If you are in the second or third trimester, awake again after the pillows, side-sleeping, warm bath, and phone-off routine have already failed, the useful question is not whether a pregnancy sleep aid is “safe” in the abstract. The useful question is which options have pregnancy-specific safety data, which ones only look reassuring because they are sold over the counter, and which ones belong off the self-treatment list.
The confusion is predictable. By the third trimester, up to 80% of pregnant people report insomnia symptoms, and Cleveland Clinic notes that more than 60% report insufficient sleep late in pregnancy despite a general target of 8 to 10 hours a night.[1] Sleep Foundation, citing NIH data, reports that more than 90% of pregnant people occasionally treat sleep difficulties with OTC sleep aids.[2] That does not mean all of those products are equivalent. It means many exhausted people are standing in the same aisle, trying to decode brand names, active ingredients, and risk signals at a point when sleep loss is no longer a minor inconvenience.

The Evidence Tiers, Before the Fine Print
Most medication safety data in pregnancy is imperfect because pregnant people are often excluded from randomized drug trials. That does not make all evidence useless. It makes the hierarchy matter more: human pregnancy data counts more than animal data, regulated drugs are not the same as loosely regulated supplements, and a product used in a pregnancy-approved combination is not in the same category as a sleep gummy with a comforting label.
| Tier | What Belongs Here | Evidence Judgment | How to Use This Information |
|---|---|---|---|
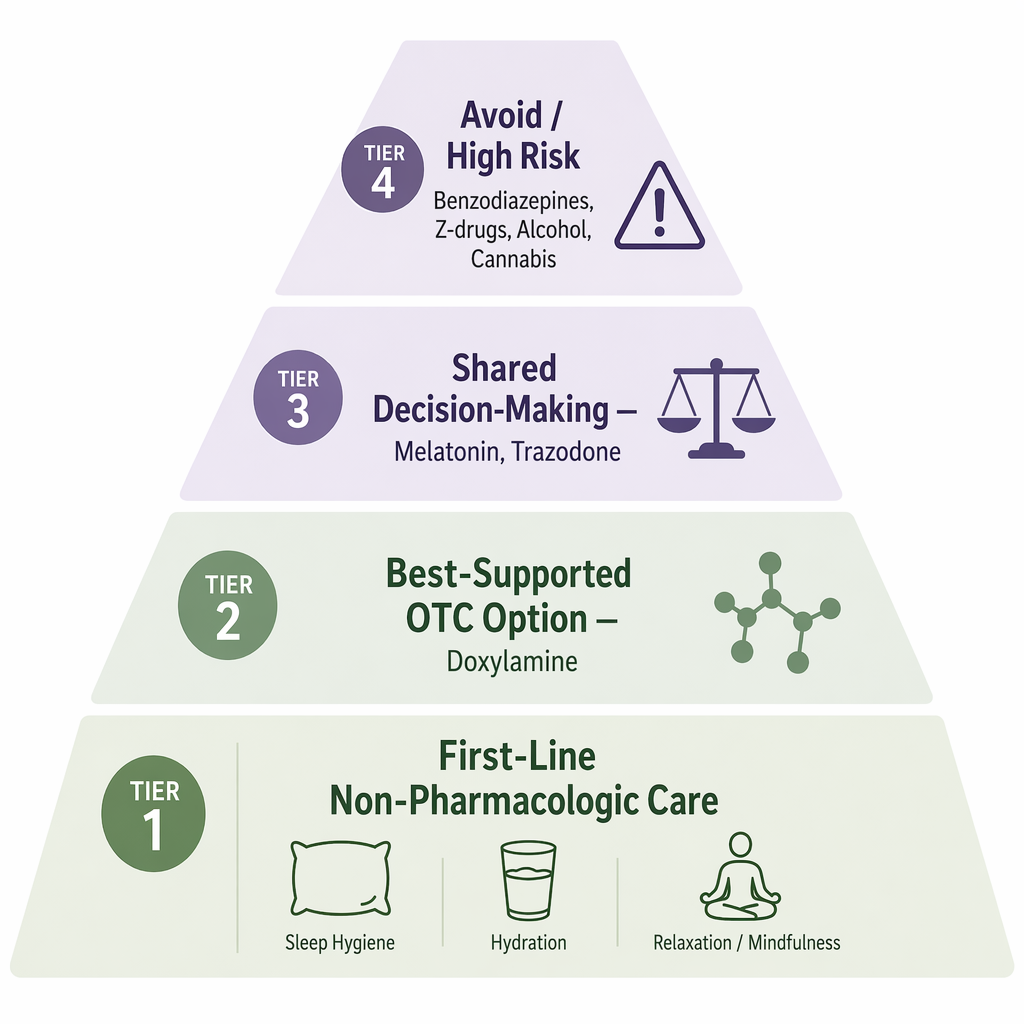
| Tier 1 | CBT-I, sleep scheduling, stimulus control, positioning, reflux or restless legs management when relevant | First-line because there is no medication exposure; clinical sources recommend non-drug care before sleep aids when symptoms allow.[2] | Use as the baseline, especially for ongoing insomnia rather than a single bad night. |
| Tier 2 | Doxylamine; diphenhydramine for occasional use | Doxylamine has the strongest pregnancy-specific OTC sleep-aid safety record; diphenhydramine is generally considered acceptable occasionally but has less pregnancy-specific data.[2][3] | Bring the active ingredient, dose, and frequency to your OB-GYN rather than relying on a brand name. |
| Tier 3 | Melatonin; trazodone | Evidence is unresolved or clinician-dependent; these are shared-decision options, not casual self-selection choices.[4] | Discuss why you need it, what else has failed, and whether your pregnancy has additional risk factors. |
