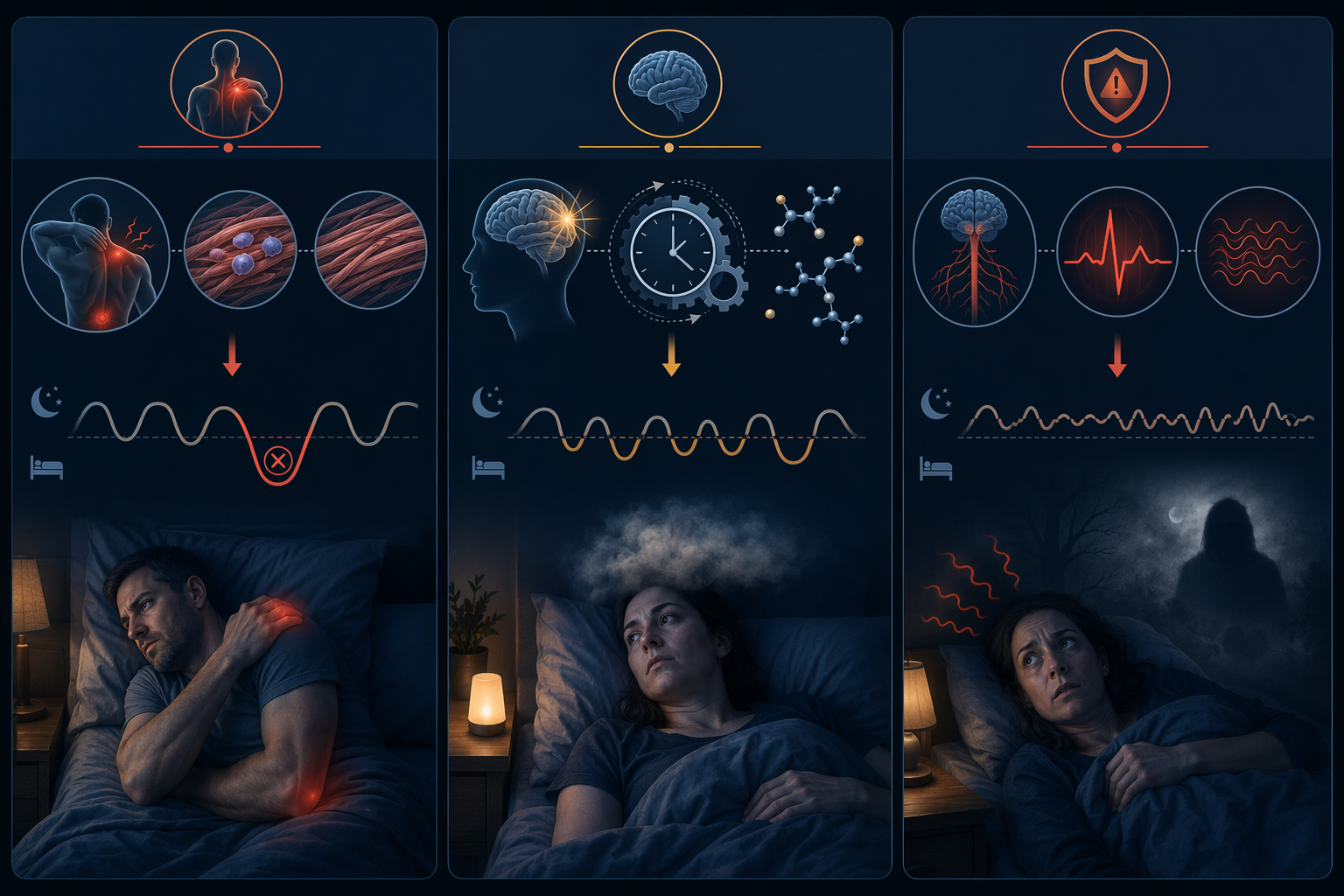
Poor sleep after an accident can come from pain, a concussion or traumatic brain injury, psychological trauma, or more than one of these at once. That distinction matters. The person who wakes every time a bruised rib pulls is dealing with a different sleep problem than the person whose brain no longer keeps a steady sleep-wake rhythm, and both are different from the person whose body goes on alert the moment the bedroom gets quiet.
