

What Is Restless Legs Syndrome?
Restless Legs Syndrome (RLS) — also known as Willis-Ekbom disease — is a neurological sleep-movement disorder characterized by an uncomfortable, irresistible urge to move the legs, most often appearing at rest and intensifying in the evening and nighttime hours. The sensations are internal to the limb rather than on the skin surface, and are commonly described as crawling, creeping, pulling, throbbing, aching, or electric.
RLS is more common than many people realize. Epidemiological estimates place prevalence at 7–10% of US adults, with the RLS Foundation citing more than 10 million affected adults in the United States. The variation between these figures reflects differences in diagnostic stringency and how frequently symptoms must occur to qualify. Women are at least twice as likely to have RLS as men, and risk increases with age — though the condition can appear at any point in adulthood.
The Five Diagnostic Criteria: How RLS Is Identified
RLS is diagnosed clinically using the five criteria established by the International Restless Legs Syndrome Study Group (IRLSSG). No polysomnography (sleep study) or blood test is required to make the diagnosis. All five criteria must be present simultaneously.
- An irresistible urge to move the legs — usually accompanied by uncomfortable sensations deep within the limb.
- Symptoms begin or worsen at rest — sitting or lying down triggers or intensifies the urge.
- Movement provides partial or complete relief — walking, stretching, or rubbing the legs reduces the sensation, at least temporarily.
- A circadian pattern: symptoms are worse in the evening or nighttime — the urge is minimal or absent during the morning and peaks after sunset.
- The symptoms are not explained by another condition (exclusion of mimics) — leg cramps, positional discomfort, swelling, arthritis, and habitual foot tapping must be ruled out as the primary cause.
Primary vs. Secondary RLS: What Triggers the Condition
RLS is classified as either primary (idiopathic) or secondary, depending on whether an identifiable underlying cause is present.
Primary RLS has no single identifiable cause and often runs in families. A positive family history is common, and several genetic variants have been associated with elevated risk, suggesting a heritable component.
Secondary RLS is triggered or substantially worsened by an identifiable underlying condition. Identifying a secondary cause matters clinically because treating the underlying condition can improve or resolve RLS symptoms. Common secondary triggers include:
- Iron deficiency (the most common and clinically significant secondary cause)
- Pregnancy, particularly in the third trimester
- Chronic kidney disease
- Peripheral neuropathy
- Parkinson's disease
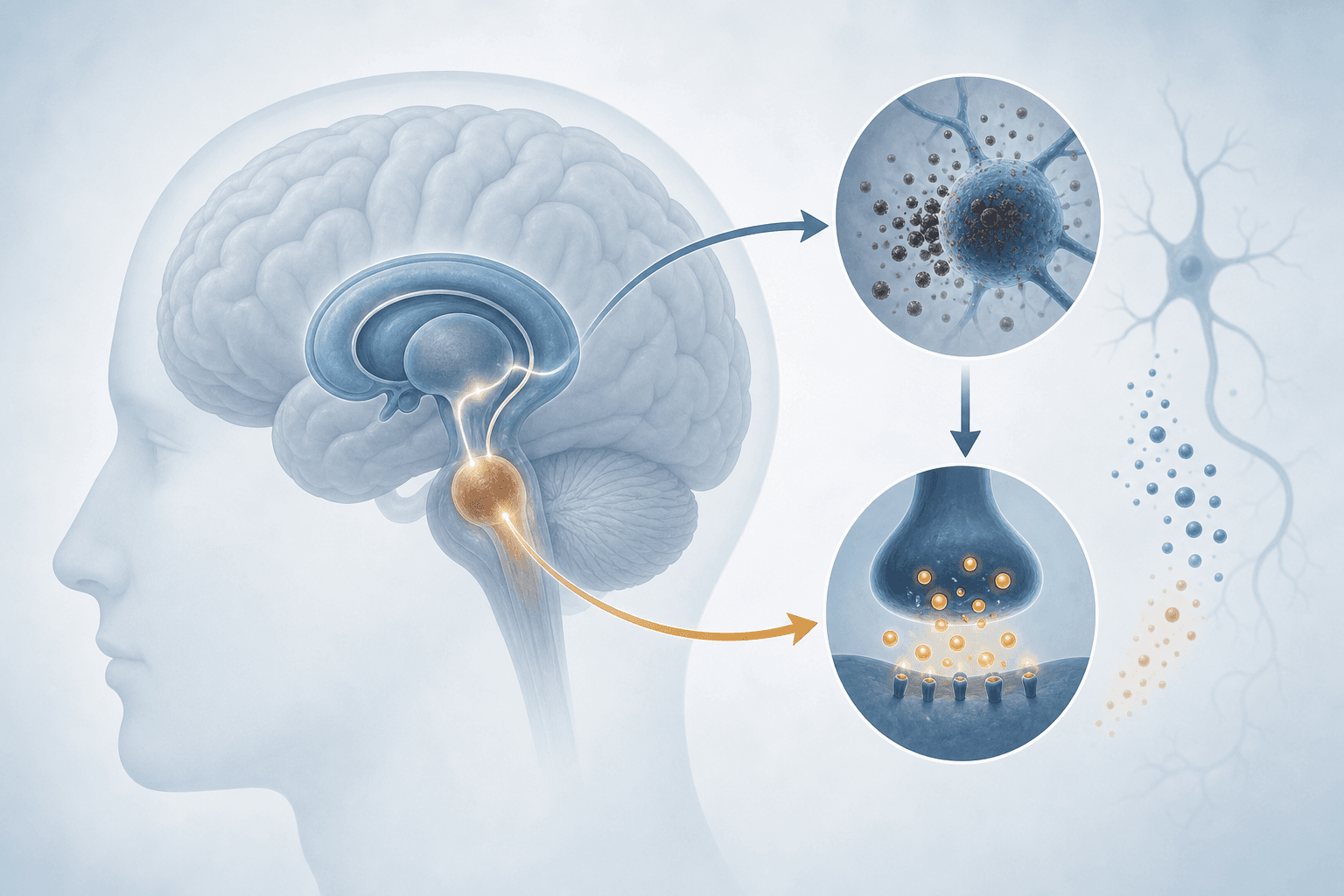
The Brain Behind the Urge: Iron, Dopamine, and the Basal Ganglia
