For veterans seeking disability benefits for sleep apnea, the practical answer in July 2026 is still this: VA rates sleep apnea under Diagnostic Code 6847 at 0%, 30%, 50%, or 100%, and a prescribed CPAP or other breathing-assistance device has historically been the key evidence behind the 50% rating.[1] The proposed 2026 changes would move away from that CPAP shortcut toward a symptom-based structure, but those changes are not final as of July 2026.[2]
That distinction matters before anything else. A veteran using a CPAP today is not living under the proposed rule. A veteran preparing a claim should not assume the current rule will last forever, either. The useful move is to understand the rating system now, gather the evidence that proves both the diagnosis and the service connection, and check the final rule status before filing.
Current VA Sleep Apnea Ratings
The current rating table is unusually direct compared with many disability issues. It does not ask only whether the veteran snores, feels tired, or owns a CPAP machine. It asks how severe the condition is under VA’s rating language and what treatment or complications are documented.
| Current rating | What VA is looking for | Monthly compensation for a veteran alone |
|---|---|---|
| 0% | Diagnosed sleep apnea, but asymptomatic | $0 |
| 30% | Persistent daytime hypersomnolence | $552.47 |
| 50% | Requires use of a breathing assistance device such as CPAP | $1,132.90 |
| 100% | Chronic respiratory failure with carbon dioxide retention or cor pulmonale, or requires tracheostomy | $3,938.58 |
The dollar amounts above are for a veteran with no dependents. Spouses, children, dependent parents, and special monthly compensation can change the actual payment. VA compensation rates also change with cost-of-living adjustments, so the current VA.gov rate table should be checked before relying on any monthly amount.[3]
The 50% level is the reason sleep apnea claims get so much attention. In the current system, a CPAP prescription can move a veteran from a 30% rating to a 50% rating even when the machine helps control the airway at night. That has always been a little awkward medically. CPAP can prevent oxygen drops, reduce arousals, and improve daytime function, but it also adds a mask, hose, noise, cleaning routine, travel burden, and a nightly tolerance test that many patients struggle with.
The 100% rating is a different category of illness. It is not the rating for ordinary obstructive sleep apnea that is treated with CPAP. It is reserved for severe cardiopulmonary consequences such as chronic respiratory failure with carbon dioxide retention, cor pulmonale, or a tracheostomy requirement.[1]
Why Sleep Apnea Is Such a Large Veteran Claims Issue
Sleep apnea is not a fringe topic in the veteran population. A 2024 Sleep Health study reported sleep apnea in 21% of veterans compared with 9% of nonveterans.[4] Separately, AASM reporting on diagnosed sleep disorders among U.S. veterans found substantial increases across fiscal years 2000 through 2010 in a dataset of 9.7 million veterans, with branch differences that included Army veterans at 12.15%, Air Force veterans at 9.96%, and Navy veterans at 9.06% for diagnosed sleep apnea.[5]
That prevalence does not prove any individual claim. It does explain why the issue keeps appearing in bedrooms, clinics, C&P exams, and appeals. A veteran may have a formal diagnosis, a CPAP prescription, and years of exhaustion, but VA still has to answer a separate question: is the condition connected to service?
One veterans-law source, citing VA’s 2024 Annual Benefits Report, states that more than 659,000 veterans receive compensation for sleep apnea and that it is the second most common respiratory condition in VA compensation.[6] That figure is useful for scale, but it should be treated as a pointer back to the VA report rather than a substitute for checking the original benefits data.
What Evidence Proves the Sleep Apnea Claim
A sleep apnea claim usually needs three things: a current diagnosis, evidence of severity or treatment, and a nexus that connects the condition to military service or to an already service-connected disability. The diagnosis and the rating are not the same thing. A sleep study can prove the disorder exists; the rating evidence shows how VA should evaluate it; the nexus evidence explains why VA should compensate it.
- Diagnosis: A sleep study, usually in-lab polysomnography or a clinically accepted home sleep apnea test, documents obstructive, central, or mixed sleep apnea.
- Treatment evidence: CPAP, BiPAP, APAP, oral appliance, surgical history, settings, mask refills, adherence downloads, and follow-up notes can show what treatment was prescribed and whether symptoms persisted.
- Symptom evidence: Daytime sleepiness, morning headaches, witnessed apneas, impaired concentration, work problems, and drowsy driving concerns are relevant when they appear in medical records or credible lay statements.
- Nexus evidence: A medical opinion or service record pattern connects the current diagnosis to service, a service-connected condition, or a qualifying exposure theory.
The CPAP prescription should be easy to find in the record, not buried in a patient portal message. If the machine was issued through VA, the record may include durable medical equipment notes, sleep clinic follow-ups, pressure settings, and compliance downloads. If it was issued privately, the veteran may need the sleep study, prescription, equipment order, and recent treatment notes from the outside sleep clinic.
CPAP adherence deserves careful handling. General CPAP non-adherence has been reported in a wide range, from 46% to 83%, and veterans with PTSD, claustrophobia, panic symptoms, or other psychiatric comorbidities may face even more friction with mask tolerance.[2] Non-adherence does not make the sleep apnea unreal. It means the file should explain what was prescribed, what happened when the veteran tried to use it, and whether symptoms remained despite treatment.