So the first useful question in sleep recovery after an accident is not “How do I sleep better?” It is: which system is keeping sleep from happening — the injured body, the sleep-regulating brain, the threat-response system, or some combination?

The three-pathway framework below is an organizing tool, not a diagnosis. It is built from separate pain, concussion/TBI, and trauma literatures rather than from one unified clinical classification. It can help you decide what kind of help to seek and which advice is likely to be too generic.
A quick way to separate the three pathways
| Pathway | What tends to keep you awake | Clues that it may be dominant | Better-matched next step |
|---|---|---|---|
| Pain and physical injury | Aching, throbbing, stiffness, positional pain, inflammation | Sleep breaks when you move; one position is tolerable and others are not; pain feels worse after short sleep | Medical injury care, pain management, positioning support, and basic sleep stability |
| Concussion or TBI effects | Disrupted sleep regulation, circadian rhythm changes, daytime fatigue, altered melatonin signaling | Headache, dizziness, light sensitivity, fogginess, new insomnia or excessive sleepiness after head impact or whiplash-type force | Concussion-specific recovery guidance and clinical evaluation if symptoms persist or worsen |
| Trauma and threat response | Hyperarousal, nightmares, intrusive memories, fear of sleep, avoidance of reminders | Your body feels unsafe at night even when the injury pain is manageable; sleep is interrupted by panic, dreams, or scanning for danger | CBT-I, trauma-informed care, and treatment that addresses arousal rather than ordinary sleep habits alone |
These categories overlap. A fall can injure a shoulder, involve a head strike, and leave the person afraid of slipping again. A car crash can cause neck pain, concussion symptoms, and nighttime hypervigilance when headlights pass the window. The point is not to pick a perfect label; it is to identify the pathway doing the most damage right now.
Pathway 1: pain turns sleep into a broken repair window
Pain-related insomnia after an accident often looks deceptively simple: you are tired, but your body will not let you stay still long enough to sleep. A sore shoulder complains when you roll over. A strained back tolerates one position until it does not. A bruised rib makes deep breathing feel like a negotiation.
This is not just discomfort layered on top of recovery. Deep non-REM sleep is one of the periods when injured tissue gets more favorable repair conditions. OrthoCarolina describes increased muscle blood flow during deep NREM sleep, carrying oxygen and nutrients needed for tissue repair; it also notes that the pituitary gland releases growth hormone during slow-wave sleep, supporting muscle repair, and that sleep deprivation reduces that secretion.[1]
Inflammation belongs in the same loop. Prolactin, a hormone involved in regulating inflammation, is released during sleep, and insufficient sleep is associated with increased inflammation and prolonged recovery in OrthoCarolina’s injury-recovery summary.[1] That does not mean one bad night ruins healing. It means repeated pain-fragmented nights can make the body’s repair work less efficient at the same time that pain makes sleep harder to sustain.
There is another practical problem: sleep loss can lower pain tolerance. Concussion Alliance summarizes evidence that sleep deprivation reduces pain tolerance, which creates a bidirectional spiral — pain wakes you, shorter sleep makes pain harder to tolerate, and the next night starts with a more reactive body.[2]
When this pathway is dominant, the most revealing detail is timing. If you fall asleep but wake whenever the injured area is loaded, stretched, bumped, or unsupported, the sleep problem may be downstream of injury management. Generic bedtime advice can still help at the edges, but it will not solve a mechanical pain trigger. The practical target is to reduce the awakenings caused by pain: appropriate medical follow-up, safer sleep positioning, prescribed or clinician-approved pain control, and avoiding the cycle of spending the whole night bracing.
Baseline routines still matter, especially when recovery has made the day irregular. A stable wake time, lower evening stimulation, and a bedroom that does not make pain worse can support all three pathways. If you need a plain foundation before adding pathway-specific care, start with sleep hygiene fundamentals and an evidence-based bedtime routine. Just do not mistake hygiene for treatment when pain is repeatedly breaking sleep.