The leading biological explanation for RLS is the iron-dopamine hypothesis. The basal ganglia — a group of brain structures involved in movement regulation — depend on dopamine to function properly. When dopaminergic signaling in the basal ganglia and substantia nigra is disrupted, the brain loses some of its ability to regulate movement efficiently, producing the characteristic urge that defines RLS.
Iron is essential to dopamine synthesis and transport. Brain-specific iron deficiency impairs dopaminergic signaling even when the rest of the body's iron stores appear adequate. As the Cleveland Clinic notes, iron can be low in the brain despite normal blood levels.
Research reviewed in the Mayo Clinic Proceedings confirms that RLS patients can have lower than normal iron stores in specific brain regions even without systemic iron deficiency or anemia — and that iron therapy can be beneficial in these patients. This is why ferritin testing is now a universal recommendation for all RLS patients, regardless of whether a systemic deficiency is suspected.
How RLS Disrupts Sleep
Because RLS symptoms peak in the evening and at night, the condition directly targets the window when sleep is supposed to begin. The urge to move makes lying still difficult, delaying sleep onset and fragmenting sleep maintenance throughout the night.
Approximately 80% of people with RLS also experience periodic limb movements of sleep (PLMS) — repetitive, involuntary leg movements that occur during sleep, often without the person's awareness. PLMS and RLS are related but distinct conditions with separate diagnostic classifications. PLMS independently disrupts sleep architecture by producing arousals and micro-awakenings that reduce sleep quality even when the person does not fully wake up.
Polysomnographic data from peer-reviewed research provides a concrete picture of how significant this disruption is:
| Sleep Measure | RLS Patients | Controls |
|---|---|---|
| Total sleep time | 326.3 minutes | 383.3 minutes |
| Sleep efficiency | 73.2% | 86.6% |
| Mean nocturnal awakenings | 12.2 | 7.4 |
The daytime consequences extend beyond fatigue. Survey data cited in research on RLS sleep effects found that adults at risk for RLS were more likely to sleep under six hours per night, take more than 30 minutes to fall asleep, report daytime fatigue in over 55% of cases, and miss work or make errors due to sleep-related impairment.
The 2025 AASM Treatment Hierarchy: A 180-Degree Reversal
The 2025 AASM clinical practice guidelines (Winkelman et al., Journal of Clinical Sleep Medicine, January 2025) represent a fundamental shift in how RLS is treated. The guidelines explicitly reverse the 2012 recommendations that placed dopamine agonists at the top of the treatment hierarchy. In their place, the new framework prioritizes iron evaluation and gabapentinoid medications.
"The focus has moved away from dopamine agonists, which were historically first-line therapy, toward iron supplementation and gabapentinoid medications." — Dr. Andy Berkowski, guideline co-author, speaking to NeurologyLive
The guidelines organize treatment into three sequential steps. Each step should be addressed before moving to the next.