The Three Service-Connection Routes
Most confusion starts when diagnosis and service connection get blended together. A veteran can have severe sleep apnea and still need evidence that VA recognizes as connected to service. The route matters because it shapes the evidence.
Direct service connection
Direct service connection is the cleanest path on paper and often the rarest in practice. It works best when service treatment records show sleep apnea symptoms, sleep-study referral, diagnosis, or treatment during active duty. Buddy statements from roommates, spouses, or unit members may help describe loud snoring, witnessed pauses in breathing, or severe daytime sleepiness during service, but lay statements usually cannot replace a medical nexus opinion.
Secondary service connection
Secondary service connection is often the more realistic path. It argues that sleep apnea is caused or aggravated by an already service-connected condition. Veterans-law sources commonly discuss sleep apnea secondary to PTSD, chronic rhinitis, sinusitis, GERD, asthma, medication-related weight gain, and other service-connected conditions, though the strength of any claim depends on the medical facts in that individual file.[6]
This is where the medical explanation has to do real work. A bare statement that “PTSD caused sleep apnea” is usually too thin. A stronger opinion explains the mechanism being claimed, the timing of diagnoses, the veteran’s treatment history, competing risk factors, and whether the service-connected condition caused the sleep apnea or aggravated it beyond its natural course.
Aggravation matters because some veterans already had risk factors before service or before a later diagnosis. The question may not be whether PTSD, rhinitis, GERD, or another condition single-handedly created the airway collapse. The question may be whether the service-connected condition made the sleep disorder worse, harder to treat, or more symptomatic in a way a clinician can explain.
Presumptive service connection and toxic exposure
Sleep apnea is not a presumptive condition under the PACT Act. That sentence is worth keeping plain because many veterans hear “burn pits,” “TERA,” and “presumptive” in the same conversation and reasonably assume sleep apnea has been added to the presumptive list. It has not.[7]
Toxic exposure can still matter as part of a medical theory. A veteran may raise a toxic exposure risk activity, burn pit exposure, particulate exposure, or respiratory history as evidence in a broader nexus argument. But that is not the same as presumptive approval. The file still needs a medical explanation that connects the exposure history to the diagnosed sleep apnea in that veteran’s case.[7]
How the Proposed 2026 Changes Would Alter the Rating Logic
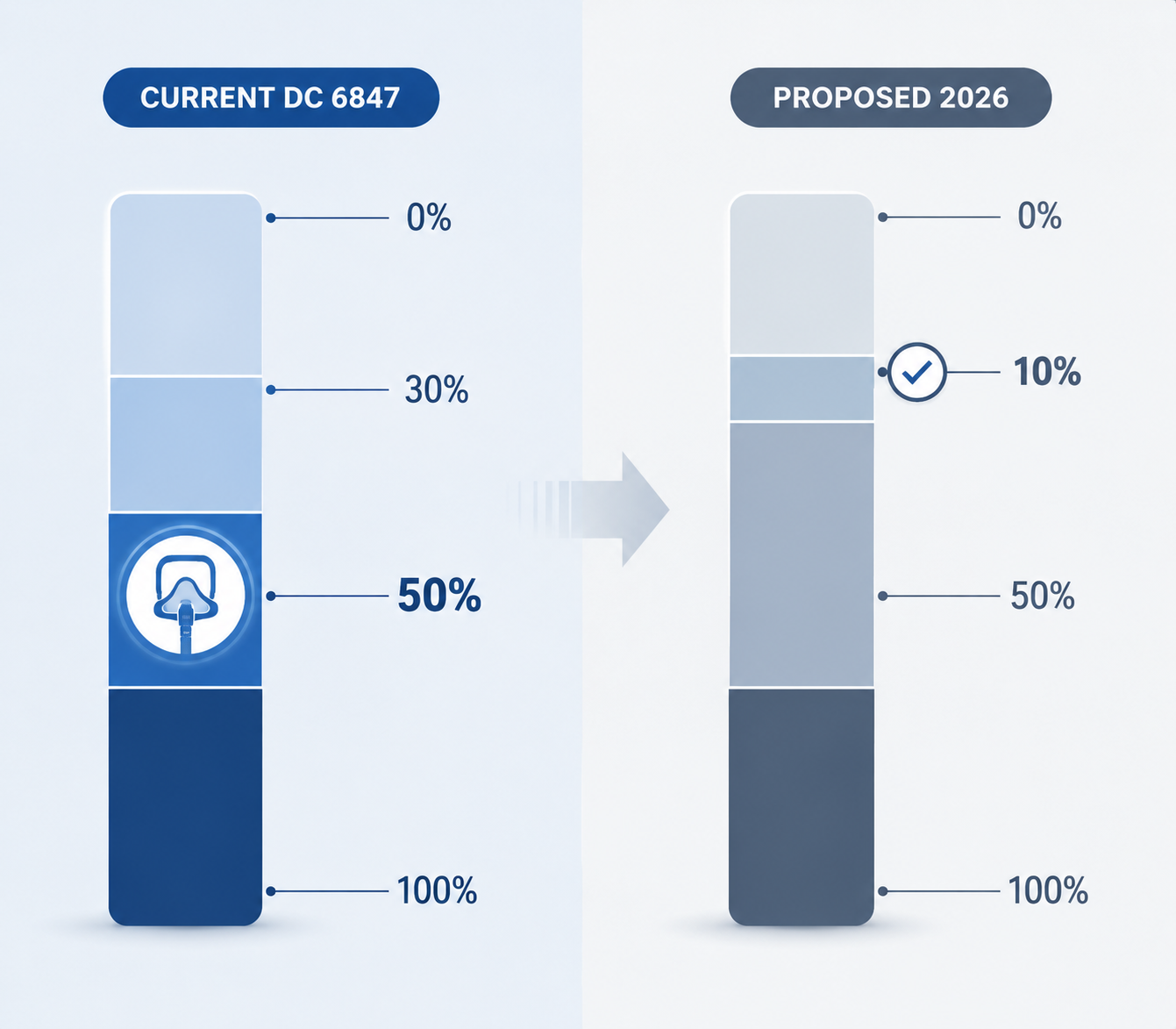
The proposed change is not a small wording edit. It would shift the sleep apnea rating away from the current “CPAP required equals 50%” structure and toward a framework based on treatment response and remaining functional impairment. The proposal was first published in February 2022, followed by a supplemental notice in September 2024, and no final rule is in effect as of July 2026.[2]
| Issue | Current DC 6847 | Proposed framework |
|---|---|---|
| Rating levels | 0%, 30%, 50%, 100% | 0%, 10%, 50%, 100% |
| CPAP effect | CPAP or similar breathing assistance device supports 50% | CPAP use alone would not automatically support 50% |
| Well-controlled symptoms with treatment | Often rated at 50% if CPAP is required | Could be rated at 10% under the proposed structure |