Pathway 2: concussion can disturb the sleep-regulation system itself
Concussion-related sleep disruption can be confusing because it may not feel like “pain keeping me awake.” A person may be exhausted but wired, sleepy during the day but restless at night, or suddenly unable to keep the schedule they had before the accident. This pathway becomes more likely when poor sleep arrives with headache, dizziness, nausea, light or noise sensitivity, blurred concentration, mental fog, mood shifts, or a clear head impact. It can also follow forces that jolt the head and neck even when the accident does not look dramatic from the outside.
The prevalence figures are broad, but they are large enough to take seriously. A 2016 review reported that sleep disturbances affect 30% to 70% of people after traumatic brain injury; the review’s underlying studies ranged from 2001 to 2015, so the estimate is best read as a comprehensive older range rather than a fresh point estimate.[3] Concussion Alliance summarizes additional research reporting that about 50% of TBI patients endorse insomnia symptoms and that 40% to 65% of concussion patients report insomnia.[2]
Mechanism matters here. Concussion Alliance describes concussion-related damage or disruption in hypothalamic regions involved in sleep regulation, along with changes in melatonin production and circadian rhythms.[2] The 2016 review also discusses disruption in sleep-wake regulation after TBI.[3] That helps explain why the advice to “just rest” can feel maddening. The system that organizes rest may itself be irritated or dysregulated.
The earliest days deserve special caution. Concussion Alliance notes research linking poor sleep in the first 10 days after concussion with increased risk of persisting symptoms.[2] That does not give a universal timeline for sleep recovery after every accident; no single peer-reviewed study tracks one unified recovery timeline across all injury types. It does mean that sleep disruption soon after a suspected concussion is not a minor side issue to ignore.
Napping is one place where concussion advice differs from ordinary insomnia advice. After the first few days, excessive daytime sleep can further confuse circadian timing. Concussion Alliance and CDC-aligned guidance advise limiting daytime naps after day 3 post-concussion to avoid worsening circadian disruption.[2][4] That is not the same as forcing yourself through severe symptoms; it is a reason to use concussion-specific guidance rather than borrowing general sleep tips.
If this pathway fits, move toward a concussion recovery plan instead of treating the problem as ordinary insomnia. The more detailed next step is how to rebuild sleep quality during concussion recovery, especially if your sleep timing, daytime fatigue, and cognitive symptoms changed together.
Pathway 3: trauma keeps the body on watch
Trauma-related sleep disruption has a different texture. The injured body may be healing, and concussion symptoms may be absent or improving, but the nervous system behaves as if danger is still nearby. The bedroom gets quiet, and the mind starts replaying impact, sirens, the fall, the sound of metal, the moment before contact, or the fear of losing control again.
The VA National Center for PTSD reports that 70% of people with PTSD have insomnia, and it identifies sleep disturbances as among the most common post-trauma symptoms.[5] That figure does not mean every accident survivor with insomnia has PTSD. It does mean that when trauma symptoms are present, sleep problems should not be waved away as ordinary stress.
Three patterns are especially important: hyperarousal, nightmares, and avoidance. Hyperarousal is the body staying prepared for threat — faster heart rate, muscle tension, scanning sounds, startling awake, or feeling unsafe when nothing visible is happening. Nightmares can make sleep itself feel risky. Avoidance may look reasonable from the outside: delaying bedtime, sleeping with lights on, staying on the couch, drinking to blunt arousal, or refusing to drive past the accident location. The short-term goal is relief; the long-term effect can be that sleep becomes another reminder to escape.
A small but often-cited Zurich study found that participants who slept within 24 hours after watching a traumatic film had fewer intrusive memories than those who stayed awake.[6] The caveat is essential: watching a traumatic film is not the same as surviving an accident. The study is suggestive for thinking about sleep and emotional memory, not a rule that can be directly applied to real-world trauma recovery.
When trauma is the dominant pathway, treating the problem as a simple bedtime-routine failure can backfire. The VA recommends cognitive behavioral therapy for insomnia, or CBT-I, as a first-line treatment for sleep problems in PTSD rather than defaulting first to medication.[5] If you are trying to understand why CBT-I is more than “sleep hygiene,” read what actually cures insomnia? CBT-I explained.
