Yes, the proposed cuts to veterans' sleep apnea benefits would substantially reduce future disability ratings for many veterans with service-connected sleep apnea. The central change is simple enough to state plainly: a CPAP prescription would no longer, by itself, support the familiar 50% rating. Under the proposal, VA would look instead at whether treatment is effective and whether disabling symptoms remain.
That is a real cut. It is also not an immediate across-the-board reduction for every veteran already receiving sleep apnea compensation. Current ratings are supposed to be grandfathered, meaning VA would not automatically lower an existing sleep apnea rating solely because the rating schedule changes. The harder question is what happens to veterans who file new claims, have claims pending, later ask for an increase, or open a new secondary claim after the standard changes.

The Rating Change That Matters
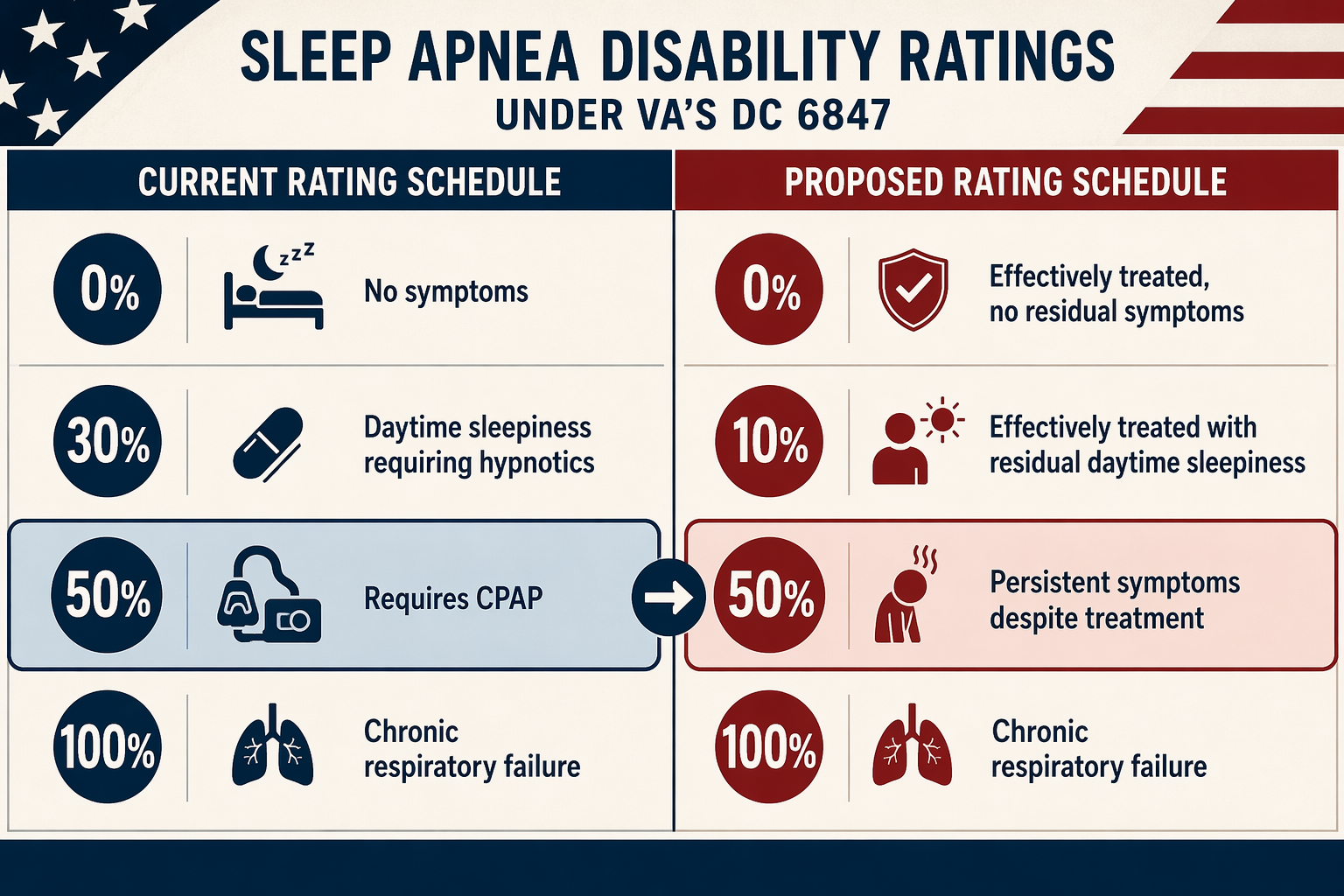
The current sleep apnea rating rule under Diagnostic Code 6847 gives a 50% rating when the condition requires use of a breathing assistance device such as CPAP. The proposed schedule would remove that device-based shortcut. A veteran whose sleep apnea is effectively treated could receive 0% or 10%, depending on residual symptoms; 50% would be reserved for persistent symptoms despite treatment; 100% would remain tied to chronic respiratory failure or similarly severe complications.[1]
| Rating | Current DC 6847 framework | Proposed framework |
|---|---|---|
| 0% | No symptoms | Effectively treated, with no residual symptoms |
| 10% | No separate 10% level for sleep apnea | Effectively treated, but with residual daytime sleepiness |
| 30% | Daytime sleepiness requiring hypnotics | No 30% level in the proposed sleep apnea framework |
| 50% | Requires CPAP or another breathing assistance device | Persistent symptoms despite treatment |
| 100% | Chronic respiratory failure | Chronic respiratory failure |
The financial consequence sits in the 50% line. Under the current schedule, the prescribed treatment can carry the rating. Under the proposed schedule, the result of treatment becomes the decisive fact. If CPAP works well enough that VA finds no residual symptoms, the rating could fall to 0% for a future claimant. If CPAP works but daytime sleepiness remains, the proposed rating could be 10%. The same diagnosis and the same machine can lead to a much lower award if the agency treats the condition as effectively controlled.
That is why describing the proposal as a modernization misses the point for veterans making filing decisions. The cut is not hidden in the diagnosis. It is hidden in the verb: requires becomes effectively treated. A veteran can still have service-connected sleep apnea, still use CPAP every night, and still be rated far below 50% under the proposed standard if VA concludes the treatment controls the condition.
Who Is Exposed, And Who Is Not