| Persistent symptoms despite treatment | May still fall under 50% if CPAP is required unless 100% criteria are met | Could support higher evaluation depending on documented residual impairment |
| Existing ratings | Current rules apply while active | Existing ratings are expected to be grandfathered under the proposal |
The controversial part is easy to see. A veteran who uses CPAP successfully may still have a real, lifelong sleep disorder, but under the proposed structure the machine’s success could lower the rating rather than support the current 50% level. From a sleep-health standpoint, that creates a strange tension: the treatment that keeps oxygen levels safer at night may also become evidence that the remaining disability is less severe.
That does not mean every future CPAP user would receive 10%. It means the automatic connection between prescribed PAP therapy and 50% would be broken. Veterans with persistent daytime symptoms, incomplete treatment response, serious complications, or unusual treatment barriers would need records showing what remains impaired after treatment, not merely proof that a machine was issued.
Grandfathering is the reason many veterans see urgency here. If the final rule follows the proposal, existing ratings would generally be protected from automatic reduction solely because the criteria changed.[2] That creates a filing window under current rules, but it is not a promise of approval. A claim still needs diagnosis, severity evidence, and service connection.
What a Veteran Should Verify Before Filing
The file should be built around evidence, not anxiety about a deadline that may move. Before filing or supplementing a claim, a veteran should verify the facts that VA will actually use.
- Confirm the diagnosis: Get the sleep study report, not just a portal note saying “sleep apnea.”
- Document prescribed treatment: Include CPAP, BiPAP, APAP, oral appliance, surgery, pressure settings, issue date, and follow-up notes.
- Show current severity: Record daytime sleepiness, residual symptoms, treatment intolerance, cardiopulmonary complications, and safety concerns when they are real and medically documented.
- Choose the correct nexus route: Direct, secondary, or exposure-related theory should match the record instead of being copied from another veteran’s case.
- Check the active rule: Current DC 6847 rules remain active as of July 2026, but VA should be checked for any final rule before submission.
- Check current compensation rates: The amounts in this article use VA rates effective Dec. 1, 2025 and may change after COLA updates.[3]
A smartwatch alert, snoring app, or partner’s observation can be useful for deciding to seek care, but it is not the same as a diagnostic sleep study. Likewise, mouth taping, sedatives, alcohol, or improvised “sleep hacks” are not substitutes for treating a breathing disorder during sleep. If sleep apnea is suspected, the first benefit step is still a clinical one: get properly tested.
For veterans who already have a diagnosis and a CPAP prescription, delaying only because the proposed 2026 rule is uncertain is hard to justify. The current rules are active now. The proposed rules are not final. Documentation quality matters under either system.
References
- How VA Rates Sleep Apnea, Hill & Ponton
- Proposed VA Sleep Apnea Rating Changes, Telemedica
- VA Disability Compensation Rates, VA.gov
- Sleep Health study on sleep apnea prevalence among veterans and nonveterans, PubMed, 2024
- Prevalence of Sleep Disorders Among US Veterans, AASM
- VA Secondary Conditions to Sleep Apnea, CCK Law
- Sleep Apnea & Toxic Exposure Guide, Trajector Medical






Comments
Join the discussion with an anonymous comment.