The same arousal system can show up after other threats that make the environment feel unsafe. For a parallel example, how hurricane anxiety disrupts sleep at every phase describes a different situation with a similar sleep mechanism: the body stays on alert because it is still listening for danger.
The hard cases are usually mixed
Many people do not fit cleanly into one pathway. A neck injury can fragment sleep, the resulting sleep loss can lower pain tolerance, and the worse pain can make the next night more fragmented. A concussion can disrupt circadian rhythm, and poor sleep can make emotional regulation harder. Trauma can increase muscle tension, which can aggravate pain. Pain can make a person feel trapped in the body at night, which can feed panic.
That is why the same sleep tip can help one accident survivor and fail another. “Go to bed at the same time” may be useful when the main issue is schedule drift. It is not enough when a rib injury wakes you every time you turn, when concussion has shifted your sleep-wake rhythm, or when closing your eyes triggers accident replays.
A better self-check is to ask what happens at the moment sleep fails:
- If pain wakes you from sleep or prevents comfortable positioning, start with injury care and the pain-sleep spiral.
- If your sleep timing changed along with headache, dizziness, fogginess, light sensitivity, or unusual daytime sleepiness, consider the concussion/TBI pathway.
- If your body becomes alert, panicky, watchful, avoidant, or nightmare-prone around sleep, consider the trauma pathway.
- If two or three are present, do not force a single explanation; treat the most urgent or disruptive pathway first while watching the others.
This also explains why supplements are such an incomplete answer. Some people consider melatonin, magnesium, herbal products, or over-the-counter sleep aids after an accident. Safety depends on the injury, medications, concussion status, alcohol use, and medical history. If you are comparing options, use an evidence-tiered guide such as which home remedies for insomnia actually have scientific backing? and check with a clinician when head injury, severe pain, pregnancy, other sedating medications, or mental health symptoms are involved.
When to stop self-triage and get evaluated
Self-triage is useful only up to a point. Seek urgent medical care after an accident if there are red-flag symptoms such as worsening headache, repeated vomiting, seizure, weakness, confusion, loss of consciousness, severe or worsening pain, trouble breathing, chest pain, new neurological symptoms, or any concern that an injury has been missed. If symptoms are escalating, do not wait for a sleep plan to work.
For non-urgent but persistent sleep disruption, the pathway can guide the appointment. Pain-dominant sleep loss belongs with the clinician managing the injury, physical therapy, or pain care. Concussion-pattern sleep changes belong with a clinician familiar with concussion recovery, especially when cognitive, vestibular, visual, or mood symptoms are present. Trauma-dominant insomnia belongs with CBT-I or trauma-informed mental health care, particularly when nightmares, avoidance, panic, or intrusive memories are keeping the nervous system activated.
Sleep recovery after an accident is not one track. If pain is driving awakenings, address injury recovery and the pain-sleep loop. If concussion signs fit, use concussion-specific sleep guidance and consider clinical evaluation. If trauma symptoms dominate, do not treat the problem as ordinary insomnia. The right intervention depends on which system is still keeping watch.
References
- The Importance of Sleep for Injury Recovery, OrthoCarolina, https://www.orthocarolina.com/media/the-importance-of-sleep-for-injury-recovery
- Sleep and Sleep Problems, Concussion Alliance, https://www.concussionalliance.org/sleep-and-sleep-problems
- Sleep Disorders in Traumatic Brain Injury, PMC, 2016, https://pmc.ncbi.nlm.nih.gov/articles/PMC4760657/
- What to Do After a Mild TBI or Concussion, CDC, https://www.cdc.gov/traumatic-brain-injury/response/index.html
- Sleep Problems and PTSD, VA National Center for PTSD, https://www.ptsd.va.gov/understand/related/sleep_problems.asp
- Sleep after trauma: the effect of sleep deprivation on intrusive emotional memories, Sleep, 2016, https://academic.oup.com/sleep/article/39/12/2123/2454067






Comments
Join the discussion with an anonymous comment.