| Tier 4 | Benzodiazepines, Z-drugs such as zolpidem or eszopiclone, barbiturates, alcohol, cannabis/CBD, most herbal supplements | Known risks, concerning associations, or insufficient pregnancy safety data make these avoid or high-risk categories.[2] | Do not start these for sleep in pregnancy without direct clinician management; some should be avoided outright. |
This is not a treatment ladder. For step-by-step escalation, the companion pregnancy sleep aid treatment ladder is the better map. This guide is narrower: it sorts the evidence behind the options people commonly consider.
Why Non-Drug Care Still Gets First Place
Non-drug care does not deserve first place because pregnancy insomnia is imaginary or because exhausted people need one more lecture about pillows. It gets first place because it can improve sleep without adding a fetal medication exposure. Cognitive behavioral therapy for insomnia, a consistent sleep window, stimulus control, adjusted evening light exposure, and treatment of triggers such as reflux, pain, anxiety, or restless legs can matter more than another over-the-counter label.
Sleep Foundation’s pregnancy sleep guidance places non-pharmacologic strategies first, including CBT-I-style behavioral approaches, sleep environment changes, and management of pregnancy-related discomforts.[2] For trimester-specific causes—urination, reflux, fetal movement, hip pain, shortness of breath, restless legs—the fuller breakdown is in Insomnia During Pregnancy: Causes by Trimester and Evidence-Based Treatment.
Still, “try sleep hygiene” is not an answer to severe insomnia. Poor sleep during pregnancy has been linked with gestational diabetes, preeclampsia, preterm birth, longer labor, C-section, and postpartum depression.[1][2] Those associations do not prove that every short night causes those outcomes, but they do mean persistent insomnia is a health issue worth treating, not a character flaw to endure. For a deeper risk review, see Insomnia During Pregnancy: What the Research Says About Risks.
Tier 2: The OTC Options With the Clearest Pregnancy Safety Story
Doxylamine Is the Standout, Not a Free-for-All
Doxylamine is the active ingredient in Unisom SleepTabs, and it is also used with pyridoxine, or vitamin B6, in a pregnancy-approved nausea and vomiting treatment. That second fact is why doxylamine stands apart from many OTC sleep aids: it has been repeatedly studied in pregnant populations for a pregnancy-related indication, not merely borrowed from general adult insomnia use.