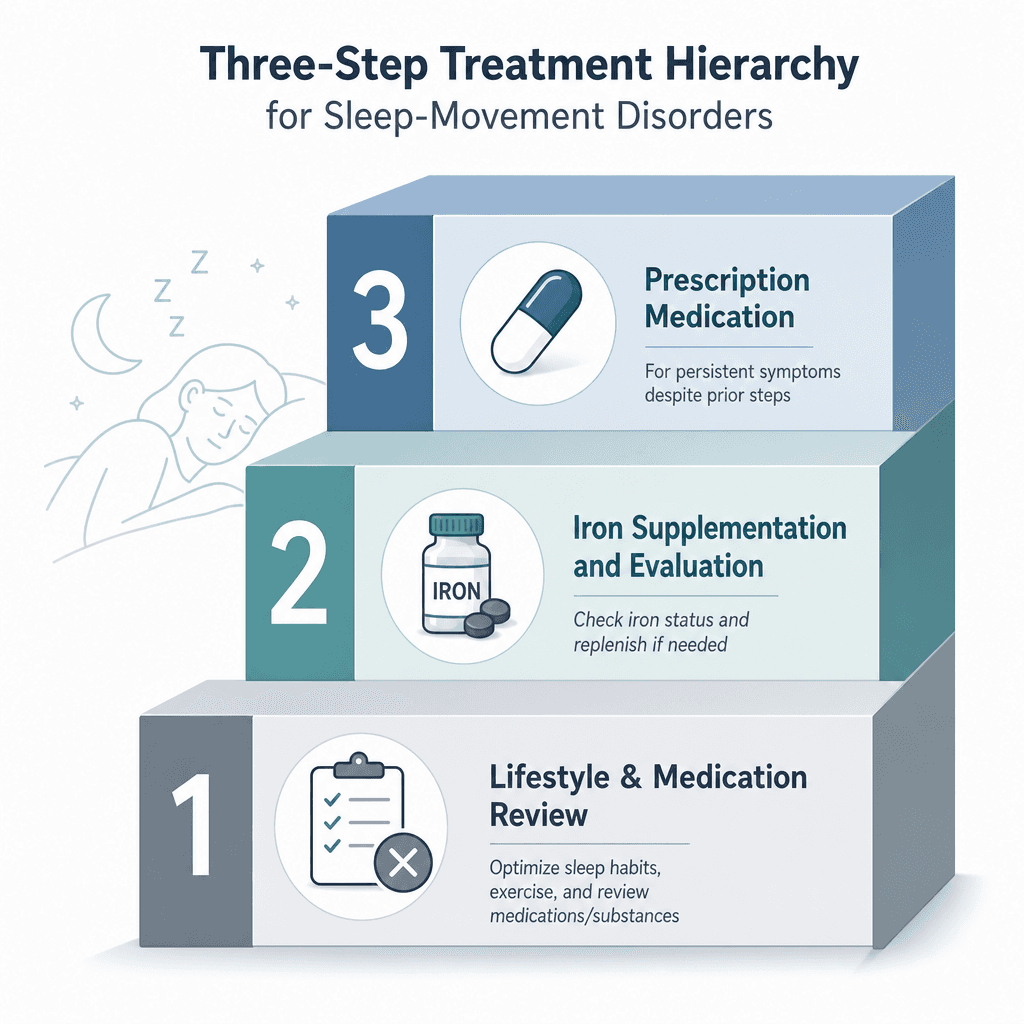
Step 1: Address Exacerbating Factors
Before any medication is prescribed, the guidelines recommend reviewing and modifying factors that are known to trigger or worsen RLS. These include:
- Alcohol and caffeine
- Antihistamines (including over-the-counter sleep aids)
- Most antidepressants (SSRIs, SNRIs, and tricyclics)
- Antiemetics and antipsychotics (e.g., metoclopramide)
- Untreated obstructive sleep apnea (OSA)
Step 2: Evaluate and Treat Iron Deficiency
Ferritin testing is now universally recommended for all RLS patients, regardless of whether systemic iron deficiency is suspected. The treatment approach depends on the result:
| Ferritin Level | Transferrin Saturation | Recommended Iron Treatment |
|---|---|---|
| Below 75 µg/L | Below 20% | Oral ferrous sulfate (guideline-supported) |
| 75–100 µg/L | Any | IV ferric carboxymaltose (strong recommendation) |
| Above 100 µg/L | Normal | Iron supplementation not indicated by ferritin alone |
Step 3: Pharmacotherapy
When iron correction and factor removal are insufficient, the guidelines recommend gabapentinoid medications as first-line pharmacotherapy. The AASM's official announcement specifies that gabapentinoids are preferred because they are not associated with the augmentation of RLS symptoms observed with dopaminergic agents.
| Medication / Class | 2025 AASM Recommendation | Augmentation Risk |
|---|---|---|
| Gabapentin enacarbil | Strong recommendation FOR | None |
| Gabapentin | Conditional recommendation FOR | None |
| Pregabalin | Conditional recommendation FOR | None |
| Low-dose opioids | Conditional recommendation FOR | Low (different mechanism) |
| Pramipexole | Conditional recommendation AGAINST | High (~8%/year) |
| Ropinirole | Conditional recommendation AGAINST | High (~8%/year) |
Augmentation: Why Dopamine Agonists Fell From First-Line
Augmentation is the central reason for the 2025 treatment reversal. It is a paradoxical worsening of RLS symptoms that develops with long-term dopamine agonist use — not an improvement, but a progressive deterioration that the medication itself causes.