For veterans already rated for sleep apnea, the most important protection is also the easiest one to lose in the noise: VA cannot reduce an existing rating solely because the rating schedule later changes. Reporting on the proposal has described current ratings as grandfathered, with the caveat that the outer edges of that protection are not fully tested for later claims activity.[2]
That does not mean every future interaction with VA is risk-free. It means the schedule change alone should not trigger an automatic reduction. The practical difference matters.
| Veteran's situation | Likely practical effect if the proposal takes effect |
|---|---|
| Already rated for sleep apnea | Existing rating should not be automatically reduced solely because the schedule changes. |
| New sleep apnea claim filed after the change | The claim would likely be evaluated under the new treatment-effectiveness standard. |
| Claim pending when the change takes effect | The applicable standard may depend on effective-date and transition rules; this is a place to watch closely. |
| Later request for an increase | The veteran may face review under the new criteria, especially if VA is asked to reassess severity. |
| New secondary claim connected to sleep apnea | The original rating may be protected from schedule-change reduction, but the new claim could create review questions that are not fully settled. |
A veteran with a long-standing 50% sleep apnea rating should not read every headline as a notice that next month's payment is about to drop. But a veteran who has a diagnosis, a CPAP prescription, and has not yet filed has a different problem. If the new rule takes effect before the claim is decided, the old assumption that CPAP equals 50% may no longer hold.
The same caution applies to an increase. A veteran who is already rated may have legitimate reasons to seek a higher evaluation or to file for a related condition. But the point of grandfathering is narrow: it protects an existing rating from being lowered just because the table changed. It does not necessarily promise that every later filing will be insulated from the new criteria. That boundary is exactly where veterans should avoid taking advice from a headline.
How Many Veterans And How Much Money
The scale is large. DAV said 763,000 current sleep apnea claimants are on the rolls and cited a VA analysis projecting $57 billion in reduced disability payments over ten years, affecting up to 1.5 million veterans.[3] Those figures have also been central to the backlash from veterans' organizations and lawmakers. They should be read carefully: the $57 billion estimate comes from a VA analysis cited by DAV and other opponents, not from a publicly available Congressional Budget Office score of the full package as of July 19, 2026.
The 763,000 figure is also not the whole universe of concern. It describes current sleep apnea claimants on the rolls. It does not capture every veteran with an undiagnosed condition, every veteran preparing a claim, or every claim already somewhere in the adjudication pipeline. That is why the grandfathering distinction cannot be treated as a footnote. The proposal protects one group from an automatic schedule-change reduction while changing the rules for the next group trying to get in.
