The more likely frame | What to check first |
|---|---|---|
| During the first few weeks or after a dose increase | Short-term adaptation or adverse effect | Nausea, reflux, constipation, meal timing, hydration, glucose swings, new anxiety about symptoms |
| After several stable months | Less likely to be simple start-up adaptation | Dose, other medications, mood, caffeine, alcohol, untreated insomnia, sleep apnea symptoms |
| While snoring, gasping, or daytime sleepiness is improving | Possible sleep benefit from weight and metabolic changes | Whether breathing symptoms, morning headaches, and sleep continuity are changing together |
When sleep starts getting better months later
The long-term sleep story is not just “less weight, better sleep,” although that is part of it. Meaningful weight loss can reduce mechanical load around the upper airway, improve breathing stability during sleep, and lower some of the metabolic pressure that keeps the body in a lighter, more reactive state overnight. For people whose poor sleep is partly driven by obstructive sleep apnea, that can be a very different experience from the rocky first month.
The strongest sleep-apnea drug trial data right now should be named carefully. The major phase 3 SURMOUNT-OSA trials were not Ozempic trials. They studied tirzepatide in adults with moderate-to-severe obstructive sleep apnea and obesity. At 52 weeks, tirzepatide reduced the apnea-hypopnea index by as much as 62.8% from baseline.[2]
That result is important because it shows that an incretin-based weight-loss medication can produce clinically meaningful sleep-breathing improvement in the right population. It should not be casually pasted onto semaglutide as if all drugs in the category have identical evidence. Ozempic and Wegovy are semaglutide products; Zepbound and Mounjaro are tirzepatide products. They overlap in the real-world conversation, but the sleep-apnea evidence is not interchangeable.
There is also earlier GLP-1 evidence in sleep apnea. In a 32-week study discussed by the American Academy of Sleep Medicine, liraglutide 3.0 mg reduced apnea-hypopnea index by 12.2 events per hour more than placebo in patients with obesity and moderate obstructive sleep apnea.[3]
For the person living through it, the relevant signs are less abstract than the trial names. Bed partners may notice less snoring or fewer gasping pauses. The person may wake with fewer headaches, need fewer bathroom trips, or stop feeling drugged by sleep after a full night in bed. Women, in particular, can have sleep apnea presentations that are easier to miss, including insomnia, fatigue, mood changes, and morning headaches rather than the classic loud-snoring stereotype; a symptom screen such as the atypical sleep apnea checklist for women can be useful when the story does not fit the usual script.
The same symptom can mean different things depending on timing
Insomnia in week two is usually a management problem until proven otherwise. Insomnia that persists through stable dosing, especially after the gastrointestinal side effects have settled, deserves a more serious review. The question is no longer just “Can I push through?” It becomes “Is this medication unmasking something, interacting with something, or producing a pattern my clinician needs to know about?”
A useful sleep log for this situation is plain and unromantic: dose date, dose amount, bedtime, wake time, nighttime nausea or reflux, constipation, alcohol, caffeine timing, exercise, glucose concerns if relevant, and whether the bad nights cluster after injection day or after dose escalation. Three dramatic nights are hard to interpret. A two-week pattern is much harder to dismiss.
This is also why generic sleep-aid shopping often disappoints. If GLP-1-related sleep disruption is driven by nausea, reflux, constipation, or an alerting neurochemical pathway, then an antihistamine hangover or a large dose of melatonin may add grogginess without fixing the trigger. Evidence-graded sleep supports have their place, but they work best when matched to the problem; a broad review of natural sleep remedies is more useful when the cause has been narrowed first.
The orexin piece is worth special caution. Orexin is one of the brain’s wake-promoting systems, and medications that target orexin are used differently from melatonin-based approaches. That does not mean a person should self-diagnose an orexin problem after starting Ozempic. It does mean that “I took melatonin and it did nothing” is not surprising if the driver is not a simple circadian timing issue. For a deeper comparison, the distinction between suvorexant and melatonin for insomnia helps explain why mechanism matters.
What to do with your own pattern
If the sleep disruption began in the first several weeks, or shortly after a dose increase, start with the modifiable irritants. Eat the last substantial meal earlier. Keep evening fat intake modest if reflux or nausea is present. Do not let daytime appetite suppression turn into accidental under-fueling followed by a strange, restless night. Treat constipation early. Avoid moving caffeine later to compensate for daytime fatigue. Keep exercise in the routine if it is already safe for you, because movement can support sleep through several biological pathways; the exercise-sleep pathways are not magic, but they are reliable enough to matter.
Call the prescribing clinician sooner if insomnia is severe, if you are barely sleeping for multiple nights, if vomiting or dehydration is present, if reflux is intense, if mood symptoms are changing, or if you have diabetes and suspect overnight glucose problems. The answer may be dose timing, dose adjustment, slower titration, symptom treatment, or a different medication. That decision belongs with someone who can see the whole chart.
If sleep is improving after months on treatment, it is reasonable to say that plainly. Some people really do sleep better when weight loss reduces airway obstruction or metabolic strain. That is not a guarantee of sleep apnea resolution, and it is not a reason to abandon CPAP or other prescribed therapy without retesting. It is a reason to tell the sleep clinician what has changed, especially if pressure settings feel different, mask tolerance changes, or daytime sleepiness improves substantially.
The cleanest read is this: early Ozempic sleep disruption is often a short-term adaptation problem, but persistent or severe insomnia should be treated as a real clinical signal. Longer-term sleep improvement is also real for some people, especially when sleep apnea is part of the original problem. The timing does not answer everything, but it tells you which question to ask next.
References
- Exploring Patient Experiences With GLP-1 Receptor Agonists on Social Media: A Mixed Methods Analysis, PubMed Central, 2023.
- Tirzepatide for the Treatment of Obstructive Sleep Apnea and Obesity, New England Journal of Medicine, 2024.
- How weight loss medications are changing the sleep field, American Academy of Sleep Medicine.






Comments
Join the discussion with an anonymous comment.