The maddening version of insomnia is not always lying awake at bedtime. Many people with sleep maintenance insomnia fall asleep without much drama, sleep for a few hours, then wake around 3 a.m. with a body that feels finished sleeping and a mind that is suddenly available for every problem it avoided during the day.
That pattern matters because it points to a different treatment question than trouble falling asleep. Sleep onset insomnia asks, in part, why sleep will not start. Sleep maintenance insomnia asks why sleep will not hold. Clinical descriptions of insomnia include difficulty initiating sleep, difficulty maintaining sleep, waking too early, or nonrestorative sleep despite adequate opportunity; the subtype changes what should be investigated first.[1]
If you want a fuller comparison of the two patterns, start with trouble falling asleep vs. staying asleep. The short version is this: waking after several hours is not proof that you failed at sleep hygiene. In many cases, the more useful question is whether your sleep pressure has already been spent.
Why the second half of the night is easier to lose
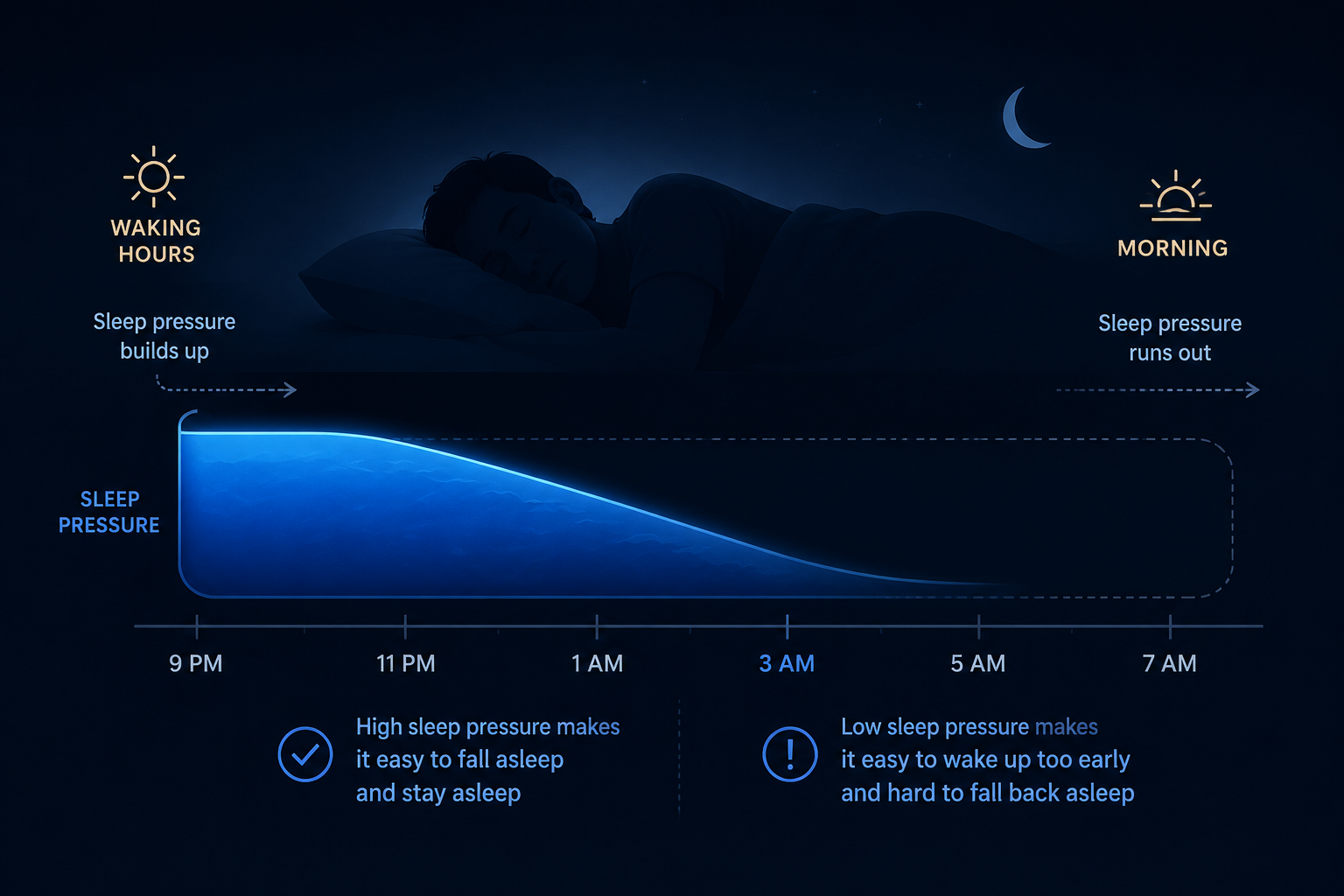
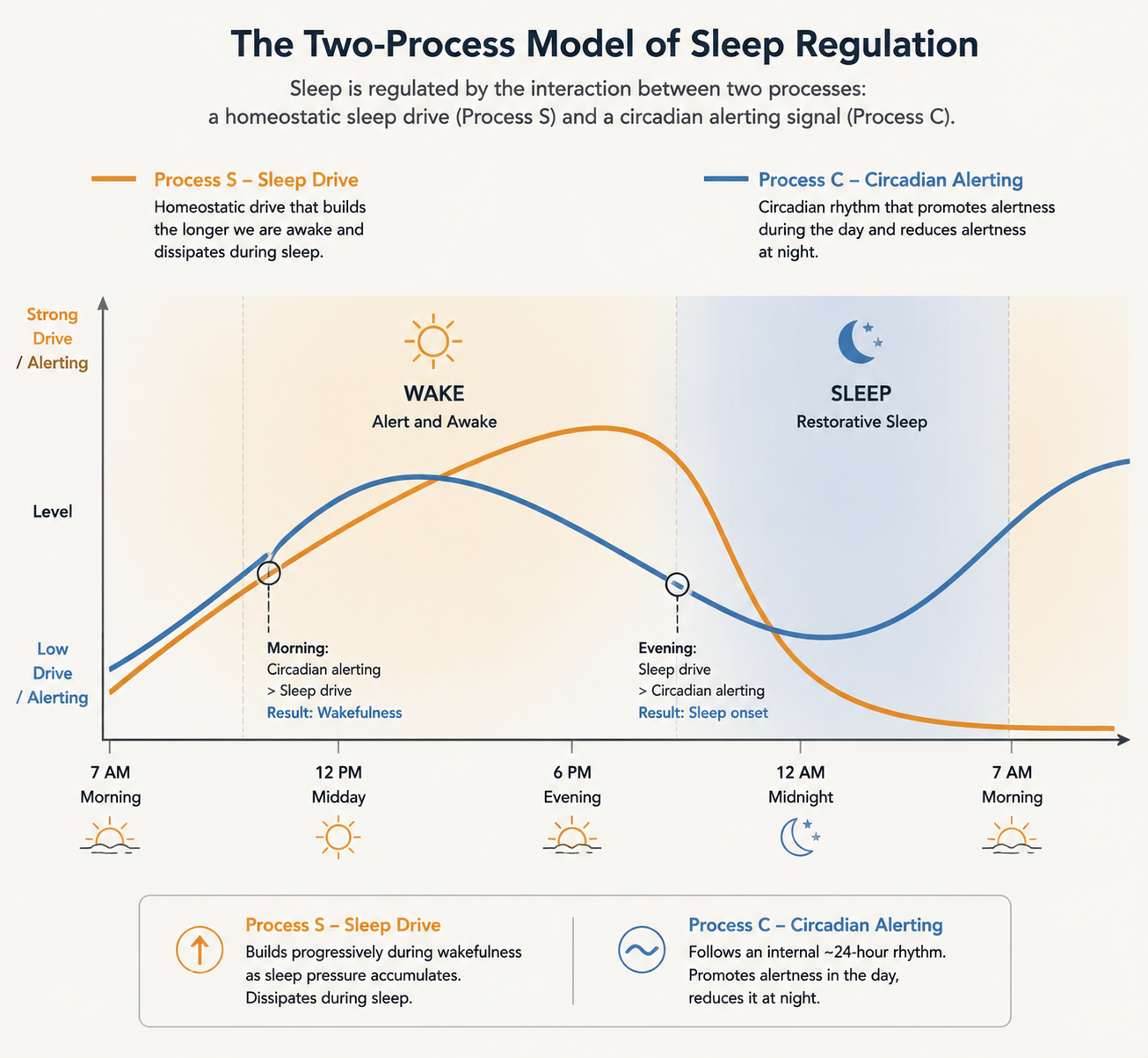
Sleep is regulated partly by homeostatic sleep drive: the pressure to sleep that builds while you are awake and fades as you sleep. It is also shaped by the circadian alerting signal, the body’s roughly 24-hour rhythm that makes sleep more or less biologically likely at different times. This is often called the two-process model of sleep regulation; the practical point is that sleep continuity depends on both enough pressure to sleep and the right biological timing.[2]
At the beginning of the night, sleep pressure is usually high. After several hours of sleep, it is lower by design. That is not a defect; it is how the system works. The problem begins when the pressure available at bedtime is not strong enough to carry the whole night. Cleveland Clinic’s explanation of sleep maintenance insomnia names this plainly: the sleep drive can be depleted, leaving a person more vulnerable to waking and staying awake in the early morning hours.[2]
This is where the usual advice can feel almost insulting. A cool room, lower light, and a calmer evening may help some people, but they do not explain why someone who did “everything right” still wakes after four or five hours. If the back half of the night is running on too little sleep pressure, the missing piece is not another lavender ritual. It is a mismatch between time in bed and the body’s current ability to sustain sleep.