The hallmarks of augmentation include:
- Symptoms beginning earlier in the day than they did before treatment started
- Spread of symptoms to the arms or other body parts
- Shorter duration of relief from each dose
- Paradoxical worsening of symptoms when the dose is increased
A 2025 case report in Cureus illustrates the pattern: a 61-year-old woman with 20 years of RLS treated with ropinirole developed symptoms that spread to her arms and worsened paradoxically each time her dose was increased. Resolution required a gradual supervised taper.
The incidence figures are striking. According to data reviewed in the Mayo Clinic Proceedings, augmentation with pramipexole or ropinirole occurs at an annual rate of approximately 8% per year, with a cumulative incidence of 40–70% over a 10-year period. Among the roughly two-thirds of treated RLS patients who have been prescribed dopamine agonists, a quarter to half develop augmentation — and the remainder remain at ongoing risk.
"We no longer recommend [dopamine agonists] as a first-line treatment, and maybe not even the second." — Dr. John Winkelman, who led the AASM task force, quoted in Harvard Health
Medications That Can Trigger or Worsen RLS
Medication review is Step 1 of the 2025 treatment hierarchy — not an afterthought. Several common drug classes are known to initiate or significantly worsen RLS symptoms, and identifying a culprit medication can sometimes resolve the condition without any additional treatment.
| Drug Class | Examples | Clinical Note |
|---|---|---|
| Antihistamines | Diphenhydramine, doxylamine (OTC sleep aids) | Among the most common triggers; OTC sleep aids are a frequently overlooked cause |
| Antidepressants (most) | SSRIs, SNRIs, tricyclic antidepressants | Bupropion is a notable exception and may be less likely to worsen RLS |
| Antiemetics | Metoclopramide | Dopamine-blocking mechanism directly exacerbates RLS |
| Antipsychotics | Many first- and second-generation agents | Dopamine-blocking mechanism; review with prescribing clinician before any changes |
Special Populations: Pregnancy and Perimenopause
Pregnancy
RLS is significantly more common during pregnancy than in the general adult population. Up to 30% of pregnant women experience RLS symptoms, with the highest prevalence in the third trimester. In most cases, symptoms resolve in the weeks following delivery.
The treatment picture during pregnancy is substantially more constrained. Most pharmacological options for RLS — including gabapentinoids and iron supplementation beyond standard prenatal levels — require careful clinical evaluation before use. Non-pharmacological approaches and close monitoring are typically the first response.
Perimenopause
Hormonal changes during perimenopause can trigger or worsen RLS in women who were previously unaffected. For a full discussion of how RLS presents and is managed in the context of perimenopausal sleep disruption, see the dedicated article on restless legs syndrome and perimenopause insomnia.
When to See a Doctor — and What to Bring
Not every person who experiences occasional leg discomfort at night needs a clinical evaluation. But several situations clearly warrant a conversation with a physician or sleep specialist:
- Symptoms are frequent enough to interfere with falling asleep or staying asleep
- Daytime fatigue, impaired concentration, or missed obligations are resulting from poor sleep
- You suspect a current medication — including an OTC antihistamine or antidepressant — may be triggering or worsening symptoms
- You are currently taking pramipexole or ropinirole and want to discuss whether your treatment aligns with the 2025 AASM guidelines
- You are pregnant and experiencing RLS symptoms that are disrupting sleep
Coming prepared to the appointment will make the evaluation more productive. Consider bringing:
- A symptom diary noting when symptoms occur, how long they last, what makes them better or worse, and how they affect sleep
- A complete medication list — including OTC products such as antihistamine sleep aids, allergy medications, and any supplements
- Family history of RLS — if a parent or sibling has been diagnosed or describes similar symptoms
- Specific questions about ferritin testing — ask whether your ferritin has been tested recently and what the result was in relation to the 75 µg/L threshold
- Questions about current treatment alignment — if you are on a dopamine agonist, ask how your current regimen compares to the 2025 AASM recommendations and what alternatives your clinician would consider





Comments
Join the discussion with an anonymous comment.