StatPearls’ 2026 doxylamine monograph describes doxylamine 25 to 50 mg at bedtime as safe and not teratogenic, and identifies it as the most studied OTC sleep aid in pregnancy.[3] That is an unusually concrete statement in a field where many products can only claim “limited data” or “ask your clinician.” It still does not turn doxylamine into an automatic nightly solution for every pregnant person.
The dose range is context for a conversation with an OB-GYN, not a prescription from an article. Sedating antihistamines can cause next-day grogginess, dry mouth, constipation, dizziness, and impaired alertness. Those side effects matter more in late pregnancy, when falls, nighttime bathroom trips, driving, childcare, and work obligations are not theoretical. If you are comparing products, check the active ingredient rather than the brand: some Unisom products contain doxylamine, while other sleep products may contain diphenhydramine or a different ingredient. The ingredient-level guide to OTC sleep medicine ingredients can help with that label check.
Doxylamine also deserves a practical boundary: stronger evidence is not the same as unlimited use. If insomnia is happening most nights, the question shifts from “Can I take something tonight?” to “Why is this becoming the pattern, and what plan keeps me functional without stacking sedation?” The deeper doxylamine guide covers who should be cautious and what to ask about frequency: Doxylamine as a Sleep Aid: Safety, Dosage, and Who Should Avoid It.
Diphenhydramine Is Not Identical Just Because It Is Another Antihistamine
Diphenhydramine, the active ingredient in Benadryl and many “PM” products, is also a sedating antihistamine. ACOG-informed consumer medical sources generally describe it as safe for occasional use in pregnancy, and Sleep Foundation includes it among OTC options sometimes used during pregnancy.[2] The important distinction is that diphenhydramine does not have the same pregnancy-specific sleep-aid evidence story as doxylamine.
That difference is easy to lose in a store aisle. Both can make you sleepy. Both are old antihistamines. Both are available without a prescription. But doxylamine’s safety record is strengthened by its role in a pregnancy-approved nausea/vomiting combination and extensive human pregnancy data; diphenhydramine is more accurately described as an option many clinicians consider acceptable for occasional use, with less pregnancy-specific data behind it.[2][3]
The practical move is simple: if you are considering either one, bring the bottle or a photo of the Drug Facts panel to your prenatal visit. Ask about the exact active ingredient, the dose, whether it interacts with anything else you take, and whether your symptoms suggest another treatable cause such as restless legs, reflux, anxiety, or sleep apnea.
Tier 3: The Gray Zone Where Casual Reassurance Does the Most Damage
Melatonin Has Conflicting Guidance, Not a Settled Green Light
Melatonin is where many pregnancy sleep aid articles get sloppy. It is a hormone sold as a supplement, which means consumers often experience it as “natural” and therefore low-risk. Pregnancy guidance does not support that shortcut. Sleep Foundation summarizes the conflict plainly: ACOG-linked guidance advises discussing melatonin with an OB-GYN, the NHS advises against use in pregnancy because of insufficient safety data, and a Brazilian scoping review concluded that melatonin is “probably safe” during pregnancy and breastfeeding.[4]
Those statements cannot be flattened into one answer. “Probably safe” from a scoping review is not the same as a regulatory approval for insomnia in pregnancy. “Discuss with your OB-GYN” is not the same as “take it because it is over the counter.” And “insufficient data” is not proof of harm. The honest category is shared decision-making: what is the severity of insomnia, what else has failed, what dose is being considered, what other conditions are present, and what does the clinician think given the specific pregnancy?
Mechanistic research also complicates the picture rather than resolving it. A review on melatonin’s role in pregnancy describes melatonin as biologically active in pregnancy-related processes, including placental and fetal development pathways.[5] That is a reason to study it carefully, not a reason to treat a supplement bottle as harmless.
Trazodone Belongs With Clinician-Guided Decisions
Trazodone is a prescription medication often used off-label for insomnia in nonpregnant adults. In pregnancy, it should not be treated as a consumer sleep aid. MGH Center for Women’s Mental Health discusses insomnia treatment during pregnancy as a stepped clinical decision, where medication choices depend on symptom severity, psychiatric history, and the risk of leaving insomnia untreated.[6]
That matters because trazodone may be considered in some situations—particularly when insomnia overlaps with mood symptoms or when other options have failed—but the decision belongs inside prenatal and mental health care, not in a late-night comparison of “natural vs prescription.” The question is not whether trazodone is morally better or worse than an OTC sleep aid. The question is whether the benefit-risk profile makes sense for this patient, at this point in pregnancy, with this medical history.