The reasonable choices that can spend sleep pressure too early
The cruel part is that many sleep-drive problems begin with choices that make sense when you are exhausted. You wake at 3 a.m., drag yourself through work, and decide to go to bed earlier. The next day you nap because your body feels desperate. By the weekend, sleeping in seems like the only humane option. Each move can feel like recovery. Each one can also reduce the pressure that would otherwise help hold sleep together the next night.
Going to bed too early is the most common trap. If your body is currently producing six hours of sleep but you give it nine hours in bed, the night has too much space in it. You may fall asleep at first because you are tired, but once the first block of sleep discharges the strongest pressure, the remaining hours can become fragile. The wake-up then looks mysterious: you did not stay up late, you were not reckless, and yet the night split open.
Napping can create the same problem from the other side. A nap may be necessary for safety or basic functioning, especially after a brutal night, but it is not free from a sleep-drive perspective. It spends some of the pressure that would otherwise accumulate for nighttime sleep. For someone whose main problem is the second half of the night, that borrowed relief can show up later as another early-morning awakening.
Sleeping in on weekends can also backfire. It may repay some acute exhaustion, but it can delay the day’s sleep-drive buildup and blur the timing signal that helps the next night land. This is one reason a Sunday “catch-up” sleep can be followed by a Monday night that feels strangely thin.
Afternoon caffeine belongs in this picture too, although it works differently. It does not create sleep pressure; it blocks some of the felt sleepiness that pressure would normally produce. For some people, that makes the first half of the night lighter or delays sleep enough to scramble the next day’s compensation cycle. The point is not that every cup of coffee causes 3 a.m. waking. The point is that the whole 24-hour pattern matters when the complaint is staying asleep.
For a deeper explanation of this same mechanism, the two-system sleep guide walks through the interaction between sleep drive and circadian rhythm. The important distinction here is that “tired” and “ready to stay asleep” are not always the same thing.
How common is this pattern?
Sleep maintenance insomnia is not rare. Cleveland Clinic describes it as affecting about 1 in 5 people, citing NIH data, though that figure is best treated as a reasonable clinical estimate rather than a fresh, subtype-specific population count.[2] Broader insomnia numbers are easier to find: an American Academy of Sleep Medicine survey reported that 12% of Americans said they had been diagnosed with chronic insomnia.[3]
Those numbers are useful mainly for one purpose: they should lower the shame. They do not prove that your particular 3 a.m. awakening has one cause. They do show that trouble maintaining sleep is common enough to deserve a targeted explanation instead of another lecture about discipline.
Why sleep restriction therapy matches the mechanism
The treatment that most directly targets depleted sleep pressure is sleep restriction therapy, usually delivered as one component of cognitive behavioral therapy for insomnia, or CBT-I. The name is unfortunate. It sounds punitive, as if the goal is to deprive an already exhausted person of more sleep. The actual goal is narrower and more rational: temporarily reduce time in bed so the body relearns to associate the sleep window with consolidated sleep.