The Bill Is One Track; VA Rulemaking Is Another
The legislative vehicle is H.R. 9237, the Take Care of America's Veterans Act. Section 108 was written as the PAYGO offset for the Major Richard Star Act, using reductions to sleep apnea and tinnitus benefits to pay for the broader package. Ranking Member Mark Takano called that provision “the largest betrayal of veterans in a single legislative act in modern history.”[4]
The House did not vote on the bill before the July recess. It was pulled from the House floor twice, first on June 25 and again on July 16, 2026, after backlash over the sleep apnea and tinnitus cuts. Speaker Mike Johnson indicated the bill may return in September 2026.[5]
That pause does not end the issue. A parallel VA rulemaking to revise disability rating criteria for sleep apnea and tinnitus has been paused but not withdrawn. If Congress drops the offset but VA later finalizes a similar rule, future claimants could still face the same basic shift from device-based rating to treatment-effectiveness rating.
This is one reason the status of the bill alone is not enough. Veterans need to track both tracks: the legislation and the agency rulemaking. One can stall while the other remains available.
Why The Backlash Became So Sharp
Opposition hardened because the sleep apnea provision was not standing alone as a technical edit. It was paired with tinnitus cuts and used as an offset inside a veterans bill that otherwise included benefits many veterans' advocates support. Forty-seven Senate Democrats sent a letter to VA Secretary Doug Collins opposing the disability rule changes and citing his confirmation pledge.[6]
DAV, VFW, and Iraq and Afghanistan Veterans of America all formally opposed the cuts. IAVA warned, “Today it's just tinnitus and sleep apnea. Tomorrow, will it be PTSD?”[3][7] The quote is advocacy language, not a prediction that PTSD cuts are already written into this bill. Its force comes from the precedent concern: once common service-connected conditions are treated as budget offsets, veterans' groups expect the next eligibility fight to come quickly.
Tinnitus matters here because it explains part of the political intensity. It is the most common service-connected disability, with 3.6 million recipients, and the same controversy would remove its standalone rating under the bill.[5] But the sleep apnea issue should not be blurred into tinnitus. For sleep apnea, the concrete loss is the end of the automatic 50% rating tied to CPAP use.
What Veterans Should Treat As Unsettled
The first unsettled point is timing. As of July 19, 2026, the bill is shelved, not dead. It may return in September. The VA rulemaking is paused, not withdrawn. Anyone deciding whether to file a new sleep apnea claim, seek an increase, or connect another condition secondarily to sleep apnea should make that decision with the current procedural status in mind, not with the assumption that the proposal has disappeared.
The second unsettled point is transition treatment for pending claims. Grandfathering is clearest for existing ratings. It is less comforting for claims that are not yet granted or for later filings that invite VA to evaluate the condition under a new table. The exact boundary will depend on the final language, effective dates, and how VA applies the rule once it is live.
The third unsettled point is scoring. The projected $57 billion reduction is serious, but the available figure comes from a VA analysis cited by advocacy groups, not a public CBO score of the full bill package. That does not make the number meaningless. It does mean readers should know what kind of estimate they are looking at.
The safest reading is bounded but blunt: this is not an immediate mass reduction for everyone already compensated for sleep apnea, and it is not harmless administrative cleanup. It is a serious proposed narrowing of future compensation. The veteran most exposed is the one whose entitlement depends on the current rule that CPAP use supports 50%, but whose claim or later review would be decided under a new rule asking whether treatment is effective enough to justify far less.
References
- VA Is Rewriting Big Pieces of the Disability Rating Playbook, Military.com, February 15, 2026
- As opposition mounts, House cancels vote on VA overhaul bill, Government Executive, June 2026
- DAV condemns congressional proposal to cut disability benefits for 1.5 million veterans, DAV, 2026
- Ranking Member Takano Warns Against Republican Bid to Strip Veterans of Their Disability Benefits, House Committee on Veterans' Affairs Democrats
- Vets bill shelved after backlash against sleep apnea, tinnitus cuts, UPI.com, July 16, 2026
- 47 Senate Lawmakers Oppose VA Disability Rule on Sleep Apnea, Tinnitus, Military.com
- VFW Action Alert: Tell Congress to Oppose Veterans Benefit Cuts, VFW, June 2026






Comments
Join the discussion with an anonymous comment.