Tier 4: Options to Avoid or Treat as High-Risk
Some categories do not need a long debate. Benzodiazepines, barbiturates, Z-drugs such as zolpidem and eszopiclone, alcohol, cannabis/CBD, and most herbal supplements are not routine pregnancy sleep aids. Sleep Foundation’s pregnancy sleep aid review flags prescription sedatives and substances such as alcohol and cannabis as concerning because of documented or potential risks, including preterm birth, low birth weight, neonatal withdrawal, developmental concerns, or inadequate pregnancy safety data.[2]
- Benzodiazepines: require clinician management because of fetal and neonatal concerns, including withdrawal risk.
- Z-drugs such as zolpidem or eszopiclone: prescription-only options with pregnancy risk concerns; not casual self-treatment.
- Barbiturates: high-risk sedatives that are not appropriate as routine pregnancy sleep aids.
- Alcohol: not a sleep treatment in pregnancy, even if it makes someone drowsy.
- Cannabis, CBD, and most herbal sleep supplements: avoid self-treatment because pregnancy safety data is inadequate or concerning.
This is also where “natural” marketing becomes actively unhelpful. Herbal blends may combine multiple sedating compounds, omit pregnancy-specific testing, and vary in strength. A supplement can be poorly studied and biologically active at the same time.
How to Bring This to Your OB-GYN Without Starting From Scratch
The most useful prenatal conversation is specific. “I can’t sleep” is true, but it does not give your clinician enough to work with. Bring the pattern: how many nights per week, whether you cannot fall asleep or cannot stay asleep, how long it has lasted, what you have tried, whether you snore or wake gasping, whether your legs feel restless, whether reflux or pain is waking you, and what you need to be able to do the next day.
- Bring the product label, not just the brand name.
- Ask whether the active ingredient is doxylamine, diphenhydramine, melatonin, or something else.
- Ask whether your pregnancy has any reason to avoid sedating medication, such as fall risk, breathing concerns, other sedatives, or a high-risk condition.
- Ask what frequency changes the plan from occasional rescue use to an insomnia treatment strategy.
- Ask when symptoms should trigger evaluation for sleep apnea, restless legs, anxiety, depression, reflux, or pain.
For many people, the most evidence-grounded OTC discussion point will be doxylamine, not because it is automatically right, but because it has the clearest pregnancy-specific safety record among common OTC sleep aids. Diphenhydramine may be reasonable occasionally when a clinician agrees. Melatonin and trazodone belong in shared-decision territory. Benzodiazepines, Z-drugs, barbiturates, alcohol, cannabis/CBD, and most herbal sleep supplements should not be used as casual pregnancy insomnia fixes.
That is the standard worth keeping: start with non-drug care when possible, do not pretend untreated insomnia is harmless, and match every sleep aid to the strength of pregnancy-specific evidence rather than to how reassuring its packaging sounds.
References
- Pregnancy Insomnia — Cleveland Clinic — https://my.clevelandclinic.org/health/diseases/pregnancy-insomnia
- Sleep Aids to Take While Pregnant — Sleep Foundation — https://sleepfoundation.org/pregnancy/pregnancy-sleep-aid
- Doxylamine — StatPearls — 2026 — https://ncbi.nlm.nih.gov/books/NBK551646/
- Can You Take Melatonin While Pregnant? — Sleep Foundation — https://sleepfoundation.org/melatonin/pregnancy
- The Role of Melatonin in Pregnancy — PMC — https://pmc.ncbi.nlm.nih.gov/articles/PMC9775355/
- Treatment of Insomnia During Pregnancy — MGH Center for Women's Mental Health — https://womensmentalhealth.org/posts/treatment-of-insomnia-during-pregnancy/


Comments
Join the discussion with an anonymous comment.