A CBT-I primer describes sleep restriction as a titrated protocol: time in bed is initially compressed, then adjusted based on sleep efficiency, the percentage of time in bed actually spent asleep. In that protocol, sleep efficiency below 85% leads to further restriction, sleep efficiency above 90% leads to expansion, and efficiency between those thresholds generally holds the schedule steady.[4]
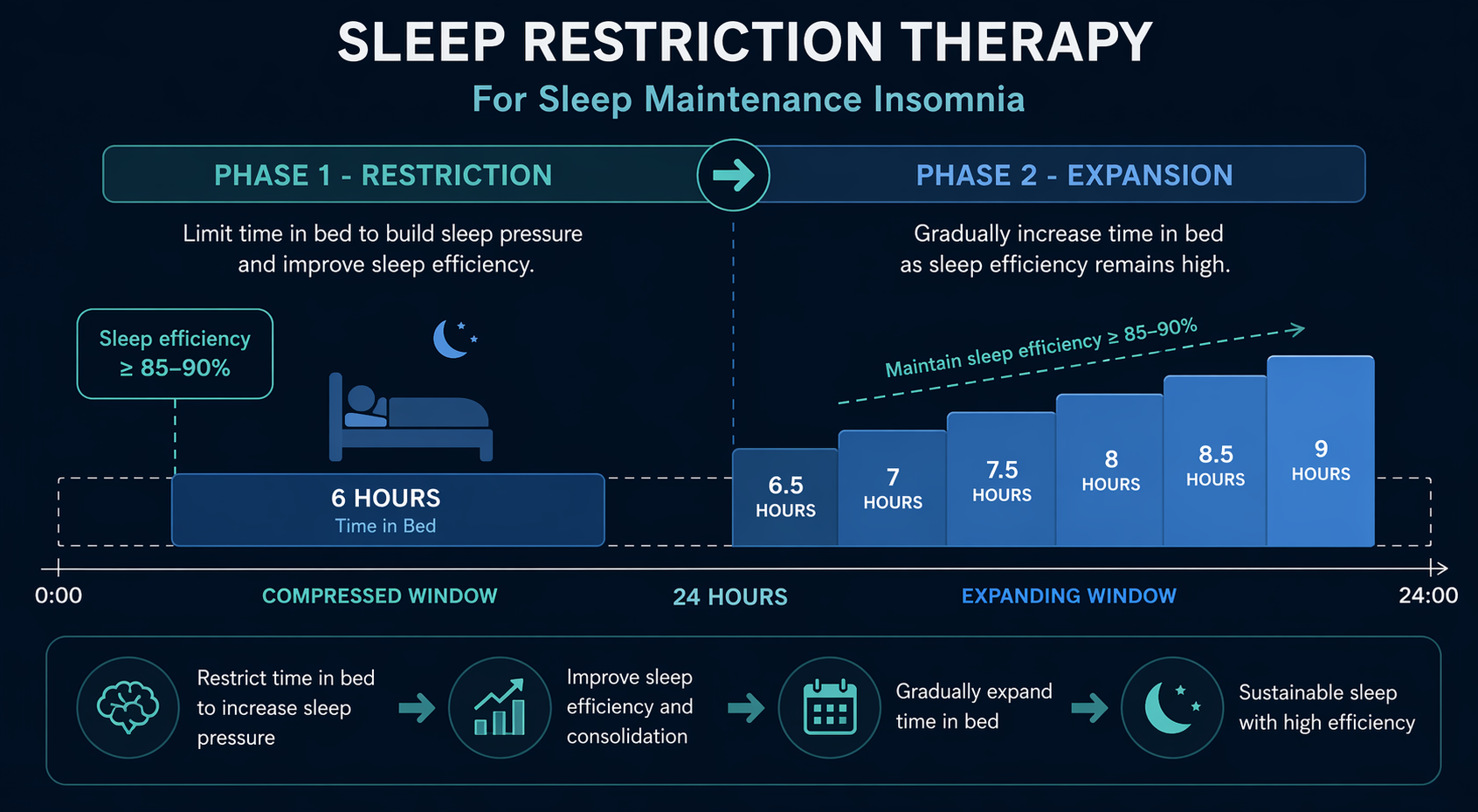
That is the mechanical elegance of the approach. If the problem is too much time in bed for the amount of sleep pressure available, sleep restriction does not ask you to decorate the bedroom differently. It changes the sleep opportunity. The first target is not a perfect eight-hour night; it is a tighter, more reliable sleep window. Only after the window becomes efficient does the schedule expand.
This early phase can feel rough. Daytime sleepiness may increase during the first week or two, which is one reason sleep restriction is often safer and more tolerable when guided by a clinician, especially for people who drive long distances, operate machinery, have bipolar disorder, seizure risk, or other medical concerns. Early sleepiness does not automatically mean the treatment is failing. It may mean the protocol is finally rebuilding the pressure that scattered sleep had been draining.
CBT-I has stronger evidence than ordinary sleep hygiene advice. The CBT-I primer reports meta-analytic evidence of roughly 50% symptom reduction, with gains maintained for up to 24 months.[4] Sleep Foundation also summarizes evidence that as many as 70% to 80% of people with primary insomnia improve with multicomponent CBT-I.[5] These figures should not be read as a guarantee for every sleeper, but they do justify treating CBT-I as a serious first-line approach rather than a wellness accessory.
For readers who want the broader treatment frame, why sleep hygiene alone is not enough explains how CBT-I combines behavioral and cognitive tools. For readers considering a structured self-guided route, a self-directed CBT-I walkthrough can help clarify what belongs in a real program and what is just repackaged sleep hygiene.
What this looks like in practice
A sleep restriction plan usually starts with a sleep diary, not a guess. The diary estimates how much sleep you are actually getting, when awakenings occur, and how much time you are spending awake in bed. From there, the sleep window is set to better match actual sleep time, then adjusted as efficiency changes. The most consequential part is often the fixed wake time. Without it, sleep pressure does not build predictably the next day.
| Part of the plan | What it is doing |
|---|---|
| Sleep diary | Separates actual sleep time from time spent hoping to sleep |
| Compressed sleep window | Raises sleep pressure by reducing excess time in bed |
| Fixed wake time | Anchors the next day’s sleep-drive buildup and circadian timing |
| Efficiency-based adjustment | Expands the window only when sleep becomes more consolidated |
This is also why casually “trying sleep restriction” without a plan can go badly. If the window is too aggressive, daytime impairment can become unsafe. If the wake time keeps moving, the pressure-building effect weakens. If naps are added back whenever the day feels hard, the intervention may never get a clean test.
The 15- to 20-minute rule is not about willpower
Sleep restriction is often paired with stimulus control therapy, another CBT-I component. In Bootzin’s stimulus control protocol, a person who cannot fall asleep after about 15 to 20 minutes is instructed to get out of bed, return only when sleepy, use the bed only for sleep and sex, wake at the same time each morning, and avoid naps.[4]
For sleep maintenance insomnia, this rule can be emotionally difficult because it asks you to leave bed at the exact hour when you most want rescue. But the logic is not moral. It is conditioning. If bed becomes the place where you rehearse being awake, frustrated, and vigilant, the room itself starts to participate in the insomnia. Getting up interrupts that training.
The move should be boring, dim, and brief enough to preserve the night. You are not starting your day at 3 a.m.; you are refusing to turn the bed into an arena. A detailed guide to stimulus control therapy is useful if this rule sounds simple on paper and miserable in real life.
When 3 a.m. waking is not mainly a sleep-drive problem
The sleep-drive explanation is useful, but it is not universal. Middle-of-the-night waking can be pushed by snoring or gasping, sleep apnea, frequent urination, pain, reflux, hot flashes, perimenopause-related hormonal changes, depressed mood, anxiety, restless legs symptoms, periodic limb movements, medications, alcohol, or other medical conditions. A behavioral sleep-pressure plan will not fix every driver on that list.
- If you wake choking, gasping, or with witnessed pauses in breathing, the sleep apnea question comes before a pure CBT-I explanation.
- If you wake repeatedly to urinate, the cause may involve fluid timing, medications, bladder symptoms, metabolic issues, or other medical factors.
- If hot flashes or cycle changes are part of the pattern, perimenopause-related waking deserves its own explanation.
- If early-morning waking comes with persistent low mood, loss of interest, or hopelessness, depression should be assessed directly.
This is not a reason to abandon the sleep-drive model. It is a reason to use it carefully. The guide to hidden causes of insomnia is the better next stop when the awakenings come with physical symptoms, and the piece on perimenopause and sleep disruption is more specific when night waking clusters around hormonal transition.
The question to ask before adding another bedtime habit
If your main problem is falling asleep, the first treatment question may be about timing, arousal, circadian delay, or conditioned wakefulness at bedtime. If your main problem is waking after several hours and being unable to return to sleep, the question shifts: is your time in bed larger than your current sleep drive can support?
That question is less blameful and more testable. It explains why going to bed earlier can worsen the problem, why naps can feel necessary and still interfere with consolidation, and why sleeping in may not repair the next night. It also explains why sleep restriction therapy, done carefully, can be more mechanism-matched than another generic checklist.
For someone waking at 3 a.m. without clear medical red flags, the next serious step is not to search for the one missing bedtime habit. It is to evaluate whether a structured CBT-I approach can rebuild enough sleep pressure to carry the night.
References
- Chronic Insomnia. StatPearls / NCBI Bookshelf.
- 3 Steps for Managing Sleep Maintenance Insomnia. Cleveland Clinic.
- Survey Shows That 12% of Americans Have Been Diagnosed With Chronic Insomnia. American Academy of Sleep Medicine.
- Cognitive Behavioral Therapy for Insomnia (CBT-I): A Primer. PMC / NIH.
- Cognitive Behavioral Therapy for Insomnia (CBT-I): How It Works. Sleep Foundation.






Comments
Join the discussion with an anonymous comment.